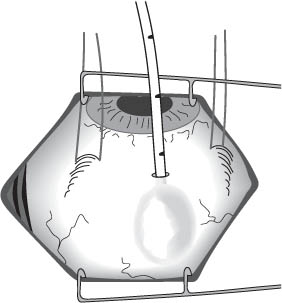
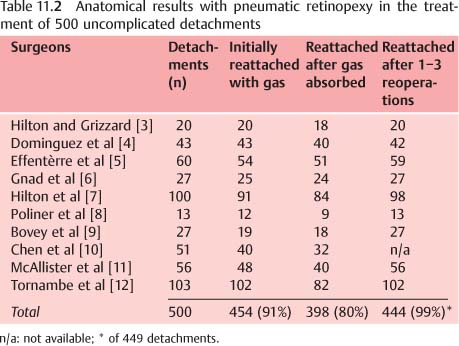
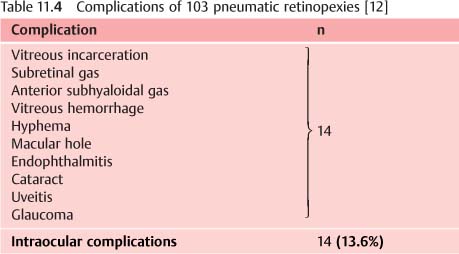
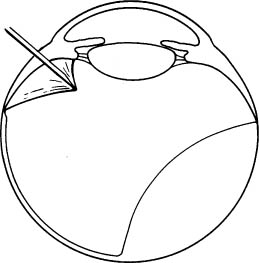
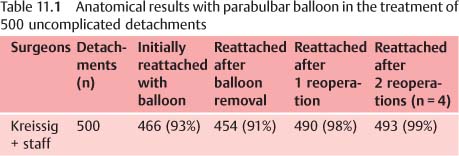
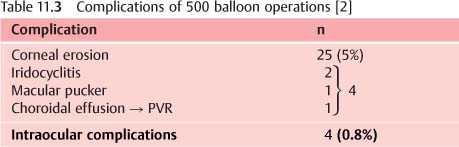
11 Balloon Buckle versus Pneumatic Retinopexy for Uncomplicated Retinal Detachments The balloon operation and pneumatic retinopexy represent minimal surgery. Both procedures are applied for uncomplicated detachments with breaks located within 1 clock hour. The operations are done with local anesthesia without drainage of subretinal fluid. Both provide a temporary tamponade during the time it takes for a cryopexy or laser application to form a retinal adhesion around the break. In contrast to the balloon procedure, pneumatic retinopexy requires the patient to maintain a prescribed head position for 1 week. The difference between the 2 procedures is apparent: The balloon procedure is extraocular. The conjunctiva is incised for the insertion, but the balloon catheter is positioned external to the scleral wall in the area of the break. Pneumatic retinopexy is an intraocular procedure; the scleral wall is perforated and the gas is injected into the vitreous. 1. Which procedure has the better reattachment rate? 2. Which procedure has the least number of complications? In Tuebingen, having experienced the complications of intraocular gas, i.e., PVR and new breaks [1], we switched in 1979 from the gas to the balloon operation for uncomplicated detachments [2]. The balloon operation can be used for superior and inferior breaks. But the gas operation is limited to detachments with breaks in the superior ⅔ of the retina. — With the balloon operation the catheter is inserted through a small incision in conjunctiva into the parabulbar space and the sclera is not perforated. The tamponade of the break or breaks is ab externo (Figs. 11. 1, 11. 2). — With pneumatic retinopexy a needle is inserted through the scleral wall into the vitreous. There are intraoperative complications, i.e., gas under the retina, incarceration of retina and vitreous, hemorrhage and infection, when injecting the gas bubble. The tamponade of the break or breaks is ab interno (Fig. 11.3). – With the gas operation the patient has to maintain a necessary head position: • Day and night. • For 1 week to provide the correct position of the gas bubble for a sufficient tamponade of the break or breaks during the time it takes to form a retinal adhesion. • To avoid closure of the anterior chamber angle by the gas bubble which, otherwise, would cause an abrupt rise in intraocular pressure. Fig. 11.1 Balloon operation implies an incision of 2 mm in conjunctiva and the balloon catheter with the stylette in place is inserted into the parabulbar space, positioned beneath the detached break and inflated with 0.7 ml of fluid after withdrawal of the stylette. There are no fixating sutures. Fig. 11.2 Schematic drawing depicting the inflated balloon after insertion into Tenon’s space and being positioned outside of the scleral wall in the area of the detached break. The parabulbar balloon represents a tamponade of the break (s) ab externo. Fig. 11.3 Pneumatic retinopexy implies perforating the scleral wall with a sharp needle (5 mm in length, if necessary shortened by a piece of silicone tubing) to inject the gas bubble into the vitreous via the pars plana. Pneumatic retinopexy represents a tamponade of the break (s) ab interno. The Figure also represents the risk one might encounter when injecting the gas into the eye. Prior to injection of the gas, one has to be certain that the tip of the needle has perforated a thin transparent membrane which might be adherent to the ciliary epithelium, otherwise the serious complication, “gas under the retina,” will result. As you see, there are already differences between the 2 procedures concerning their applicability, surgical technique and postoperative management. A total of 500 uncomplicated detachments (with 1 break or group of breaks within 1 clock hour) were operated upon with the parabulbar balloon by the author and the staff in Tuebingen; 500 comparable detachments were treated with pneumatic retinopexy by a group of experienced posterior segment surgeons in the United States and Europe [2]. The retina was reattached in 93%. After removal of the balloon, redetachment occurred in 2% (Table 11. 1). After 1 reoperation re-attachment was achieved in 98% and after a 2nd reoperation (n = 4 of 500) in 99%. But the following should be borne in mind: The final result of 99% retinal reattachment was obtained after 1 to 2 reoperations. The retina was reattached in 91%, however—and this is the crucial difference—after absorption of the gas redetachment developed in 11% (versus 2%) (Table 11. 2). Thus: A final reattachment of 99% with pneumatic retinopexy was obtained after 1 to 3 reoperations. Let me explain this to you. The main complication after the balloon operation is extraocular (Table 11.3): A superficial corneal erosion in 5%. It can be avoided, if the balloon catheter is directed away from the cornea at the end of the operation. After balloon operation intraocular complications were 0.8%. For comparison, the complications after pneumatic retinopexy are shown (Table 11.4): After gas intraocular complications were 13.6%, i.e., 15 times more frequent than after the balloon procedure. And here are the more serious complications concerning the retina: – After pneumatic retinopexy (Table 11.6) new breaks occurred in 15% (between 4% and 30%), and PVR in 4% (between 2% and 10%).
11.1 Introduction
 Why?
Why?
 To position the gas bubble into the area of the break or breaks to provide sufficient tamponade.
To position the gas bubble into the area of the break or breaks to provide sufficient tamponade.
 The following questions arise:
The following questions arise:
 To answer these questions the surgical results of 1,000 uncomplicated detachments were analyzed, of which 500 were treated with one procedure and 500 with the other procedure.
To answer these questions the surgical results of 1,000 uncomplicated detachments were analyzed, of which 500 were treated with one procedure and 500 with the other procedure.
11.2 Differences between Balloon Operation and Pneumatic Retinopexy
11.2.1 Application
11.2.2 Surgical Technique
11.2.3 Postoperative Management
 – With the balloon procedure the patient does not have to maintain a special position of the head postoperatively.
– With the balloon procedure the patient does not have to maintain a special position of the head postoperatively.
 Are there also differences concerning the surgical results?
Are there also differences concerning the surgical results?
 To answer this question, the postoperative results of the 2 series were analyzed.
To answer this question, the postoperative results of the 2 series were analyzed.
11.3 Clinical Studies
11.3.1 Results
 After balloon insertion
After balloon insertion
 After 1 balloon operation and removal of the balloon the retina remained attached in 91%.
After 1 balloon operation and removal of the balloon the retina remained attached in 91%.
 After pneumatic retinopexy [2–12]
After pneumatic retinopexy [2–12]
 After gas absorption, the retina remained attached in only 80%.
After gas absorption, the retina remained attached in only 80%.
 What was the cause of the different rate of re-detachments?
What was the cause of the different rate of re-detachments?
 The difference in morbidity between the 2 procedures.
The difference in morbidity between the 2 procedures.
11.3.2 Complications
 – After the balloon operation (Table 11.5) new breaks developed in 1.4% and PVR in 0.2%.
– After the balloon operation (Table 11.5) new breaks developed in 1.4% and PVR in 0.2%.
Balloon Buckle versus Pneumatic Retinopexy for Uncomplicated Retinal Detachments
 When comparing the results of both procedures what are the differences?
When comparing the results of both procedures what are the differences?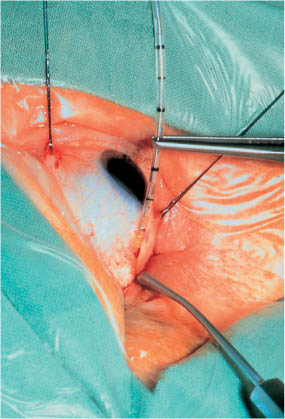
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


