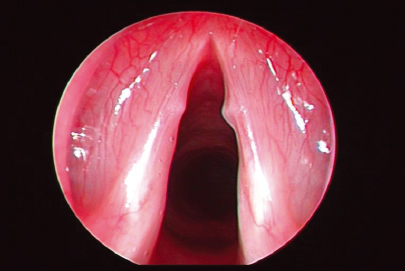
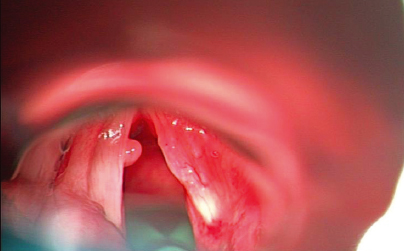
25 Benign Lesions of the Larynx Most patients with benign laryngeal disorders present with dysphonia. All patients should undergo a complete assessment, including a head and neck examination to exclude an underlying malignant neoplastic process. Following this, patients should ideally be managed within a voice clinic, with a suitably qualified voice therapist. A thorough history of all patients presenting with a voice problem is essential. The quality, timing, and frequency of exacerbating and relieving factors must be explored. Contributing factors including smoking, caffeine intake, gastroesophageal reflux disease (GERD), thyroid disease, and regular medications must be documented. Vocal history with particular attention to patterns of vocal behavior should be recorded, as well as attention to vocal hygiene. Vocal abuse behaviors result in damage to the laryngeal mucosa, and this is associated with excessive talking, prolonged or excessive loudness, use of inappropriate pitch, excessive cough, and frequent throat clearing. A detailed examination of the patient’s vocal folds with videolaryngoscopy and stroboscopy should be conducted as routine. In select cases, laryngeal electromyography and quantitative voice measurements may be indicated. Videodocumentation of preoperative findings and a high-quality voice recording are essential. Visualization of the larynx by the patient also enables them to appreciate and understand their pathology and can subsequently improve compliance with voice therapy. Almost all patients with benign laryngeal pathology should be considered for a trial of voice therapy, before surgery is considered. Education regarding vocal hygiene, hydration, and avoidance of vocal abuse is a necessary baseline. Patients must understand how certain behaviors may have contributed to their vocal fold pathology. Voice therapy to address how these factors may have contributed and correction of these may be all that is required for many patients. If this is not sufficient to resolve symptoms, and surgery is indicated, patients should also be considered for postoperative voice therapy, to address contributing factors and prevent recurrence of their pathology. We now have a more comprehensive understanding of the laryngeal anatomy, specifically the microarchitecture of the vocal folds. This knowledge of anatomy has evolved over the past several decades, since Hirano’s description of the complex layered microanatomy of the human vocal fold,1 which is of paramount importance in phonation. The true vocal fold is composed of five separately identifiable layers. The deepest layer consists of the thyroarytenoid muscle, also functionally known as the “body.” Contraction of this muscle stiffens and thickens the vibratory margin of the cord. Overlying this muscle is the lamina propria, which is subdivided into three layers (superficial, middle, and deep), based on the molecular composition of each. The deep layer is largely composed of dense collagen fibers. The middle layer also contains some collagen fibers but is distinguishable by its high elastin content. Together, the deep and middle layers form the vocal ligament or “transition,” a recognized and important landmark in vocal fold surgery, and also a transition between the deepest muscle layer and the “cover” (epithelium and superficial lamina propria). The superficial lamina propria is composed mainly of amorphous glands and a few fibrils. The most superficial of all the layers is the overlying stratified nonkeratinizing squamous epithelium that overlies the superficial lamina propria, and together these form the “cover.” The layered structure of the vocal fold allows the superficial layer to oscillate independently during phonation. Understanding the layered microarchitecture of the true vocal fold and its role in normal voice production has led to much emphasis on refined surgical techniques for maximal preservation of normal tissue. The principles of phonosurgery aim to preserve the uninvolved epithelial covering, while removing an underlying lesion. Using this conservative approach, little or no trauma to the normal mucosa and superficial layer of the lamina propria should occur. For almost all benign laryngeal lesions, one should remain superficial to the vocal ligament, which will avoid scar formation, without stimulating fibroblasts in the intermediate layer of the lamina propria, or deeper. There is currently no role for stripping of mucosa of the vocal fold, for benign disease. Local anesthesia with sedation can be used to perform direct laryngoscopy for endoscopic microlaryngeal surgery, but this is not widely favored or practiced within the United Kingdom. Most endoscopic procedures for benign laryngeal pathology are performed under general anesthesia as a day case procedure. This requires a close working relationship and cooperation of both the otolaryngologist and the anesthetist for the shared airway. There are several approaches that can be employed and this is determined by the individuals’ experience and preference. Endotracheal intubation provides the safest, most stable ventilation under general anesthesia. A microlaryngoscopy tube, of 5.0 mm internal diameter, can be placed in the posterior glottis and usually provides an adequate view for most pathologies. If transoral laser surgery is planned, specifically designed laser-resistant endotracheal tubes can be used. An alternative approach is general anesthesia without intubation, using the Venturi jet ventilation technique, which allows for a clear view of the larynx. This can be delivered in one of two ways: supraglottic jet ventilation can be employed using a sanders jetting needle secured through a side-arm channel of the laryngoscope, positioned above the level of the vocal folds. This allows for a completely unobstructed laryngeal view for the surgeon. Alternatively, a disposable jet catheter can be placed through the vocal folds to deliver transglottic jet ventilation. The advantage of this is that jet ventilation is initiated below the level of the vocal folds, and therefore there is less mechanical interference at the vibratory margin, when performing surgery. Clinical Insights The author (K.G.) prefers supraglottic jet ventilation for laser-assisted surgery as this helps in the dispersal of plume from the surgical field. Delicate microlaryngeal surgery, however, is best achieved with subglottic tracheal jet ventilation. Technical advances and improved outcome assessments have resulted in great advances in phonosurgery. Suspension laryngoscopy, appropriate anesthetic techniques, microscopic vision, and our improved knowledge of laryngeal microanatomy have led to surgical refinements in endoscopic techniques, with a variety of alternative tools being used. The most widely practiced techniques include cold steel dissection and the carbon dioxide (CO2) laser. Cold steel dissection instruments have long been available. In recent times, these instruments have become more refined for the delicate microsurgery that is now practiced, and these should include a selection of sharp, precise microsurgery instruments. However, with the advent of high-magnification microscopes and high-precision microlaryngeal instrumentation, the carbon dioxide laser has become an alternative surgical tool, which should be used as a high-precision surgical knife, in experienced hands. However, the operating surgeon must have a good understanding of the effects of wattage, spot size, and mode (continuous or pulsed) and indeed the indications and limitations of this surgical tool. One important consideration is that the CO2 laser does introduce a potential risk of peripheral tissue damage, from dissipated thermal injury, and for this reason some laryngologists have traditionally not favored its use in benign laryngeal pathology. However, others argue that now with the advent of the microspot laser with a spot size of less than 250 μm, the potential heat distribution to the deepest layers of the lamina propria is significantly reduced, making this a safe and effective tool in patients with superficial benign vocal fold lesions. Furthermore, the newer microspot and scanning devices provide a range of spot sizes and laser beam shapes, which can enhance the delivery of laser energy while minimizing carbonization, charring, or thermal collateral effects. There is still much debate regarding the relative merits of these two mainstream techniques. Only a limited number of studies have directly compared the efficacy of microdissection with microspot CO2 laser surgery in the larynx, and these have consistently shown comparable results, with no significant differences in clinical outcomes between the two surgical tools.2,3 There are only two prospective randomized trials comparing CO2 laser surgery with conventional microdissection techniques. The first of these was reported in 1999 by Hörmann et al, who evaluated pre- and postoperative vocal function using direct videolaryngoscopy, maximal phonation, and speech and singing voice fields.4 The results from this study showed an improvement in postoperative vocal function with both techniques, but this was only statistically significant in their cold surgery group. A similar prospective randomized study was reported in 2000 by Benninger who compared aerodynamic, perceptual, and videostroboscopic outcome measures between microspot CO2 laser excision and cold steel microdissection for a variety of superficial benign vocal fold lesions.5 Interestingly, his data showed no demonstrable difference in clinical outcomes or indeed in the recovery time comparing the two surgical techniques. On balance, the literature largely supports the use of laser in the treatment of superficial benign laryngeal pathologies, and its use is now far more acceptable to most phonosurgeons. More recently, some surgeons now also advocate the use of powered instruments, such as the laryngeal microdebrider. This can be used for a variety of laryngeal pathologies, including malignancy. However, for benign lesions of the larynx, it is most widely used in the treatment of laryngeal papillomas. However, the safe and efficient use of this powered instrument requires a clear understanding of the instrumentation, including the different blade options and instrument settings. In recent years, the use of the microdebrider for laryngeal papillomas is becoming increasingly favored compared with the laser, as it avoids the risks of laser-associated thermal injury. A few retrospective studies have compared microdebrider with laser treatment for respiratory papillomas. These have shown that microdebrider resection was associated with significantly reduced operative times and potentially reduced cost implications,6 as well as a reduced incidence of soft-tissue complications.7 A more recent prospective study also supported the use of the microdebrider, as this was associated with significantly better objective voice outcomes postoperatively.8 The only randomized, prospective study comparing microdebrider with CO2 laser removal of recurrent respiratory papillomas also demonstrated greater improvement in voice quality and shorter procedure times,9 thus supporting the use of the microdebrider as a safe and potentially more cost-effective tool. Cautious use of this device is needed to avoid resection of normal epithelium. All techniques require extreme care and a skilled surgeon. Individually, they are all excellent tools if used in the correct way, with due consideration to the microanatomy of the vocal folds and the principles of phonosurgery. The use of all types of instrumentation should be within the armamentarium of every phonosurgeon, and the use of each tool should be modified according to the pathology that is being treated. Clinical Insights The author (K.G.) prefers the use of the CO2 laser particularly for extensive pathology or premalignant conditions of the larynx. Any surgical intervention on the free edge of the musculomembranous vocal fold requires great care, with laser settings adjusted to minimize collateral trauma. Use of lowest power settings to effect change to the lesion (~2.5 W) and in either single pulse or superpulse (0.4/0.1 seconds) minimize collateral trauma. Most recently, scanned beams of linear 1 or 2 mm length or curvilinear 1 to 3 mm length have provided an excellent tool for bloodless excision of benign lesions with hardly any trauma or disturbance of the adjacent vocal fold epithelium. Vocal fold nodules (singer’s nodules) are benign, localized, and superficial “growths” on the medial surface of the true vocal folds that are believed to result from phonotrauma. Nodules are typically bilateral and usually small and gray-white in color (Fig. 25.1), with hyperplastic epithelium and underlying chronic inflammatory infiltrate. They are classically located at the junction of the anterior and middle thirds of the vocal fold, i.e., midpoint of the membranous vocal fold, and are confined to the superficial squamous epithelium. Nodules are most commonly observed in middle-aged women and children (boys more frequently than girls), who are prone to vocal abuse. Figure 25.1 Bilateral vocal fold nodules. Patients with vocal fold nodules commonly present with dysphonia. This results from their effect on interrupting the vibratory pattern of the vocal fold from both their mass effect and impeding full glottic closure during phonation. Their occurrence is typically related to vocal abuse and misuse. Therefore, attention to underlying causative factors, through voice therapy and education, plays an integral role in the treatment plan. If diagnosed correctly, more than 90% will resolve or become asymptomatic with voice therapy alone. If, however, there is unacceptable vocal impairment despite compliance with medical treatment and voice therapy, surgery may be considered. The nodules can be removed using microsurgical techniques, with minimal normal tissue disruption, usually with cold steel microdissection, although the CO2 laser can also be used. The center of the nodule should be held with grasping microforceps and pulled medially toward the opposite cord. Microscissors can be used to cut the mucosa close to its base, thus preserving the normal mucosa. The opposite side nodule can also be removed at the same time. Postoperative voice rest is recommended for 48 hours and correction of voice production techniques with voice therapy is essential, to prevent recurrence. Vocal fold polyps are generally unilateral and represent localized areas of edematous polypoidal changes, superficial to the vocal ligament, usually resulting from phonotrauma. They typically involve the free edge of the vocal fold mucosa (Fig. 25.2), although they may also occur on the superior or inferior aspect of the vocal fold. They are more common in men, in smokers, and in the young and middle-aged groups. Careful examination may also reveal a contact response resulting in a “contrecoup” lesion on the contralateral vocal fold (Fig. 25.3). Figure 25.2 Left vocal fold polyp, arising from the free edge of the vocal fold mucosa.
Assessment
Anatomy
Principles of Phonosurgery
Anesthesia
Laryngeal Instrumentation for Dissection
Vocal Fold Nodules
Vocal Fold Polyps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


