Purpose
To report a distinct type of calcification in hydrophilic intraocular lenses in complicated, traumatized eyes with a history of intraocular gas use.
Design
Observational case series.
Methods
Three cases of hydrophilic intraocular lens (IOL) opacification confined to the pupillary area are reported from clinical practice in London, UK. Clinical details and analysis of the explanted intraocular lenses are provided with environmental scanning electron microscopy images and x-ray energy-dispersive spectroscopy results.
Results
All cases were associated with use of intraocular gas in complicated traumatized eyes, and had central areas of IOL opacification over the pupillary zone, confined to the anterior surface of the IOL. Analysis of the lenses showed the opacified areas to be composed of calcium and phosphate.
Conclusion
The areas of opacification in all 3 hydrophilic IOLs were attributable to calcification. We postulate that intraocular gas use and the altered blood-aqueous barrier of these complicated traumatized eyes co-act to trigger secondary IOL calcification. Further experimental testing is needed to confirm this clinical association.
Intraocular lens (IOL) opacification is a serious but rare problem that may necessitate exchange of the lens. It has been observed with most IOL materials and has usually been traced to a specific defect in the manufacture of the IOL or its polymer. A rare snowflake pattern of opacification has been reported in polymethylmethacrylate (PMMA) IOLs, some types of early silicone IOLs were seen to develop brown discoloration, and microvacuoles (glistenings) can be seen with a variety of IOL materials, but most commonly with the Acrysof (Alcon Laboratories) hydrophobic material.
The most numerous and severe cases of opacification, however, have been attributable to calcification of hydrophilic IOLs, which has led to large numbers of explantations with the Hydroview (Bausch and Lomb Surgical, Rochester, New York, USA), Aqua-Sense (Ophthalmic Innovations International, Ontario, California, USA), MemoryLens (IOL Tech, La Rochelle, France) and SC60B-OUVT IOLs (Medical Developmental Research Inc, Clearwater, Florida, USA). With some of these IOLs the calcification occurred in a specific pattern. The Hydroview lens developed a fine, very superficial calcification on or in the surface of both anterior and posterior optical surfaces, even extending under the cover of the area of anterior rhexis and optic contact. The opacification progressed in many patients to obscure fundus detail and reduce vision, requiring explantation.
In contrast, the Aqua-Sense lens developed an entirely different pattern of intraocular calcification, again some months after implantation, in which the central “nuclear” region of the IOL became opaque, separated from the optic surfaces by a clear zone and partially extending into the optic-haptic junction. This was thought to be attributable to incomplete binding of the ultraviolet blocking agent. Calcification in other types of IOLs has not been so uniformly characterized, but the MemoryLens has been reported to develop widespread calcification on the optic surface and the SC60B-OUVT IOL deeper subsurface opacification limited to the optic area. Calcification has been confirmed by histologic stains of explanted lenses specific for calcium and by elemental analysis with x-ray energy-dispersive spectroscopy showing the presence of calcium and phosphate in opacified areas with all these IOLs. It is clear that calcification can occur in a characteristic pattern with specific hydrophilic IOLs.
In this report we describe 3 cases of IOL opacification in hydrophilic IOLs that are characterized by an unusual pattern of calcification limited to the superficial anterior IOL surface in the pupillary area. All cases occurred in eyes that had undergone multiple complicated intraocular procedures with a common theme of intraocular gas usage, which we hypothesize could be causal.
Cases
Case 1
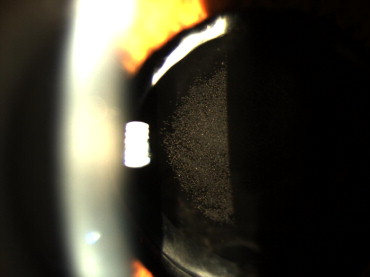
A 45-year-old man presented to our eye emergency service with decreased vision and glare symptoms in his left eye. The patient had previously suffered blunt trauma to the same eye and had undergone uneventful cataract surgery with implantation of a hydrophilic IOL 4 years previously at a different unit. One year previously he had also undergone a vitrectomy with cryotherapy and sulfur hexafluoride (SF 6 ) injection for retinal detachment. Visual acuity was 0.2 logMAR (20/32) and 0.8 logMAR (20/125) at 9% contrast at presentation, and on slit-lamp examination there was central IOL opacification consisting of fine granular areas confined to the pupillary zone of the superficial anterior IOL surface, which appeared to consist of small punctuate circular lesions that were almost confluent ( Figure 1 ). The IOL was slightly decentered in the capsular bag and the opacification was centered on the pupil rather than the IOL. He subsequently underwent an IOL exchange. At surgery an attempt was made to polish or remove the opacified area, without success or any change in the appearance. Pre-existing damage to the zonules in the inferonasal quadrant was seen, but surgery was otherwise unremarkable. One month postoperatively the best-corrected acuity had improved to 0.0 logMAR (20/20) with an improvement in contrast.
Review of the case notes showed both cataract extraction and lens implantation of an 18.5-diopter Rayner C-flex (Rayner Ltd, Hove, UK) IOL and the vitrectomy, cryotherapy, and SF 6 injection had been unremarkable, with no intraoperative complications. Intracameral agents used during cataract surgery are listed in the Table . Subconjunctival cefuroxime was used for endophthalmitis prophylaxis. Intracameral agents used during the vitrectomy were balanced salt solution and cefuroxime.
| Case | IOL | POH | Ophthalmic Surgery | Systemic Disease | Intracameral Agents | Gas Used |
|---|---|---|---|---|---|---|
| 1 | Rayner C-flex 570C | Blunt trauma Cataract Retinal detachment | Phaco Vitrectomy + cryo + SF 6 | Hypertension | 1% Lidocaine Healon Cefuroxime BSS | Intravitreal SF 6 |
| 2 | Bausch & Lomb Akreos | Fuchs heterochromic cyclitis Cataract Glaucoma | Phaco Trabeculectomy – C 3 F 8 injection into AC Bleb needling | Diabetes | HPMC 2% lidocaine Epinephrine | 20% C 3 F 8 in AC |
| 3 | Bausch & Lomb Akreos | Fuchs corneal endothelial dystrophy Cataract | Combined DSAEK & phaco Air & SF 6 injection to AC Repeat DSAEK | Nil | Healon HPMC Miochol BSS Provisc | 20% SF 6 in AC Air in AC |
Case 2
A 74-year-old patient was noted to have central superficial opacification of his IOL confined to the pupillary area at a routine postoperative visit. He had an ophthalmic history of Fuchs heterochromic cyclitis and glaucoma and had undergone phacoemulsification on the same eye 9 months previously. The cataract surgery had been unremarkable; intracameral agents used are listed in the Table and subconjunctival betnesol and cefuroxime were given at the end of surgery. An 18.5-diopter hydrophilic acrylic IOL (Akreos Adapt; Bausch and Lomb Inc, Rochester, New York, USA) was inserted in the bag and there were no intraoperative complications. A trabeculectomy with mitomycin C 0.2 mg was performed 5 months later because of failure of medical treatment (G latanoprost, Azopt, brimonidine) to control intraocular pressure. Six weeks later 20% perfluoropropane (C 3 F 8 ) was injected into the anterior chamber to control postoperative hypotony and a bleb needling procedure was performed another 8 weeks later.
A lens exchange was subsequently performed. Surgery was uneventful with insertion of the new IOL into the capsular bag. Visual acuity improved to 0.2 logMAR (20/32) unaided with an intraocular pressure of 8 mm Hg with no topical treatment.
Case 3
A 72-year-old diabetic man with Fuchs corneal endothelial dystrophy had previously had a penetrating keratoplasty in the right eye. In February 2007 he underwent combined phacoemulsification with lens implantation and Descemet stripping endothelial keratoplasty (DSAEK) to the left eye. Phacoemulsification surgery was unremarkable and a 19.5-diopter Akreos Adapt lens was inserted into the capsular bag. Viscoelastics used are listed in the Table . Miochol, balanced salt solution, and SF 6 20% were also injected into the anterior chamber during the procedure. Other medications used included topical atropine and subconjunctival gentamycin and betnesol.
Two further injections of gas were used to refloat the graft (once with air and once with SF 6 ) in the first few weeks after the procedure. He underwent a repeat DSAEK with 20% SF 6 in August 2007 and a complete gas fill was noted in the operative notes. Healon (Abbott Medical Optics Inc, High Wycombe, United Kingdom) and Provisc (Alcon Labs, Hemel Hempsted, United Kingdom) viscoelastic were used during this procedure. Approximately 1 month later, during a postoperative visit, a central circular area of opacification of the IOL, very similar to the previous cases, was noted, which was symptomatically significant enough to warrant an IOL exchange a few months later. Postoperative vision improved to 0.0 logMAR (20/20) 2 months later.
Methods
The explanted IOLs from Cases 1 and 2 were immersed in saline and subsequently analyzed at the Centre for Ultrastructural Analysis at Guy’s Hospital, London with a FEI Quanta FEG environmental scanning electron microscope with a back-scattered electron detector and energy-dispersive x-ray spectrometer for elemental analysis. The explanted IOL in Case 3 was analyzed at the Moran Eye Center (FEI, Hillsboro, Oregon, USA) with alizarin red staining.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


