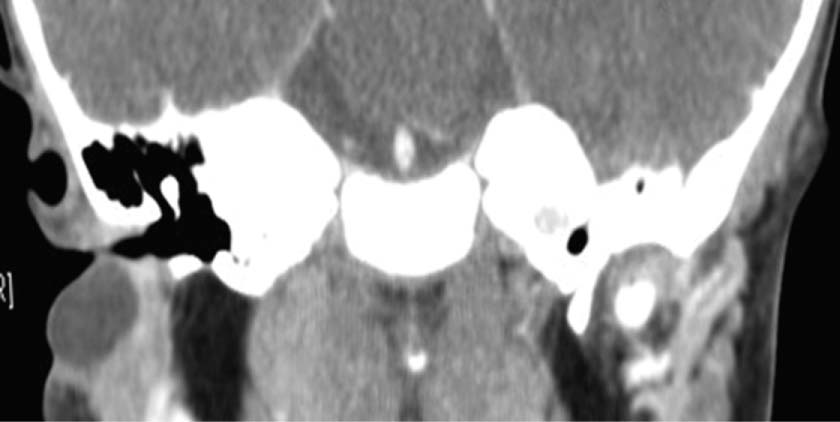
68 A 1-year-old boy presented with a right ear lesion obstructing the external auditory canal and intermittent drainage from a pit in the right cheek just inferior to the ear lobule (Fig. 68.1). He had no history of hearing loss, renal disease, or other systemic illness. Facial nerve function was intact and symmetric. The ipsilateral tympanic membrane and remainder of the head and neck examination were normal. Computed tomography (CT) imaging demonstrated a well-defined, low-attenuating mass anterior to the floor of the right cartilaginous external auditory canal. The mass measured 15 × 9 mm and was partially surrounded by parotid tissue (Fig. 68.2). 1. The differential diagnosis of a pediatric neck mass can be divided into congenital and acquired lesions. Congenital masses can further be divided into midline and lateral anomalies. Acquired lesions can be benign or malignant. Table 68.1 illustrates the differential diagnosis of pediatric neck masses. 2. Knowledge of the embryology of branchial development is essential for understanding the pathway that an anomaly will follow. The greatest head and neck embryonic development occurs in the first 8 weeks. There are six branchial arches (Fig. 68.3). Between these arches are clefts externally that are lined with ectoderm and pouches internally that are lined with endoderm. The fifth branchial arch degenerates. Each arch has an associated nerve, artery, cartilaginous bar, and muscle. The sternocleidomastoid muscle (SCM) derives from the cervical somites posterior and inferior to the branchial arches (Table 68.2). Fig. 68.1 Right ear with cystic mass obstructing the external auditory canal. Fig. 68.2 Coronal computed tomography imaging demonstrating cystic mass inferior to external auditory canal. 3. Branchial anomalies related to arch development include cysts, sinuses, and fistulae. Cysts are lined by mucosa or epithelium, have no external opening, and arise from embryonic rests trapped inside developing tissue. Sinuses result from the incomplete closure of branchial pouches and clefts, and they communicate with a single body surface, either the skin or pharynx. Fistulae also result from the incomplete closure of pouches or clefts; however, they communicate with two body surfaces.
Branchial Arch Anomaly
History
Differential Diagnosis—Key Points

Congenital | |
Midline | Lateral |
Thyroglossal duct cyst | Branchial cleft cyst |
Dermoid/epidermoid cyst | External laryngocele |
Teratoma | Pseudotumor of infancy (fibromatosis coli) |
Plunging ranula | Thymic cyst |
Lymphatic/vascular malformation | Lymphatic/vascular malformation |
Hemangioma | Hemangioma |
Normal thyroid gland |
|
Acquired | |
Benign | |
Infectious or inflammatory:reactive lymphadenopathy | |
Sialadenitis | |
Abscess | |
Granulomatous (atypical mycobacteria, cat-scratch, toxoplasma, sarcoidosis) | |
Neoplastic: lipoma, neurofibroma, pilomatrixoma, benign mixed tumor | |
Malignant | |
Lymphoma (Hodgkin, non-Hodgkin), rhabdomyosarcoma, thyroid carcinoma, salivary tumors, neuroblastoma, histiocytosis (Langerhans) | |
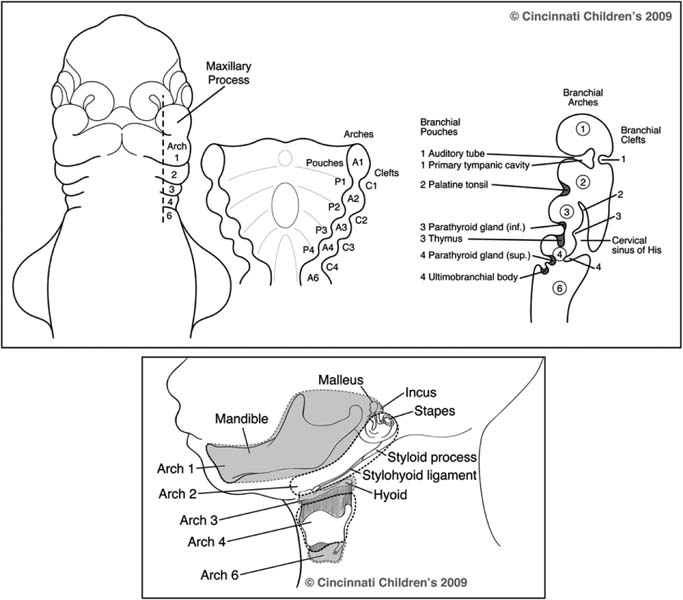
Fig. 68.3 Embryology of branchial arches, clefts, and pouches (superior) and the structures from which they derive (inferior).
4. Traditional teaching holds that the path of a branchial anomaly can be predicted based on knowledge of branchial arch embryology. Cysts, sinuses, and fistula tracts course posterior-medial-deep to other derivatives of their own branchial arch, and anterolateral and superficial to the derivatives of the arch behind them. The origin of third and fourth branchial anomalies is controversial.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


