Types
Subtypes
Non-melanocytic
Benign
Squamous cell papilloma
Seborrheic keratosis
Inverted follicular keratosis
Molluscum contagiosum
Reactive hyperplasia (pseudoepitheliomatous hyperplasia)
Potentially premalignant
Actinic (solar) keratosis
Intraepithelial neoplasia
Sebaceous nevus (of Jadassohn)
Malignant
Basal cell carcinoma
Squamous cell carcinoma
Melanocytic
Benign epithelial pigmentation or hypermelanosis
Ephelis or freckles
Lentigo simplex
Solar lentigo
Benign
Junctional nevus
Intradermal nevus
Compound nevus
Spitz nevus
Balloon cell nevus
Blue nevus and cellular blue nevus
Oculodermal nevus of Ota
Seborrheic keratosis
Potentially premalignant
Congenital dysplastic nevus
Lentigo maligna (melanotic freckle of Hutchinson)
Malignant
Melanoma arising from nevi
Melanoma arising in lentigo maligna
Melanoma arising de novo
3.2 Squamous (Non-melanocytic)
3.2.1 Benign Epidermal Tumors
3.2.1.1 Squamous Cell Papilloma
Squamous papillomas are common benign tumors typically occurring in middle-aged or older adults.
Clinical Features
The clinical appearance is that of a pedunculated or sessile nodular growth with a variably convoluted surface.
Histopathologic Features
Microscopically a papilloma consists of benign squamous epithelium with variable acanthosis and hyperkeratosis overlying an expanded fibrovascular core, which creates the exophytic nodule (Fig. 3.1).
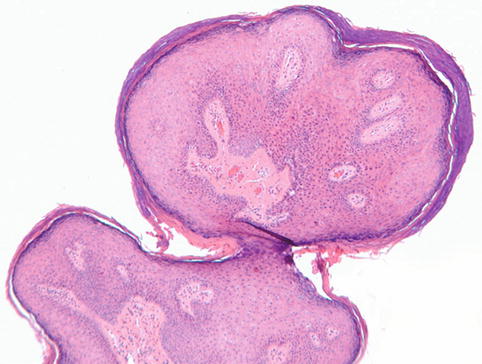
Fig. 3.1
Squamous papilloma. Polypoid lesion consisting of benign squamous epithelium with variable acanthosis and hyperkeratosis overlying a fibrovascular core (hematoxylin and eosin; original magnification 4×)
Treatment
If symptomatic, surgical excision may be performed.
3.2.1.2 Seborrheic Keratosis
Seborrheic keratoses are commonly acquired skin lesions which can occur on the eyelid affecting middle-aged and elderly patients.
Clinical Features
The clinical appearance varies considerably in terms of size (few millimeters to several centimeters) and degree of pigmentation making it sometimes difficult to differentiate clinically from nevi, pigmented basal cell carcinomas, and melanoma [1]. They are sharply demarcated warty plaques or dome-shaped growths with a greasy surface, which may become friable with inflamed eczema-like features (Fig. 3.2).
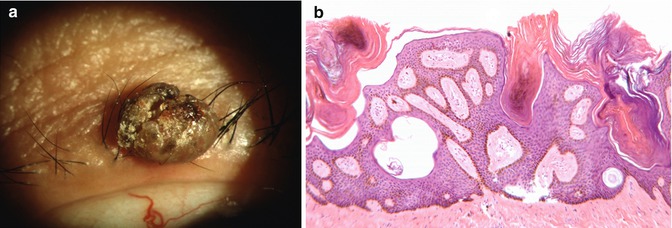
Fig. 3.2
Seborrheic keratosis. Upper eyelid involvement in a 75-year-old man (a). Retiform (network-like) pattern of squamous epithelium surrounding islands of connective tissue and composed of sheets of basaloid cells with keratin-filled horn pseudocysts (b; hematoxylin and eosin; original magnification 10×)
Histopathologic Features
Seborrheic keratoses are divided into several histological types according to the predominant histologic features: acanthotic, hyperkeratotic, adenoid, clonal, and irritated (Fig. 3.2). The most common type is the acanthotic, in which there is a proliferation of squamous basaloid cells protruding above the skin surface, which is punctuated by horn pseudocysts. Hyperpigmentation can occur, which is due to transfer of melanin to the keratinocytes. When a patient experiences a sudden appearance of a seborrheic keratosis or an increase in the number or size of these lesions, this may be associated with an internal malignancy and is referred to as the Leser-Trelat sign [2].
Treatment
Even in lesions that are large, the growth pattern is superficial with growth predominantly above the epidermal surface. Therefore, deep excision is unnecessary, and these lesions are often removed by shave biopsy.
3.2.1.3 Inverted Follicular Keratosis
Also known as irritated seborrheic keratosis, inverted follicular keratosis is commonly seen on the face. The eyelid margin is a frequent site of involvement [3].
Clinical Features
Usually a solitary lesion of recent onset (less than 3 months), it may be nodular, papillomatous, or cystic in appearance. Inverted follicular keratosis can be easily mistaken for squamous cell carcinoma.
Histopathologic Features
Histopathologically it consists of an endophytic proliferation of squamous epithelium with squamous eddies, variable pigmentation, and acantholysis and chronic inflammation. There may be increased mitoses and apoptosis (Fig. 3.3) [4].
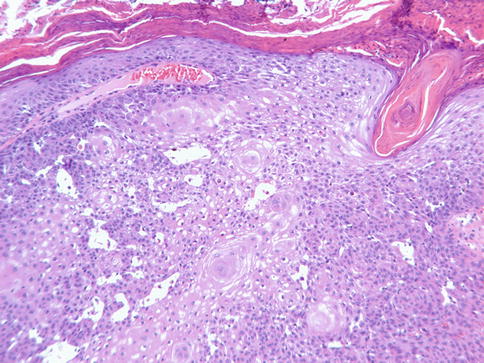
Fig. 3.3
Inverted follicular keratosis. Note endophytic growth pattern with overlying hyperkeratosis and parakeratosis. Flattened concentric epidermal cells within acanthotic areas are called squamous eddies (hematoxylin and eosin; original magnification 10×)
Treatment
Complete excision should be performed.
3.2.1.4 Molluscum contagiosum
Molluscum contagiosum is a nonneoplastic skin infection caused by a virus from the poxvirus group.
Clinical Features
This entity occurs frequently in children but may also occur in adults anywhere on the body except the palms and soles. It appears as papules that are white or flesh colored measuring 2–5 mm, often with a central dimple or plug containing cheesy or waxy material (Fig. 3.4).
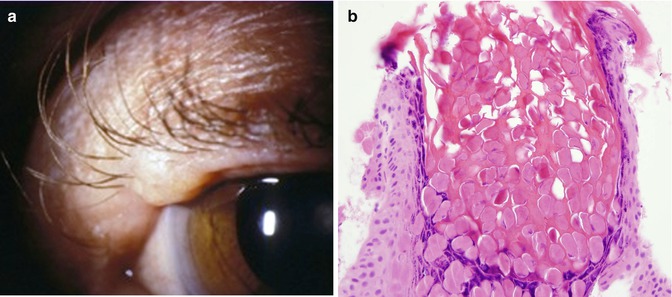
Fig. 3.4
Molluscum contagiosum. Clinical appearance (a). Epidermal crater filled with keratinocytes containing molluscum bodies (intracytoplasmic inclusions) (b. hematoxylin and eosin; original 40× magnification)
Histopathologic Features
Molluscum contagiosum is characterized by downward growth of the epidermis forming multiple lobules. The keratinocytes contain large eosinophilic intracytoplasmic inclusion bodies (“molluscum bodies”) which are characteristic (Fig. 3.4). The central crater consists of disintegrating cells discharging the molluscum bodies and keratin.
Treatment
These lesions usually resolve over months to years in patients with intact immune systems. However, removal of individual lesions can be done surgically or by scraping, de-coring, freezing, or electrosurgery. Medications used for warts may also be used, and cantharidin (“beetle juice”) is the most common solution used. Tretinoin cream is an alternative.
3.2.1.5 Keratoacanthoma
3.2.1.6 Reactive Hyperplasia (Pseudoepitheliomatous Hyperplasia)
Epithelial hyperplasia occurs as a reaction to trauma, surgical wound, cryotherapy, burn, radiation, ulcers, or fungal infection. It can also occur in association with tumors such as granular cell tumor and melanocytic lesions. It is not a tumor but rather a reactive process that may clinically be seen as a tumor and is histopathologically challenging as well.
Clinical Features
An elevated nodular or ulcerative lesion resembling basal or squamous cell carcinoma.
Histopathologic Features
There is epidermal hyperplasia with elongated seemingly invasive tongues of epithelial cells which may anastomose and are frequently infiltrated by inflammatory cells (Fig. 3.5) [2]. The epithelium shows normal maturation without true dysplasia; however it is not always easy to separate this reactive process from squamous cell carcinoma because of the significant cytologic atypia that may occur.
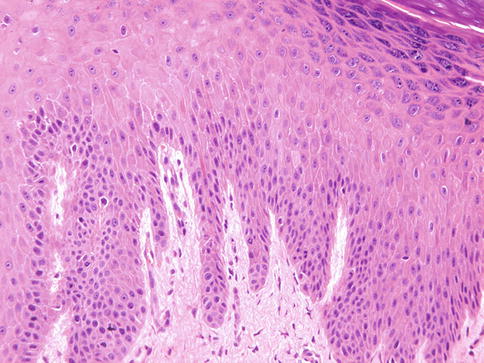
Fig. 3.5
Reactive hyperplasia (pseudoepitheliomatous hyperplasia). Epidermal hyperplasia with elongated and sometimes anastomosing rete ridges, normal maturation of epithelium, and variable hyperkeratosis. Note the absence of atypia in this case (hematoxylin and eosin; original magnification 20×)
Treatment
Complete excision is recommended when clinically suspicious.
3.2.1.7 Cutaneous Horn or Nonspecific Keratosis
These are nondiagnostic descriptive terms for any hyperkeratotic lesion (benign or malignant) and thus do not imply by themselves predilection for malignant behavior.
Clinical Features
A protruding keratotic lesion is the presentation (Fig. 3.6). This lesion is associated with a variety of benign or malignant lesions. In a study of 48 cases involving the eyelids, the most common associated lesions were seborrheic keratosis, actinic keratosis, and basal cell carcinoma and squamous cell carcinoma [8].
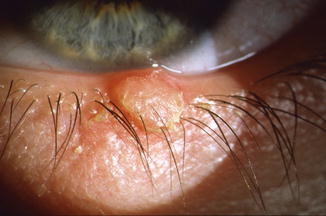
Fig. 3.6
Cutaneous horn is a clinically descriptive, nondiagnostic term for a nonspecific keratosis
Histopathologic Features
There are no specific histopathologic features other than hyperkeratosis. The findings are solely dependent on the particular type of lesion present.
Treatment
Treatment should be determined by the histopathology if possible. If the lesion is clinically suspicious for malignancy, excision is recommended.
3.2.1.8 Sebaceous Nevus (of Jadassohn)
Sebaceous nevus syndrome (of Jadassohn) is an uncommon congenital lesion which is part of the epidermal nevus syndrome, which is characterized by cutaneous sebaceous nevi and extracutaneous manifestations [9]. It is a benign hamartoma composed of large sebaceous glands, heterotopic apocrine glands, defective hair follicles, acanthosis, and papillomatosis. These lesions evolve with time. They are most commonly found on the head and neck region and appear as irregular linear lesions with alopecia. In spite of their being benign, there is an increased risk in adulthood for the development of secondary benign (such as syringocystadenoma papilliferum) or malignant skin tumors (most commonly basal cell carcinoma) within the area of these nevi [10].
3.2.2 Premalignant Squamous Tumors
3.2.2.1 Actinic (Solar) Keratosis
Actinic or solar keratosis is most frequently a result of damage of the epidermal cells of the skin by near ultraviolet radiation. Fair-skinned older patients and those with a history of excessive sun exposure are typically affected. However there is also an increased incidence in renal transplant patients and thus immunosuppression is a risk factor.
Clinical Features
There are a variety of clinical presentations, usually characterized by multiple, erythematous, excoriated, sessile plaques [11]. Although it is a precursor to squamous cell carcinoma, the mitotic activity is generally low [12]. In a study wherein histopathologic evaluation of the resected squamous cell carcinoma was undertaken, 82 % of cases had concomitant actinic keratosis close to the carcinoma [13]. However, population-based studies indicate a much lower annual rate of 0.01 % of malignant transformation of actinic keratosis [14]. Such discrepancy may exist because of differences in clinical and pathological nomenclature used to describe actinic keratosis and early squamous cell carcinoma. It is now believed that actinic keratosis is an incipient form of squamous cell carcinoma requiring treatment [15, 16]. Squamous cell carcinoma that arises from actinic keratosis is low grade and offers an excellent prognosis.
Histopathologic Features
Histopathology generally shows hyperkeratosis and parakeratosis with varying degrees of squamous dysplasia, characterized by loss of epithelial cell polarity and dysmaturation. It involves the interfollicular epidermis, sparing the follicles and the intraepidermal portion of the sweat ducts, an important distinction from carcinoma in situ. Solar elastosis of varying degrees is present in the dermis (Fig. 3.7). Subtypes include hypertrophic (when the epithelium is acanthotic), atrophic (when the epithelium is atrophic or thin), acantholytic (when there is prominent dyscohesion of the basal cells), and lichenoid (when there is a dense mononuclear cell infiltrate in the upper dermis). When there is severe dysplasia, the differential is squamous carcinoma in situ or Bowen’s disease (Fig. 3.8).
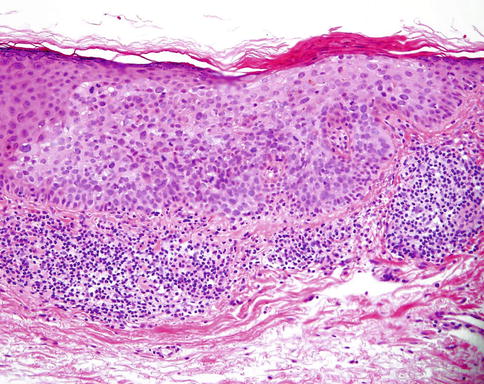
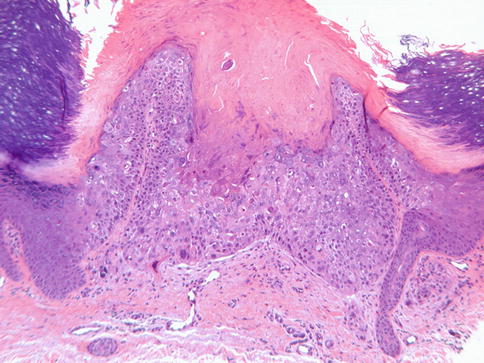
Fig. 3.7
Actinic (solar) keratosis. Note dysmaturation of the squamous epithelium, mitoses, loss of granular layer, and parakeratotic crust (hematoxylin and eosin; original magnification 20×)
Fig. 3.8
Squamous intraepithelial neoplasia. Marked squamous dysplasia (Bowen’s disease, also considered as squamous carcinoma in situ) (hematoxylin and eosin; original magnification 10×)
Treatment
Management is close observation and excision of more suspicious lesions. Multiple lesions can be treated with topical chemotherapeutic agents or cryotherapy [17]. A meta-analysis of published studies indicates that 3 % diclofenac in 2.5 % hyaluronan gel is effective in treatment of actinic kertatosis [18]. Topical gel must not be applied to the eyelids as it is not approved for ophthalmic use.
3.3 Melanocytic Benign Epidermal Tumors
3.3.1 Epithelial Pigmentation
3.3.1.1 Freckles or Ephelides
Freckles are flat brown skin spots that appear in childhood. Freckles characteristically darken with sunlight exposure and fade in winters in the absence of sunlight exposure. In contrast, solar lentigines do not fade with cessation of sunlight exposure.
3.3.1.2 Lentigo Simplex
The lesion of lentigo simplex is flat, brown to black macule measuring 1–2 mm in diameter. They are the precursors of junctional nevi and are clinically indistinguishable from them. Similar appearing multiple lesions of the eyelid may be associated with the autosomal dominant Peutz-Jeghers syndrome of mucocutaneous pigmentation and intestinal polyposis (Chap. 12), Carney syndrome, LEOPARD syndrome, and xeroderma pigmentosum [2]. Histology shows hyperpigmentation of the basal layer with increased number of melanocytes, often with slight elongation of the rete ridges.
3.3.1.3 Solar Lentigo
The lesions of solar lentigo are light to dark brown, slowly expanding macules that develop in chronically sun-exposed areas of the skin, including the eyelids. They occur in over 90 % of elderly Caucasians. Presenting as small macules 3–5 mm in diameter, the lesions may gradually grow to several centimeters in diameter. Differentiation from lentigo maligna and lentigo malignant melanoma is imperative and requires histopathologic examination. Solar lentigo lesions respond to treatment with topical 0.1 % tretinoin, 2 % hydroxyanisole, laser therapy, and cryotherapy.
3.3.2 Melanocytic Nevus
A melanocytic nevus is considered as a hamartoma or a benign tumor of neural crest-derived melanocytes [19]. An eyelid nevus, as in other areas of the skin, can be acquired (usually) or congenital.
3.3.2.1 Congenital Nevus
Clinical Features
Congenital nevi may be single or multiple with sharp borders and are usually larger than acquired nevi. They tend to become darker and the surface undergoes papular or nodular change with age.
Size-Based Classification
The congenital nevi are classified by their largest diameter as small (<1.5 cm), medium (1.5–19.9 cm), and large or giant congenital melanocytic nevi (>20 cm) [21].
Malignant Transformation
The risk of malignant transformation varies significantly with the size of the lesion. The lifetime risk of about 6 % is highest with giant nevus [22]. In another study in which the authors did an analysis of several published studies with a total of 6,571 patients, the overall risk of melanoma was much less (0.7 %) [23]. In this same article, they found that by comparing the age-adjusted data from the SEER database, the relative risk of patients with congenital melanocytic nevi for developing melanoma during childhood and adolescence was 465-fold. Despite irrefutable evidence supporting origin of melanoma in small congenital nevi, the magnitude of risk associated with small- and medium-sized congenital nevi is probably much less although reliable data does not exist [20, 24]. The risk is particularly negligible in prepubertal years [20].
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


