21 Core Messages • Benign neoplasms make up the majority of salivary gland pathology. • The most common benign tumors of the salivary gland are pleomorphic adenomas and Warthin tumors. • History and physical examination are often sufficient to determine if a lesion is benign or malignant but fine-needle aspiration is recommended. • Complete surgical excisioin, not enucleation, is the preferred treatment for benign salivary neoplasms. Benign salivary gland tumors make up the majority of salivary neoplasms. The most common of these are pleomorphic adenomas and Warthin tumors. In the pediatric population, the most common benign salivary tumor is a hemangioma. In addition to those mentioned, there exist several other types that will be covered here. This chapter will discuss the anatomy of salivary glands, the classification of the benign salivary neoplasms, and their management. The major salivary glands are primarily composed of acini and their ducts. The acinar-ductal subunit comprises five kinds of cells: myoepithelial, acinar, intercalated ductal, striated ductal, and excretory ductal (remembered by the acronym MAISE). The acinar cells can be serous, mucinous, or mixed (seromucinous). These cells are surrounded by myoepithelial cells that are contractile in nature. Myoepithelial cells are also located around intercalated ducts. The acinus drains into the intercalated duct and then into the striated duct, which modifies the content of the primary secretion. Finally, the saliva moves to the excretory duct and then to the upper aerodigestive tract. The largest of the paired major salivary glands is the parotid, located preauricularly. It is predominantly serous. The facial nerve exits the stylomastoid foramen and enters the gland, branching at the pes anserinus and then to the five major branches. The nerve arbitrarily divides the parotid into a superficial and deep lobe. Tumors involving the deep lobe may extend into the parapharyngeal space and will be covered in detail later in the chapter. The final excretory duct of the parotid is known as Stenson duct and empties into the buccal mucosa close to the maxillary second molars. Accessory parotid tissue, which is subject to the same pathology as primary parotid tissue, can be located anterior to the parotid near Stenson duct. The second largest of the three paired major salivary glands is the submandibular gland and is located in the submandibular triangle. It is considered mixed, but serous acini compose the majority of the gland. Superficial to the gland lies the facial vein, while the facial artery courses through the gland. Three nerves lie in close proximity to the gland: the marginal mandibular branch of the facial nerve, the lingual nerve, and the hypoglossal nerve. The main excretory duct of the gland is known as Wharton duct and drains into the floor of the mouth at the lingual frenulum. The smallest of the major salivary glands are the paired sublingual glands, located anteriorly in the floor of the mouth. Mucinous acini predominate in these glands. The drainage goes directly in the floor of mouth via the ducts of Rivinus or may join the submandibular (Wharton) duct as the duct of Bartholin. As of writing this chapter, the most recent classification of salivary gland tumors comes from the World Health Organization in 2005. The benign neoplasms included are listed in Table 21.1. Pleomorphic adenomas make up the majority of benign tumors in major and minor salivary glands, with most found in the parotid. They also account for 45 to 70% of all salivary tumors and up to 85% of benign tumors.1,2 Grossly, pleomorphic adenomas can have a rubbery texture and a grayish yellow or tan appearance. Histologically, three types have been described: cellular, myxoid, and classic depending on the balance of epithelial/myoepithelial cells and the stromal component.3 The epithelial cells are ductal while the myoepithelial cells can vary from spindle shaped to oval. Often there is a chondroid stroma or cartilaginous differentiation (Fig. 21.1). True to its name, pleomorphic adenomas have a wide variety of histopathologic appearances and can occasionally confuse the diagnosis with squamous cell carcinoma or mucoepidermoid carcinoma, depending on the epithelial differentiation. Up to 40% show “pseudopod” extensions into the normal parotid tissue and are likely responsible for recurrence after incomplete extirpation.4 Malignant transformation is possible for these tumors and increases over time, with up to 10% becoming malignant over the lifetime of the patient. Table 21.1 World Health Organization Histological Classification of Benign Salivary Tumors
Benign Salivary Gland Tumors
Anatomy
Classification of Benign Salivary Tumors
Pleomorphic Adenoma
Pleomorphic adenoma |
Warthin tumor (papillary cystadenoma lymphomatosum) |
Basal cell adenoma |
Myoepithelioma |
Oncocytoma |
Canalicular adenoma |
Sebaceous adenoma |
Lymphadenoma |
Ductal papillomas |
Cystadenoma Hemangioma |
Treatment involves complete tumor excision with a margin rather than enucleation. In the parotid gland, this usually entails a superficial parotidectomy with facial nerve preservation and complete gland removal for other major or minor salivary glands.
Warthin Tumor
Also known as papillary cystadenoma lymphomatosum, this tumor is the second most common benign salivary tumor. The vast majority occur in the parotid with only rare extraparotid occurrences. The “classic” patient is a 50-to 60-year-old, tobacco-smoking man. Although there is a male predominance, the percentage of men and women involved has become closer over the years. There is a strong predilection for tobacco smokers, and it typically affects patients in their 50s to 80s.1,5 Up to 12.3% can present bilaterally.6 Grossly, they are well circumscribed and cystic, often filled with a brownish or mucus-like fluid. Pathologic examination shows cystic structures with papillary projections lined with two layers of oncocytic cells, in a lymphoid stroma (Fig. 21.2). The latter feature can make it appear like a lymphoma on fine-needle aspiration (FNA) biopsy.
Malignant transformation is rare for these tumors, but the recommended treatment is complete surgical excision. Commonly, Warthin tumors involve the parotid tail so that superficial parotidectomy is sufficient for cure.
Basal Cell Adenoma
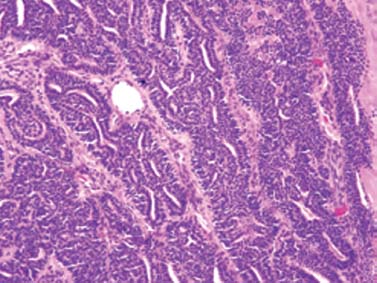
Basal cell adenomas were previously referred to as monomorphic adenomas, though this older classification probably also included canalicular adenomas as well. These rare tumors are three times more likely to be present in the parotid with the rest in minor salivary glands. They make up 1 to 3% of benign salivary gland neoplasms and the mean age at presentation is in the 50s. Pathologically, tumors are basaloid in appearance and can be solid, trabecular, membranous, or tubular (Fig. 21.3).7,8 Treatment involves complete excision.
Oncocytomas
Oncocytes are cells that contain a deeply eosinophilic cytoplasm (because of an abundance of mitochondria) with round nuclei and a low nuclear to cytoplasmic ratio (Fig. 21.4). The most common oncocytic lesion in the head and neck is a Warthin tumor, but the term “oncocytoma” is reserved for a tumor consisting of “oncocytes arranged in solid sheets, collapsed trabeculae, or an organoid pattern.”9 The majority are found in the parotid gland, with the rest located in the oral cavity or sinonasal cavity.10 Sinonasal oncocytomas may be locally aggressive without being malignant.
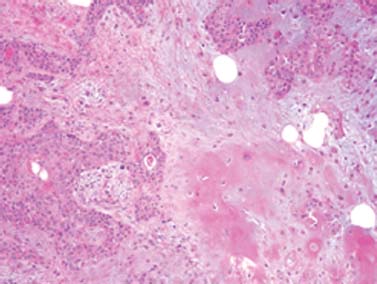
Figure 21.1 Pleomorphic adenoma (hematoxylin and eosin). Note the chondroid differentiation in the center right.
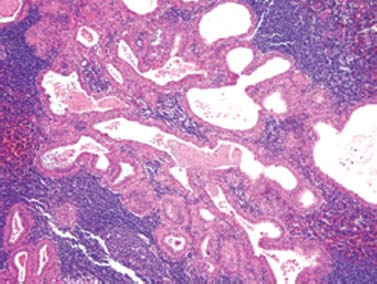
Figure 21.2 Warthin tumor (hematoxylin and eosin). Cystic spaces are lined with oncocytic epithelium with two layers of nuclei.
Canalicular Adenoma
Before 20 years ago, canalicular adenomas were classified together with basal cell adenomas as the monomorphic adenomas. Further histologic analysis has shown these two to be distinct tumors. These tumors almost exclusively occur in the minor salivary glands, usually arising in the upper lip. Rare cases of occurrences in the buccal mucosa, palatal mucosa, and parotid have been described. Very rarely, multiple occurrences can be found in the same patient. The mean age at presentation is between the 60s and 70s.7,11,12 Pathology shows a well-encapsulated mass, with cuboidal to columnar cells arranged in a duct-like pattern, in a loose but vascular stroma (Fig. 21.5). Separation between some of the cells gives a “beads-on-a-string” characteristic.13 Canalicular adenomas can be differentiated from basal call adenomas and pleomorphic adenomas in that they do not contain myoepithelial elements or chondroid differentiation, respectively. Treatment involves complete surgical excision.
Sebaceous Adenoma
Sebaceous adenomas are extremely rare, benign neoplasms that have been reported in the parotid gland, submandibular glands, and intraorally. Because sebaceous glands occur naturally in the oral cavity in a minority of the population, the origin of intraoral sebaceous adenomas is unclear. The mean age at presentation has been reported to be in the 60s. Histologically, they show sebaceous cell nests in an acinar-like pattern, sometimes with squamous differentiation or oncocytic metaplasia.14,15 Surgical excision is curative.
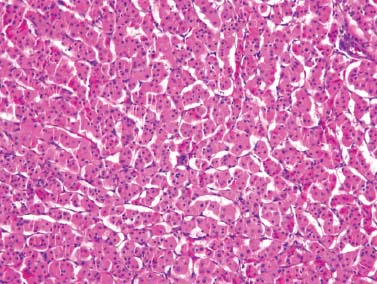
Figure 21.4 Oncocytoma (hematoxylin and eosin). Sheet of oncocytic cells with abundant eosinophilic cytoplasm.



