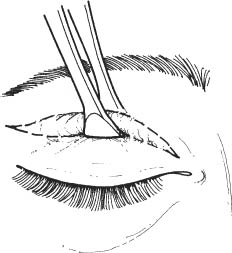
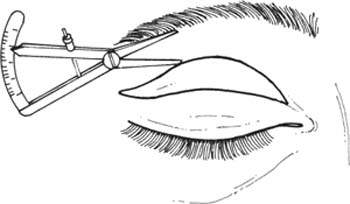
52 See Chapter 3. 1. Complete lid and eye examination to determine detailed operative plan. 2. Measure position of lid crease. (If lid crease is indistinct or malpositioned, placement of supratarsal fixation sutures may be indicated.) 3. Evaluate presence and location of herniated orbital fat. (Cosmetically unacceptable fat prolapse is often located medially.) 4. Evaluate brow position. (A brow lift may be required if brow droop is present.) 5. Evaluate lid position. (A ptosis procedure may be indicated in combination with the blepharoplasty.) 6. Check corneal sensation, corneal staining, Bell phenomenon, and Schirmer test to evaluate potential impact of any postoperative lagophthalmos. 7. Perform a visual field examination to document any field cut (usually superior) secondary to dermatochalasis if required by insurance. 8. Obtain photographs in frontal and side view to document preoperative appearance. 9. Discontinue aspirin and nonsteroidal anti-inflammatory agents for 10 days before surgery. Discontinue warfarin 2–3 days preoperatively, if medically possible. 10. Query patient about bleeding tendencies. A useful screening question is asking if the patient had unusual bleeding after dental extraction. Obtain hematological evaluation if bleeding tendency is suspected. 1. Mark location of desired lid crease with tissue marking pen usually at the upper border of the tarsal plate. a. In general, use the existing lid crease because it is easier to make symmetric marks. Note: Creases are lower in men than in women, and lower in most Asian individuals than in Caucasians. b. The eyelid crease is ~6 mm above lashes at the lateral canthus, 7–9 mm centrally, and 5 mm nasally. Figure 52.1 a. Place lower tooth of forceps on the premarked lid crease line, pinch excess skin just enough to evert lid margin slightly. Repeat this maneuver over the full extent of the upper lid, marking upper border of skin to be resected with marking pen. (This maneuver suggests the most skin that can be removed without developing lagophthalmos) (Fig. 52.1). Figure 52.2 b. Measure from inferior aspect of eyebrow to upper aspect of planned excision on each side. In functional blepharoplasty, it is rare to leave less than 8–10 mm from inferior brow to upper aspect of the incision. In cosmetic blepharoplasty, leaving 12–17 mm of skin is typical. Note, by inspection and palpation, the junction of thin eyelid skin and thicker skin below eyebrow; do not extend excision into the thicker skin (Fig. 52.2). 3. Extend marks medially to level of superior punctum and temporally beyond lateral canthus. a. Lateral extent of blepharoplasty is determined by redundancy of skin beyond canthus. If skin is to be excised laterally, gently slope excision superiorly from the canthus following the normal skin crease pattern. b. Angle upward if extending medial past punctum to avoid webbing. 4. Apply topical anesthetic. 5. Subcutaneous infiltration with a 50:50 mixture of lido-caine 2% plus 1:100,000 epinephrine and 0.75% bupivacaine.
Blepharoplasty
 Upper Eyelid
Upper Eyelid
Indications
 Removal of redundant skin that is obstructing visual field or causing symptoms of heaviness and fatigue
Removal of redundant skin that is obstructing visual field or causing symptoms of heaviness and fatigue
 Cosmetic improvement
Cosmetic improvement
 Upper blepharoplasty may be used as an adjunct to ptosis surgery in patients with lid droop and excess upper lid skin.
Upper blepharoplasty may be used as an adjunct to ptosis surgery in patients with lid droop and excess upper lid skin.
 Upper blepharoplasty may be used to harvest skin for reconstructive skin graft.
Upper blepharoplasty may be used to harvest skin for reconstructive skin graft.
Preoperative Procedure
Instrumentation
 Scleral shield
Scleral shield
 Marking pen
Marking pen
 Toothed forceps
Toothed forceps
 Scalpel (e.g., #15 Bard-Parker blade)
Scalpel (e.g., #15 Bard-Parker blade)
 Stevens scissors
Stevens scissors
 Westcott scissors
Westcott scissors
 Cautery
Cautery
 Needle holder
Needle holder
 Hemostat
Hemostat
 Sutures 6–0 Prolene or 6–0 fast absorbing plain gut
Sutures 6–0 Prolene or 6–0 fast absorbing plain gut
Operative Procedure
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


