Purpose
To compare binocular visual function of pseudophakic patients having modified monovision (0.75 diopter [D] anisometropia) with that of patients having conventional monovision (1.75 D anisometropia).
Design
Prospective observational study.
Methods
Eighty-two patients that underwent bilateral implantation of a monofocal intraocular lens were recruited at 3 months postoperatively. Modified monovision was simulated by adding a +0.75 D spherical lens to the nondominant eye, while conventional monovision was simulated by adding a +1.75 D spherical lens. Binocular corrected visual acuity (VA) at various distances, binocular contrast VA (contrast VA) and that with glare (glare VA), and stereoacuity were evaluated.
Results
With modified monovision, mean binocular corrected intermediate VA at 1.0 m was 20/19 and near VA at 0.3 m was 20/51, and stereoacuity was 125 ± 100 seconds of arc. Mean binocular intermediate VA at 1.0 m was significantly better with modified monovision than with conventional monovision ( P = .0001), while near VA and intermediate VA at 0.5 m were significantly worse ( P < .0001). Mean binocular photopic and mesopic contrast VA and glare VA tended to be better with modified monovision than with conventional monovision, but the difference was not significant. Mean stereoacuity was significantly better with modified monovision than with conventional monovision ( P = .0020).
Conclusions
Modified pseudophakic monovision provided excellent binocular VA from far to intermediate distances, although near VA was worse than that with conventional monovision. Contrast VA with and without glare tended to be better and stereoacuity was significantly better with modified monovision, suggesting that this method is useful for correcting presbyopia without marked impairment of binocular function.
Pseudophakic monovision is now widely applied for correcting presbyopia when performing cararact surgery with monofocal intraocular lens (IOL) implantation. Previous studies demonstrated significant improvement in bilateral near and intermediate visual acuity (VA) with pseudophakic monovision. Compared with implantation of diffractive multifocal IOLs, uncorrected intermediate VA is better and near VA is worse with pseudophakic monovision. In addition, because glare and halo symptoms are slight with monovision using monofocal IOLs, the incidence of IOL explantation is much lower with pseudophakic monovision than with multifocal IOLs.
Successful monovision primarily depends on the degree of anisometropia between both eyes. In proportion to the degree of anisometropia, uncorrected near VA and intermediate VA are improved, but stereopsis and binocular contrast sensitivity are impaired. Pseudophakic monovision was originally developed to create approximately −2 diopter (D) of myopia in 1 eye. As stereopsis in patients with 2 D of monovision is substantially impaired, however, we assumed that approximately 1.5 D of anisometropia would be the optimal refraction for pseudophakic monovision to achieve useful near vision with less compromised stereopsis. Furthermore, more than 1.5 D of defocus decreases binocular contrast sensitivity to a level worse than monocular contrast sensitivity because of the loss of binocular summation.
Intermediate vision tasks including using a computer or mobile phone have become increasingly important. Some patients who predominantly perform intermediate vision tasks prefer to maintain high-quality stereopsis and binocular contrast sensitivity over achieving excellent near vision, and may therefore choose to use reading glasses when they read small letters over a long period of time. For such patients, modified pseudophakic monovision with −0.5 to −1.0 D of anisometropia may be suitable. Although a certain percentage of surgeons actually prefer this method, the outcomes of modified pseudophakic monovision have not been clarified.
The purpose of the present study was to compare binocular visual function of patients having modified pseudophakic monovision with that of patients having conventional pseudophakic monovision. To strictly assess visual function, modified monovision with −0.75 D of anisometropia and conventional monovision with −1.75 D of anisometropia was simulated in the same patients. Furthermore, to evaluate the changes in binocular visual function in bilaterally emmetropic patients, we used the binocular visual function of patients without monovision as a control.
Methods
Patients
This study was an experimental study. All patients scheduled to undergo bilateral cataract extraction and implantation of a monofocal IOL between November 2012 and December 2013 were sequentially screened for enrollment by a clinical research coordinator. Preoperative exclusion criteria were pathology of the optic nerve, macula, or cornea; severe opaque media other than cataract; previous history of ocular inflammation or surgery; abnormal ocular position (esophoria or exophoria); pupillary diameter smaller than 4.5 mm after full pupil dilation; and any difficulties with examinations. Screening was continued until 82 patients were recruited. This research adhered to the tenets of the Declaration of Helsinki. The Institutional Review Board (IRB)/Ethics Committee of the Hayashi Eye Hospital, Fukuoka, Japan, at which the present study was conducted, approved the study protocol, and all patients provided written informed consent to participate in the present study.
Surgical Techniques
A single surgeon (K.H.) performed all surgeries using the same previously described procedure. First, a continuous curvilinear capsulorrhexis measuring approximately 5.0 mm in diameter was made using a bent needle. Next, a 2.4-mm clear corneal incision was made using a steel keratome, and endocapsular phacoemulsification of the nucleus and aspiration of residual cortex were performed. Finally, the wound was enlarged to 2.65 mm using a steel keratome. The lens capsule was inflated with 1% sodium hyaluronate (Healon; Abbot Medical Optics, Santa Ana, California, USA), after which a hydrophobic acrylic IOL (ZCB00, Abbot Medical Optics) was placed into the capsular bag using the Monarch II injector (Alcon Laboratories, Fort Worth, Texas, USA).
Simulation of Monovision
Simulation of pseudophakic monovision was performed at 3 months postoperatively. Modified monovision was simulated by adjusting the dominant eye to emmetropia and the nondominant eye to −0.75 D of myopia (modified monovision group), while conventional monovision was simulated by adjusting the dominant eye to emmetropia and the nondominant eye to −1.75 D of myopia (conventional monovision group), using the method described previously. In brief, the dominant eye was determined by the hole-in-card test (sighting dominance), in which the patients were asked to look at a Landolt target at 5 m through a 1-cm hole in the center of the cardboard. After full distance correction in both eyes, a spherical lens of +0.75 or +1.75 D was added to the nondominant eye. The same 82 patients in whom bilateral eyes were distance corrected without the addition of a spherical lens served as controls (non-monovision group).
Outcome Measures
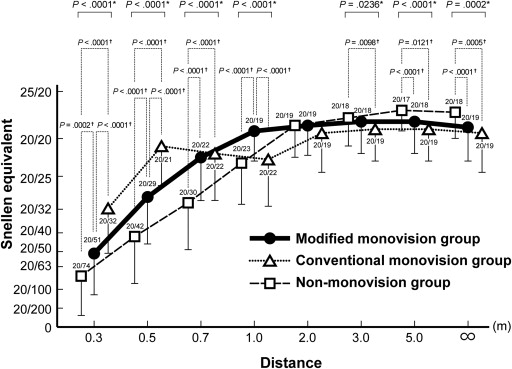
After simulation of 0, 0.75, and 1.75 D of monovision, binocular distance-corrected VA from far to near distances was measured using the all-distance vision tester (AS-15; Kowa, Nagoya, Japan). The method used to measure VA at various distances using the AS-15 are described elsewhere. This device measures equivalent VA at infinity (∞), and at 5.0-, 3.0-, 2.0-, 1.0-, 0.7-, 0.5-, and 0.3-m distances by placing a spherical lens and variously sized visual targets at appropriate distances along the visual axis. We define VA between 0.3 m and 0.4 m as near VA, and that between 0.5 m and 1.0 m as intermediate VA.
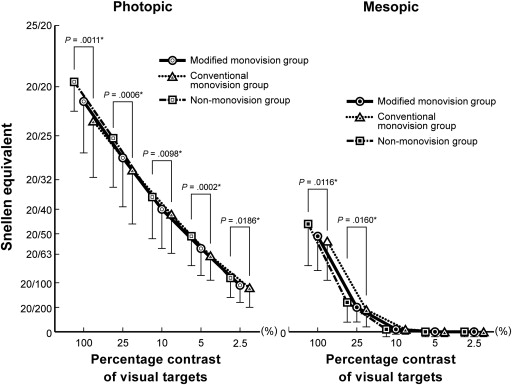
Binocular contrast VA under photopic and mesopic conditions was examined using the Contrast Sensitivity Accurate Tester (CAT-2000; Menicon, Nagoya, Japan). The CAT-2000 measures the logarithm of the minimal angle of resolution (logMAR) VA using 5 contrast percentages of visual targets (100%, 25%, 10%, 5%, and 2.5%) under photopic and mesopic luminance conditions. Measurement under the photopic lighting condition was made with a chart luminance of 100 candela/m 2 , while the chart luminance under the mesopic condition was 2 candela/m 2 .
Near stereoacuity at 0.4 m was examined using the Titmus stereo test under photopic conditions (80–100 cd/m 2 ). Stereoacuity was determined by the number of circles for which a patient answered correctly, and this number was converted to seconds of arc for statistical analysis. The stereoacuity level of circle 5, which is equivalent to 100 seconds of arc (arc sec), is considered to be the lowest limit of useful stereoacuity.
The subjective refractive status (spherical and cylindrical powers) and keratometric cylinder were measured using an autorefractometer (KR-7100; Topcon, Tokyo, Japan). The manifest spherical equivalent was determined as the spherical power plus half the cylindrical power. The pupillary diameter was examined using the Colvard pupillometer (Oasis Medical, Glendora, California, USA). All examinations were performed by ophthalmic technicians unaware of the study objectives.
Data Analysis
Decimal VA was converted to the logMAR scale for statistical analyses. Differences in mean corrected VA at far to near distances, contrast VA and glare VA, stereoacuity, manifest spherical equivalent value, keratometric astigmatism, and other continuous variables between the groups with 0, 0.75, and 1.75 D pseudophakic monovision were compared using the Kruskal-Wallis test. Categorical variables were compared between the 3 groups using the goodness of fit for χ 2 . When a statistically significant difference was found between the 3 groups, the difference between each combination of 2 groups was further compared using the Mann-Whitney U test for continuous variables and the χ 2 or Fisher exact test for categorical variables with the Bonferroni adjustment for multiple comparisons. The correlations between age and binocular corrected VA from far to near distances, and between age and contrast VA and glare VA, were examined using the Spearman rank correlation test. Any difference with a P value of less than .05 was considered statistically significant.
Results
The 82 enrolled patients completed all scheduled examinations. Mean patient age (±standard deviation) was 69.2 ± 9.4 years (range 50–85 years). There were 37 men and 45 women. Characteristics of patients’ dominant and nondominant eyes are shown in Table 1 . Mean manifest spherical equivalent value, keratometric astigmatism, uncorrected or corrected distance VA, or pupillary diameter looking at far and near did not differ significantly between the dominant and nondominant eyes. The right eye was more often the dominant eye than the left eye ( P = .0030).
| Characteristics | Dominant Eye | Nondominant Eye | P Value |
|---|---|---|---|
| Age (y) | 69.2 ± 9.4 | – | |
| Sex (male/female) | 37/45 | – | |
| Left/right a | 31/51 | 51/31 | .0030 b |
| MRSE (D) | −0.36 ± 0.36 | −0.35 ± 0.38 | .5336 |
| Corneal astigmatism (D) c | 0.68 ± 0.40 | 0.73 ± 0.45 | .7437 |
| LogMAR visual acuity | −0.02 ± 0.04 | −0.02 ± 0.04 | .5350 |
| Pupillary diameter (mm) d | |||
| Far (5.0 m) | 3.3 ± 0.6 | 3.2 ± 0.6 | .5525 |
| Near (0.4 m) | 2.7 ± 0.5 | 2.6 ± 0.6 | .5258 |
a The ratio of the left and right eyes.
b Statistically significant difference.
d Measured under photopic lighting condition of 100∼180 cd/mm 2 .
Binocular Visual Acuity at Far to Near Distances
Mean binocular corrected VA at distances of ∞ and 5.0, 3.0, 1.0, 0.7, 0.5, and 0.3 m differed significantly between the modified monovision, conventional monovision, and non-monovision groups ( P ≤ .0236), except for binocular VA at 2.0 m ( Figure 1 ). Mean binocular intermediate VA at 1.0 m was significantly better, and binocular near VA at 0.3 m and intermediate VA at 0.5 m was worse, in the modified monovision group than in the conventional monovision group ( P ≤ .0001). Mean binocular VA at other distances did not differ significantly between the 2 groups. Binocular near VA at 0.3 m and intermediate VA at 0.5, 0.7, and 1.0 m were significantly better, and binocular distance VA at ∞ and 5.0 m was significantly worse, in the modified monovision group than in the non-monovision group ( P ≤ .0121). When we assumed a logMAR binocular VA of 0.1 to be a clinically meaningful magnitude of difference among the 3 groups using the Kruskal-Wallis test, the statistical power was calculated to be more than 98%, except for logMAR binocular VA at 1.0 m. Although the statistical power of binocular VA at 1.0 m was 48%, mean binocular VA at 1.0 m was significantly different among the 3 groups ( P < .0001).
Distribution of Binocular Visual Acuity at 5.0, 1.0, and 0.3 Meters
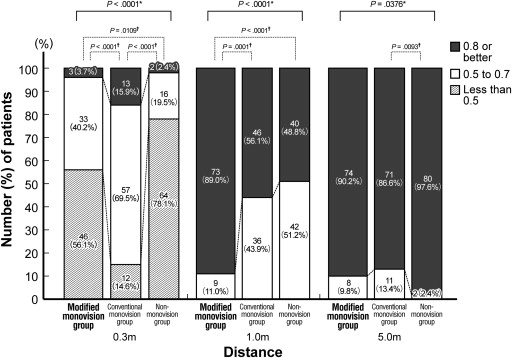
The distribution of binocular corrected VA at 5.0, 1.0, and 0.3 m differed significantly between the 3 groups ( P ≤ .0376; Figure 2 ). The distribution of binocular intermediate VA at 1.0 m was significantly better and that of near VA at 0.3 m was significantly worse in the modified monovision group than in the conventional monovision group ( P < .0001), while there was no significant difference in the distribution of distance VA at 5.0 m. The distribution of binocular intermediate VA at 1.0 m and near VA at 0.3 m was significantly better in the modified monovision group than in the non-monovision group ( P ≤ .0001), whereas there was no significant difference in that of distance VA at 5.0 m.
Contrast Visual Acuity and Glare Visual Acuity
Mean binocular contrast VA ( Figure 3 ) and glare VA ( Figure 4 ) under both photopic and mesopic conditions differed significantly among the 3 groups ( P ≤ .0254), except for mesopic contrast VA at 5% and 2.5% contrast and mesopic glare VA at 10%, 5%, and 2.5% contrast. Mean contrast VA and glare VA under photopic and mesopic conditions tended to be better in the modified monovision group than in the conventional monovision group, but the difference was not significant. The photopic and mesopic contrast VA and glare VA were significantly worse in the modified monovision group than in the non-monovision group at most contrast levels ( P ≤ .0131). When we assumed a logMAR contrast VA and glare VA of 0.1 to be a clinically meaningful difference among the 3 groups using the Kruskal-Wallis test, the statistical powers were more than 97%, except for mesopic glare VA at 25% contrast. Although the statistical power of mesopic glare VA at 25% contrast was 74%, mean mesopic glare VA at 25% contrast was significantly different among the 3 groups ( P = .0160).
Near Stereoacuity
Mean near stereoacuity was 125 ± 100 arc sec in the modified monovision group, 184 ± 146 arc sec in the conventional monovision group, and 91 ± 40 arc sec in the non-monovision group; the mean value was smallest in the non-monovision group, followed by the modified monovision group and conventional monovision group ( P < .0001; Figure 5 ). The number (percentage) of patients who achieved a disparity threshold of 100 arc sec or better was 68 patients (82.9%) in the non-monovision group, 52 patients (63.4%) in the modified monovision group, and 39 patients (47.6%) in the conventional monovision group; the incidence was highest in the non-monovision group, followed by the modified monovision group and the conventional monovision group ( P < .0001).
Correlation Between Age and Binocular Visual Acuity at Far to Near Distances and Between Age and Contrast Visual Acuity and Glare Visual Acuity
Using the Spearman rank correlation analysis, significant correlations were found between age and binocular corrected VA at 5.0, 3.0, 2.0, and 1.0 m in the modified monovision group and the non-monovision group ( Table 2 ). In the conventional monovision group, there was a weak but significant correlation between age and binocular corrected VA only at 0.5 m. At these distances, younger age correlated significantly with better binocular VA.
| Modified Monovision Group | Conventional Monovision Group | Non-monovision Group | ||||
|---|---|---|---|---|---|---|
| Spearman ρ a | P Value | Spearman ρ a | P Value | Spearman ρ a | P Value | |
| Binocular visual acuity at far to near distances | ||||||
| ∞ | 0.204 | .0662 | 0.097 | .3834 | 0.371 | .0008 b |
| 5.0 m | 0.347 | .0018 b | 0.164 | .1399 | 0.500 | <.0001 b |
| 3.0 m | 0.300 | .0055 b | 0.090 | .4192 | 0.435 | <.0001 b |
| 2.0 m | 0.260 | .0193 b | 0.080 | .4733 | 0.347 | .0018 b |
| 1.0 m | 0.310 | .0052 b | 0.181 | .1027 | 0.213 | .0554 |
| 0.7 m | 0.173 | .1193 | 0.197 | .0764 | 0.041 | .7095 |
| 0.5 m | −0.004 | .9736 | 0.270 | .0150 b | 0.046 | .6807 |
| 0.3 m | −0.122 | .2725 | −0.043 | .7002 | −0.168 | .1307 |
| Photopic contrast visual acuity | ||||||
| 100% | 0.484 | <.0001 b | 0.370 | .0009 b | 0.277 | .0128 b |
| 25% | 0.404 | .0003 b | 0.356 | .0013 b | 0.420 | .0002 b |
| 10% | 0.373 | .0008 b | 0.273 | .0140 b | 0.274 | .0137 b |
| 5% | 0.356 | .0013 b | 0.336 | .0025 b | 0.382 | .0006 b |
| 2.5% | 0.346 | .0019 b | 0.310 | .0052 b | 0.407 | .0003 b |
| Mesopic contrast visual acuity c | ||||||
| 100% | 0.111 | .3188 | 0.237 | .0328 b | 0.405 | .0003 b |
| 25% | 0.269 | .0154 | 0.253 | .0228 b | 0.273 | .0140 b |
| 10% | 0.239 | .0317 b | 0.289 | .0094 b | 0.364 | .0011 b |
| Photopic glare visual acuity | ||||||
| 100% | 0.375 | .0007 b | 0.289 | .0092 b | 0.428 | <.0001 b |
| 25% | 0.378 | .0007 b | 0.275 | .0132 b | 0.436 | <.0001 b |
| 10% | 0.311 | .0051 b | 0.280 | .0117 b | 0.436 | <.0001 b |
| 5% | 0.390 | .0004 b | 0.241 | .0304 b | 0.398 | .0003 b |
| 2.5% | 0.346 | .0019 b | 0.307 | .0057 b | 0.376 | .0007 b |
| Mesopic glare visual acuity c | ||||||
| 100% | 0.308 | .0055 b | 0.312 | .0050 b | 0.442 | <.0001 b |
| 25% | 0.369 | .0009 b | 0.304 | .0062 b | 0.380 | .0006 b |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


