Chapter 2 Canalplasty for Exostoses of the External Auditory Canal and Miscellaneous Auditory Canal Problems
 Videos corresponding to this chapter are available online at www.expertconsult.com.
Videos corresponding to this chapter are available online at www.expertconsult.com.
The etiology of these benign growths of the tympanic bone is strongly associated with the frequency and severity of exposure to cold water.1 Frequently, these lesions are found in surfers, swimmers, or other individuals with frequent cold water exposure over several years. A widely held belief based on clinical information is that exostoses occur primarily during the years of growth, with their proliferation being enhanced or perhaps even caused by exposure to cold water during this period. This belief tends to be supported by historical information from patients with exostoses, who almost always indicate that they swam in cold water during their youth.2–4 This historical information is strongly corroborated by the high incidence of exostoses in avid surfers who spend hours in the water almost daily. In our clinical experience, this problem occurs almost exclusively in men, who are more likely than women of the same age to have had frequent cold water exposure during their youth.
EXOSTOSES OF THE EXTERNAL AUDITORY CANAL
Preoperative Preparation
Site Preparation
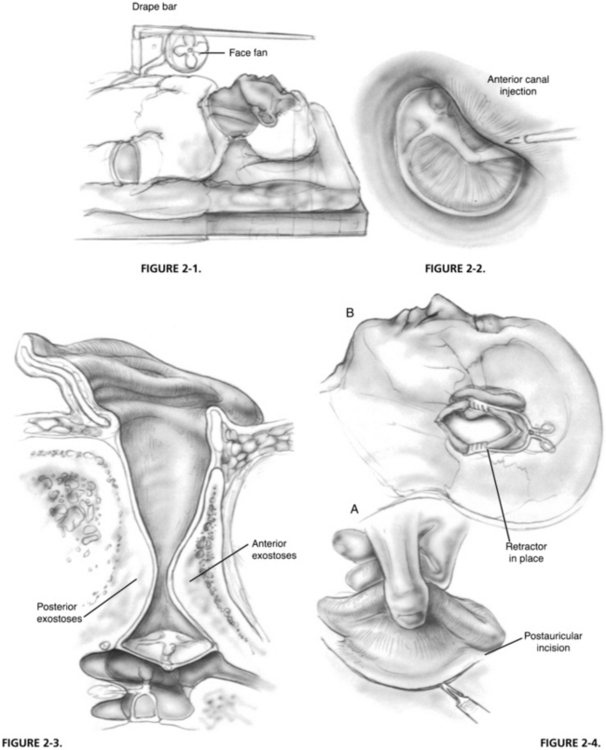
The hair is shaved behind the ear to a distance of approximately 1.5 inches posterior to the postauricular fold. The auricle and the periauricular and postauricular areas are scrubbed with povidone-iodine (Betadine) solution or chlorhexidine gluconate (Hibiclens) for iodine-allergic patients. A plastic drape is placed over the area with the auricle and the postauricular area exteriorized through the opening in the drape. This drape is placed over an L-shaped bar that is fixed in the rail attachment of the operating table (Fig. 2-1). For patients under local anesthesia with sedation, a small, low-volume office fan is attached to the bar to provide a gentle cooling breeze to the patient’s face during the procedure. The plastic drape forms a canopy, allowing the patient to see from under the drape and reducing the feeling of claustrophobia. In addition, a foam earpiece from an insert speaker is put into the opposite ear. The earpiece is connected to a compact disk player and input microphone that allows the patient to listen to relaxing music and provides a pathway to converse with the patient, if desired.
Analgesia
It is important not only to achieve analgesia, but also to maximize canal hemostasis with injections into the external auditory meatus. Using 2% lidocaine (Xylocaine) with 1:20,000 epinephrine solution in a ringed syringe with a 27 gauge needle, a classic quadratic injection is made such that each injection falls within the wheal of the previous injection. Another useful injection is an anterior canal injection, which is made with the bevel of the needle parallel to the bony wall of the external meatus (Fig. 2-2). In a patient with extensive exostoses, this injection is usually made into the lateral base of a large anterior sessile osteoma. After insinuation of the needle, it is advanced a few millimeters, and a few drops are injected extremely slowly. The solution infiltrates medially along the anterior canal wall and provides some analgesia to the auriculotemporal branch of CN V, which is usually unaffected by the quadratic injection and adds to the hemostasis anteriorly. The postauricular area is infiltrated with 2% lidocaine with 1:100,000 epinephrine solution mixed with equal parts of 0.5% bupivacaine.



