40 Brainstem Auditory Implants
The auditory nerve is often compromised after removal of vestibular schwannomas (VSs) in individuals with neurofibromatosis type 2 (NF2). Such individuals have benefited from signing and lipreading; however, these methods do not restore useful hearing sensations. Development of the auditory brainstem implant (ABI) solved this problem by providing auditory sensations from electrical stimulation of the cochlear nucleus complex.1,2 The multichannel version of the ABI (Nucleus, Cochlear Corporation, Englewood, Colorado, United States) successfully completed U.S. Food and Drug Administration (FDA) clinical trials in July 2000 and received approval for commercial release. The use of the ABI now has expanded to other pathologies that compromise the eighth nerve.
This chapter provides an overview of how the ABI is used and the perceptual performance that is achieved. Since 1979, this work has been underway in more than 265 patients with various implementations of the ABI at House Ear Institute (HEI, Los Angeles, California, United States). The first 25 patients received the initial single-channel ABI; the next 71 patients received the eight-electrode multichannel ABI; and subsequent patients have received a 21-electrode multichannel ABI system (the Nucleus ABI24).
A research device using penetrating electrodes for cochlear nucleus stimulation was also developed and evaluated in FDA clinical trials at HEI.
Previous papers summarizing ABI implantation and management of patients with NF2 have been reported elsewhere.3–5
History of Development
The first application of the ABI was by Dr. William House and Dr. William Hitselberger in 1979 in a patient who lost hearing after removal of a second-side VS. The patient insisted that she serve as a test case in the application of an ABI device. The electrode was a simple ball type, and electrical stimulation was supplied by a modified body-worn hearing aid. The patient received useful auditory sensations but also developed some leg sensations and the device was temporarily removed. Huntington Medical Research Institute (HMRI, Pasadena, California, United States) redesigned the electrode array with two (and later three) platinum ribbon electrodes on a mesh carrier, and this provided more stable hearing performance in 25 implantees through the early part of 1992. Modified 3M/House type cochlear implant (CI) processors provided the electrical stimulation and gave recipients sound sensations that were useful in communication, particularly in combination with lipreading. As of this writing, the first ABI recipient continues to use her single-channel ABI daily with benefit. The multiple electrodes (two to three on the original array) provided an opportunity to evaluate the efficacy of multichannel stimulation with ABIs, and this led to the development and successful use of the present multichannel ABI. More than 1000 individuals worldwide have now benefited from this technology, including some infants as young as 9 months of age.
Patient Selection
There is a high prevalence (90%) of bilateral VS in individuals with NF2.6 The lifespan of such individuals has been significantly prolonged by effective treatment of these and other tumors associated with NF2. Quality of life has also improved for such individuals, even though perceptual performance, particularly for those with NF2, has not generally reached typical CI levels.
Ideally, individuals with NF2 are identified and receive treatment early to maximize chances of hearing preservation. Often, however, tumors have progressed to the stage where hearing preservation is unlikely and an ABI is recommended.
FDA approval of the ABI states that it is appropriate for use in individuals who are at least 12 years of age. Preoperative audiologic criteria do not exist, because surgical removal of the VS typically results in loss of any remaining hearing. ABI candidates are individuals undergoing surgical removal of first or second-side VS or patients who already have had both VSs removed. First 90% of implantees have received auditory sensations from their ABIs, but the remaining 9% have not, primarily because of anatomic problems. In many such cases, implantation on the first-side tumor has provided a second opportunity for these individuals to achieve a functioning system when their second acoustic tumor was removed. FDA approved this change in the ABI investigational protocol in circa 1996.
Since FDA approval, the application of the ABI has expanded beyond individuals with NF2. The fact remains, however, that the ABI may not be for everyone with nonviable auditory nerves. With the NF2 population, we learned that several nonimplant-related factors can influence ABI benefit: general health, vision, social activity level, support, and anatomic status (as seen on magnetic resonance imaging [MRI]). Patient age can also be a factor, with teenage implantees often presenting some additional maturity-related challenges in addition to some of the same factors as those well beyond their teenage years.2 And, because the ABI generally works best in conjunction with lipreading, severely visually impaired recipients have generally shown less benefit, although several visually challenged patients have received substantial benefit and become excellent ABI users. The bottom line is that candidates for ABIs should be apprised of the possible effects of these factors on their potential to benefit from the device and they should demonstrate understanding and acceptance of these factors.
Preoperative Evaluation and Counseling
The goal of ABI preoperative counseling should be to inform the patients realistically, yet demonstrate that the ABI can be of great benefit given time and experience. This is an opportunity to help patients prepare for the loss of hearing after tumor removal and lay the groundwork that will help them acclimate to a new way of hearing with the ABI. A frank and thorough explanation of what is involved in using and improving with an ABI is necessary. Failing to achieve this understanding can delay satisfactory adjustment to the ABI. A primary reason this is so important is that ABIs result in a wide range of auditory performance and, in many cases, lower levels than typical CI performance. Most patients in our experience start with a basic level of auditory performance, and improvement can be significantly influenced simply by the number of hours the ABI is used on a daily basis. Performance can be improved greatly for as long as 10 years after implantation, but generally at a slower pace than in CIs.
A high level of motivation to make maximal use of whatever sounds the ABI provides will contribute greatly to long-term benefit with the device.2 Postoperative follow-ups are also a necessary part of optimizing ABI performance. During these sessions, changes that normally occur in response to stimulation can be accommodated by reprogramming the ABI sound processor. Counseling preoperatively provides an opportunity to emphasize the necessity of compliance with the follow-up protocol and to address any motivation issues. Some patients may also benefit from special counseling to help them cope with deafness and the other disabilities that can be related to NF2. This may help minimize their effect on adjusting to and regularly using the ABI.
Another issue that should be discussed preoperatively is the strong possibility that nonauditory sensations such as tingling or dizziness may be experienced either alone or in combination with auditory sensations. Patients should be informed that these are a normal part of ABI programming and that they must communicate the type and magnitude of these sensations to the audiologist. Patients should also be informed that it is usually possible to substantially reduce or eliminate nonauditory sensations and that mild side effects can often disappear on their own. Cautious optimism is an excellent tone to maintain throughout preoperative counseling. This has eliminated unpleasant surprises during the initial stages of ABI use and has worked well in properly setting the stage for postoperative rehabilitation. Adjustment to ABIs is an ongoing process fostered by a clear understanding of the contributing factors and typical time frame for progress.
For the successful treatment and management of individuals with NF2, the participation of an experienced, skilled, and coordinated multidisciplinary team is essential. The success of an ABI program depends on the contribution of each team member. Chief among these are the surgeon’s skill and experience in removing acoustic tumors, preserving necessary structures, and accurately placing the electrode array. Proper identification of the implant site depends on expert electrophysiologic monitoring support. Also, ABI recipients could not benefit from their implants without audiologic expertise in properly programming the speech processor and optimizing performance. Learning to use and adapt to an ABI, even under ideal circumstances, takes longer than in cochlear implantation. It is an ongoing process, and new recipients should be encouraged that performance almost always improves greatly with time and experience. Periodic reprogramming of the sound processor is absolutely necessary for improvement to occur. Patients who have difficulty complying with these follow-up visits can expect less benefit from their ABIs over the long term.
Device
The first ABI recipient was implanted with a CI ball-type electrode by Hitselberger et al.7 Subsequent patients received a fabric mesh electrode array (2 × 8 mm) specifically designed for the cochlear nucleus complex. In 1992, an eight-electrode multichannel ABI system was developed in a collaborative effort by HEI, Cochlear Corporation, and HMRI. Subsequently, the number of electrodes was increased to those in the present Nucleus ABI24 system shown in Fig. 40.1A. The electrodes (0.7 mm in diameter) are mounted in a flexible perforated silicone and mesh substrate that allows the electrode to conform to the surface of the cochlear nucleus and remain in a stable position. Pulsatile stimulation (2400 pulses/s/electrode) is provided by the ABI24 receiver stimulator that is capable of using several advanced sound processing strategies.
The ABI24 system includes the Nucleus Freedom sound processor and a transmitter coil (Fig. 40.1B). The processing strategy approved for use with ABIs by the FDA is the Nucleus SPEAK (spectral peak) strategy. This strategy is also well established as effective in CIs, and it analyzes input sound frequencies and transmits information about spectral maxima by sequentially activating electrodes on the array. Several parameters can be varied over a wide range, including number of spectral maxima, the sequence and number of electrodes that can be activated, the stimulus rate, levels, and pulse durations, as well as available speech processing strategies (including the Nucleus Advanced Combination Encoder [ACE]).
The basic procedure of the Freedom processor is as follows: 21 contiguous analysis filters split the input sound spectra and then deliver the output to selectable electrodes on the array. ABI recipients must be individually tested regarding any electrode-specific pitch percepts, and scaling and ranking of this parameter is a major part of sound processor programming. The general goal is to link low-frequency sounds with electrodes that sound lower in pitch and likewise with higher frequency sounds. This sound processing strategy also optimizes speech and environmental sound perception in CIs; however, the highly homogeneous physiological structure of the cochlea makes the process relatively straightforward with CIs. A much more complex relationship exists with an ABI because of individual variations in cochlear nucleus anatomy, neuronal survival, electrode placement, and other factors. Given that nonauditory sensations are also more common, programming ABI speech processors can take longer than programming CIs.

Figure 40.1 (A) The Nucleus ABI24 auditory brainstem implant receiver/stimulator with 21-electrode surface array (and remote ball ground electrode) for the cochlear nucleus complex. (B) The Nucleus Freedom auditory brainstem implant speech processor with a transmitter coil.
Printed with permission from: Cochlear Corporation, Centennial, Colorado, United States.
The penetrating ABI (PABI) system (Cochlear Corporation, Englewood, Colorado, United States) developed for research application8 has two electrode arrays with a 10- (or 12-) electrode surface array, plus a penetrating-type array with 8- (or 10-) needle microelectrodes. It uses the same external sound processor equipment and strategies as the regular surface ABI, except that stimulation can occur on either (or both) type of electrode arrays in the same individual. There are special considerations for programming PABIs that are in addition to the usual considerations with regular surface electrodes. Not the least of these is lower charge density safety limits created by the very focused electrical stimulation generated at the tips of the needle electrodes. The type and magnitude of nonauditory sensations also can vary from the norm.
Anatomic Considerations
The targets for the placement of the ABI array are the dorsal and ventral cochlear nuclei, with probable emphasis on the ventral portion. The nuclei are hidden by the cerebellar peduncle, so surface landmarks are used to identify their location; however, these structures may be distorted by tumor. The area of the lateral recess of the fourth ventricle is shown in a drawing depicting a histological section in Fig. 40.2. Important landmarks are the terminus of the sleevelike lateral recess forming the foramen of Luschka, inferior to the root of the glossopharyngeal (ninth) nerve, and superior to the foramen of the vestibulocochlear and facial nerve roots.
Normally, the intact choroid plexus marks the entrance to the lateral recess (foramen of Luschka) and the taenia obliquely traverses the roof of the lateral recess, marking the surface of the ventral cochlear nucleus. A large VS may distort the lateral surface of the pons and medulla and obscure or complicate identification of these structures. Even so, often the eighth nerve stump may be traced to the mouth of the lateral recess, or the ninth cranial nerve can also point to the opening of the recess. A concavity sometimes visualized between the eighth and the ninth nerve should not be confused with the introitus of the recess.
The dorsal and ventral cochlear nuclei are found within the lateral recess and on its superior aspect. Historically, we have positioned the electrode array well within the recess to optimize positional stability. Insertion depths that are too deep or too shallow, however, can result in electrodes at the ends of the array not eliciting auditory sensations. Electrophysiological testing during placement can help achieve an optimal location. The ventral cochlear nucleus is the main relay for the eighth nerve input and is probably the primary source of auditory sensations, although some stimulation undoubtedly occurs via activation of the dorsal cochlear nucleus.
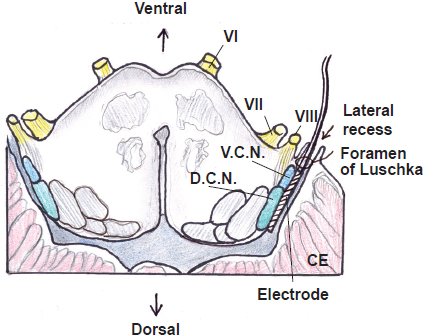
Figure 40.2 Drawing showing a histological section showing the area of the lateral recess of the fourth ventricle, cranial nerves VI, VII, VIII, and the relationship between ventral cochlear nucleus (VCN), dorsal cochlear nucleus (DCN), inferior cerebellar peduncle, and vestibular nuclei. The cerebellum (CE) is also shown.
Printed with permission from: Bhalani Medical Book House. Fayad J, Brackmann DE, Otto S. Auditory brainstem implants. In: Kirtane MV, Brackmann DE, Borkar DM, de Souza C, eds. Comprehensive Textbook of Otolaryngology: Diagnosis, Management and Operative Techniques. Mumbai, India: Bhalani Medical Book House; 2010:581; Fig. 37.2.
Surgical Considerations
Good access for tumor removal and lateral recess exposure is achieved using the translabyrinthine craniotomy, and a typical translabyrinthine acoustic tumor removal process is followed except that recording electrodes are placed for monitoring electrically evoked auditory brainstem responses (EABRs) and any activity from cranial nerves VII and IX. As shown in Fig. 40.3, a c-shaped postauricular incision is used and the ABI receiver/stimulator is placed in a pocket in the temporal area. Intravenous antibiotics, for example, cefuroxime (3 g; Zinacef), are administered prophylactically on induction of anesthesia. Intraoperative monitoring of the EABR helps verify that the electrode array is placed accurately and slight adjustments have been used to minimize nonauditory electrical activity. The placement of EABR monitoring electrodes is done as follows: subdermal needle electrodes are inserted at the vertex of the head, over the seventh cervical vertebrae, and at the hairline of the occiput. For monitoring nonauditory activation, electromyographic activity is monitored from the facial nerve in the standard fashion,8 and with bipolar electrodes inserted in the ipsilateral pharyngeal (soft palate) muscle to monitor any activity from cranial nerve IX. Stimulation of the electrodes on the array occurs after the receiver/stimulator has been secured and the electrode array is placed. Activation occurs using a transmitter coil placed over the receiver/stimulator antenna. EABRs from cochlear nucleus stimulation with biphasic pulses is different from responses from acoustic stimulation or CI electrical stimulation. Interpretation from an experienced electrophysiologist is necessary to provide useful feedback to the neurosurgeon about the electrode array placement.
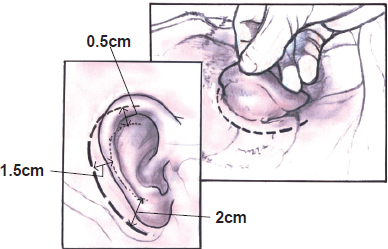
Figure 40.3 c-shaped incision currently used for the placement of an auditory brainstem implant. The incision starts behind the pinna and is approximately 2 cm away from the postauricular fold at the level of the mastoid tip.
Printed with permission from: Bhalani Medical Book House. Fayad J, Brackmann DE, Otto S. Auditory brainstem implants. In: Kirtane MV, Brackmann DE, Borkar DM, de Souza C, eds. Comprehensive Textbook of Otolaryngology: Diagnosis, Management and Operative Techniques. Mumbai, India: Bhalani Medical Book House; 2010:581; Fig. 37.2.
Implantation Procedure
Through a translabyrinthine craniotomy, the tumor dissection is completed in the normal fashion. Subsequent to complete removal of the tumor and hemostasis, an area suitable for location of the internal receiver/stimulator is selected and temporalis muscle is elevated and excised off the parietal skull. As shown in Fig. 40.4
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


