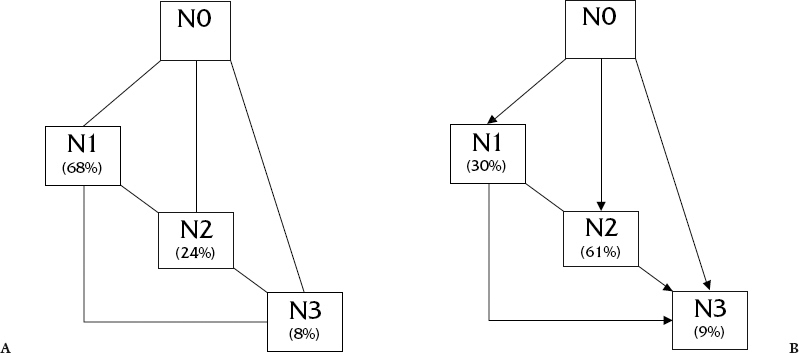
The presence of regional lymph node metastasis at initial presentation is the single most important factor influencing the outcome of patients with upper aerodigestive tract squamous cell carcinomas.1–4 Accordingly, an aggressive approach to the management of patients presenting with obvious lymphatic metastasis is advocated. However, the management of clinically occult dissemination of squamous cell carcinoma to regional lymph nodes is a topic of considerable debate.5–11 The controversy focuses mainly on four issues: the need for elective treatment, selection of patients requiring intervention, the type of intervention to be used, and the benefit of such intervention to the patient. Need for Elective Treatment Several studies have shown a diminished survival rate in patients with occult lymphatic metastasis. Tulenko et al.12 showed that the 5-year cure rate decrease from 79% in patients without any evidence of metastasis to 29% in those with occult disease detected on pathologic examination to 11% in those with clinically evident disease. Similarly, Alvi and Johnson13 showed that disease control rates decreased from 82% for patients without metastasis to 47% for those with occult metastasis and to 31% when extracapsular spread was present in lymph nodes containing occult metastasis. Accordingly, identification and treatment of patients with occult metastasis appear warranted. However, because there is no statistical difference in regional control rates or survival between patients undergoing elective neck dissection for micrometastasis compared with those undergoing therapeutic neck dissection for N1 disease, extrapolation suggests that patients with N0 necks can be followed until metastasis becomes clinically evident.3 Unfortunately, patients at risk of micrometastasis to the cervical lymphatics do not absolutely progress in an orderly fashion.3, 9, 14–17 A report by Anderson et al.14 showed that most patients initially observed with N0 neck, have greater than N1 nodal involvement clinically at subsequent treatment, even under close follow-up (Fig. 3–1). In fact, most patients (77%) had metastatic disease greater than N1 or associated extracapsular spread on pathologic analysis. In addition, in patients with N0 necks, the rate of distant metastasis is higher in those who develop subsequent nodal recurrence (11%) as compared with patients who remain disease free (3%).7, 8 This suggests early intervention is warranted in patients at high risk of occult nodal involvement. Figure 3-1 Clinical findings in patients failing in the neck after observation for N0 neck. (B) Pathological findings in patients failing in the neck after observation for N0 neck. Theoretically, the early identification and treatment of patients with metastatic squamous cell carcinoma to regional cervical lymph nodes will have a favorable impact on survival, but prospective studies have failed to confirm this association. However, improved disease-free survival has been observed in both prospective and retrospective analysis. Kligerman et al.17 found that the disease-free survival increased from 49% to 72% with the addition of elective supraomohyoid neck dissection. Similarly, Fakih et al.16 also reported increased disease-free survival with the addition of elective neck treatment (67% vs 47%). In summary, elective neck dissection helps in prognostication, identifies cases requiring adjuvant treatment, and improves initial disease control rates. Selection of Patients Requiring Elective Treatment No parameters have been established to identify patients reliably with clinically occult lymphatic metastasis. Most investigators have adopted an arbitrary cutoff of 10 to 15% incidence of occult nodal involvement to select patients requiring elective intervention. Decision analysis, based on the data from the available medical literature, suggests that a 20% risk should be the accepted threshold for providing treatment.18 The risk of occult regional lymphatic metastasis from primary squamous cell carcinomas of the upper aerodigestive tract can be assessed on the basis of anatomic location of the primary tumor, size, T stage, and histomorphologic characteristics (Table 3-1). In general, the risk of occult nodal metastasis increases from the anterior to posterior aspect of the upper aerodigestive tract (i.e. the lips, <5%; oral cavity, 19 to 50%; oropharynx, 22 to 66%; and hypopharynx, 38 to 77%.1–3, 19–22 For tumors of the larynx and pharynx, the risk of nodal metastasis increases as one progresses from the center of the laryngopharyngeal compartment to the periphery.2, 3, 22, 23 The risk of occult regional lymph node metastasis from carcinoma of the true vocal cord is exceedingly small, increasing as one progresses from the vocal cords to the false vocal cords, aryepiglottic fold (16 to 26%), pyriform sinus (38%), and pharyngeal wall (66%).2, 3, 22, 23 Within the oral cavity, a significantly higher risk of occult nodal metastases occurs in floor-of-mouth (40 to 50%), gingival (19%), and oral tongue cancers (25 to 54%) than those originating from the hard palate (< 5%).2, 3, 22, 23 The risk of occult nodal metastases increases with increasing primary tumor burden at any site, as reflected by the T stage. The risk of nodal metastasis increases from <14% for T1 lesions to 30% for T2, 45% for T3, and 55 to 75% for T4 lesions. Occult involvement increases from 19% for T1 and T2 lesions to 26 to 32% of T3 and T4.1–3, 5, 24
| Anatomic location |
| Size |
| T stage |
| Depth of invasion |
| Type of host-tumor interface |
| Endophytic growth pattern |
Certain histomorphologic features of the primary tumor also predict an increased risk of nodal metastasis. Endophytic tumors are more inclined to metastasize than are exophytic tumors. It has been well documented that for tongue and floor-of-mouth cancers, tumor thickness is related to the risk of nodal metastases, with a 7.5% prevalence of occult metastasis for tumors < 2 mm thick compared with 26% for 2–8 mm tumors and 42% for those > 8mm in thickness25 (Table 3-2). Similarly, Fukano and his colleagues showed clinically negative necks turned out pathologically positive in 30% of cases with <5 mm depth of invasion, compared with 43% when the tumor depth was <5 mm.26 Poorly differentiated carcinomas are associated with a higher risk of nodal metastasis compared with well-differentiated lesions. In addition, such factors as tumor-host interface have been suggested to be predictive of risk.27
Augmentation of clinical examination with various radiologic studies, including computed tomography (CT) (66%), magnetic resonance imaging (MRI) (75%), and ultrasound examination (68%), enhances the accuracy with which those patients who have nodal metastasis can be identified.28–39 Although a 92% accuracy rate for identifying cervical metastasis is reported with the use of positron emission tomography (PET) scanning, it is tainted by sample size constraints.38 The use of sentinel node biopsy and molecular assessment for occult metastasis also remains both limited and variable in efficacy.40–43 The presence of metastasis that is missed on routine pathologic examination is confirmed in studies using supplemental subserial sectioning, immunohistochemistry, or molecular analysis.
An additional 8% of cases with metastasis in regional lymph nodes were identified by Ambroch and Brink44 on serial sectioning of lymph nodes reported as negative on routine pathologic examination in N0 necks. Most strikingly, Brennan et al.42 identified a 21% rate on missed lymphatic metastasis, using p53 mutation analysis. Finally, mathematical models, attempting to combine all available information, and molecular studies, attempting to identify patients at increased risk of occult metastasis, have also met with variable results.19, 45 Overall, even with the use of supplemental studies, no reliable methods have been identified for accurate prediction of the presence of nodal metastasis in individual patients with clinically undetectable disease. Accordingly, selection of patients for elective treatment continues to be made on the basis of arbitrary criteria.
| With Lymph Node Metastasis (%) | Dead of Disease(%) | |
| <2 mm | 13 | 3 |
| 2-9 mm | 46 | 17 |
| >9 mm | 65 |



