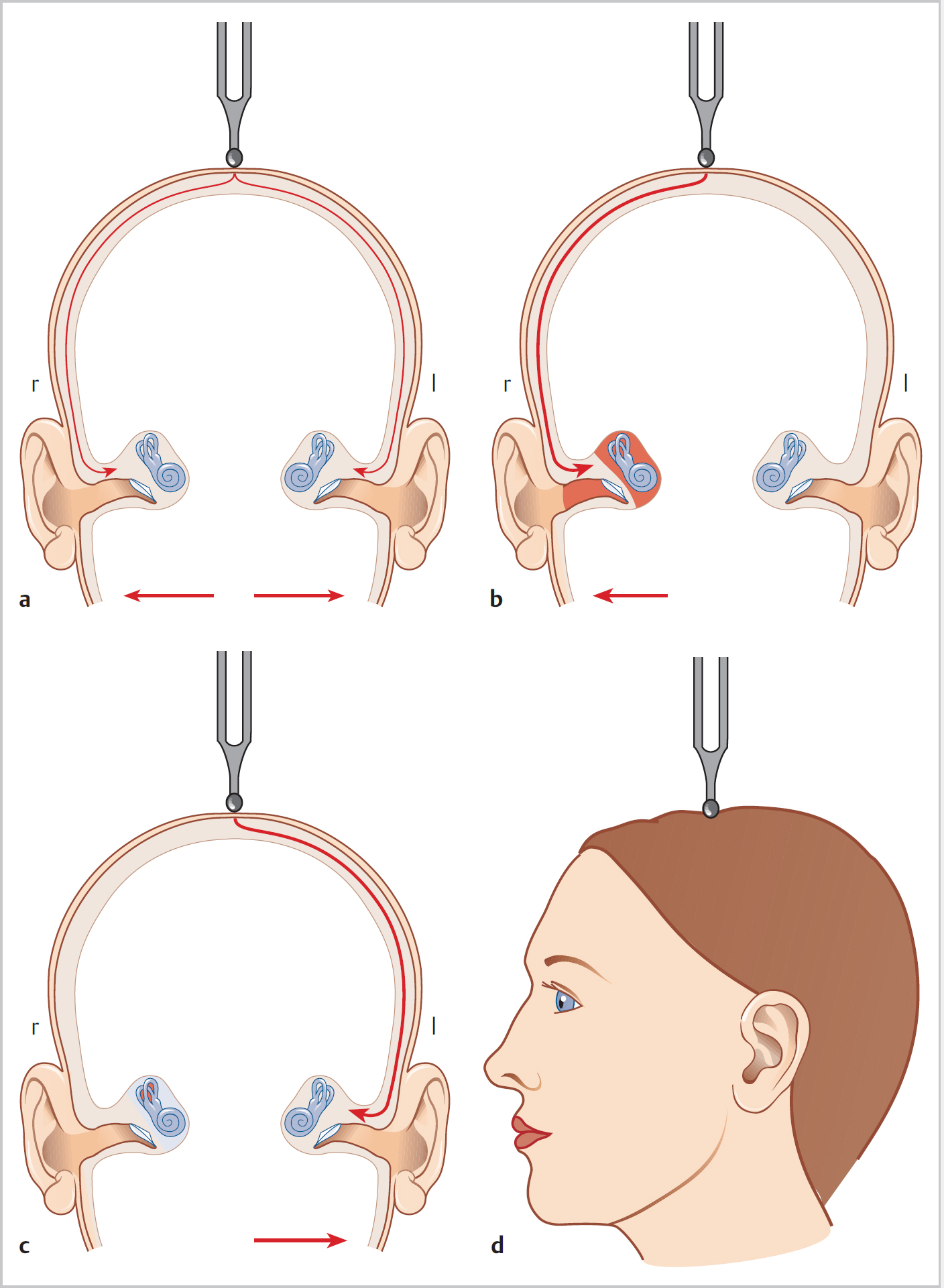
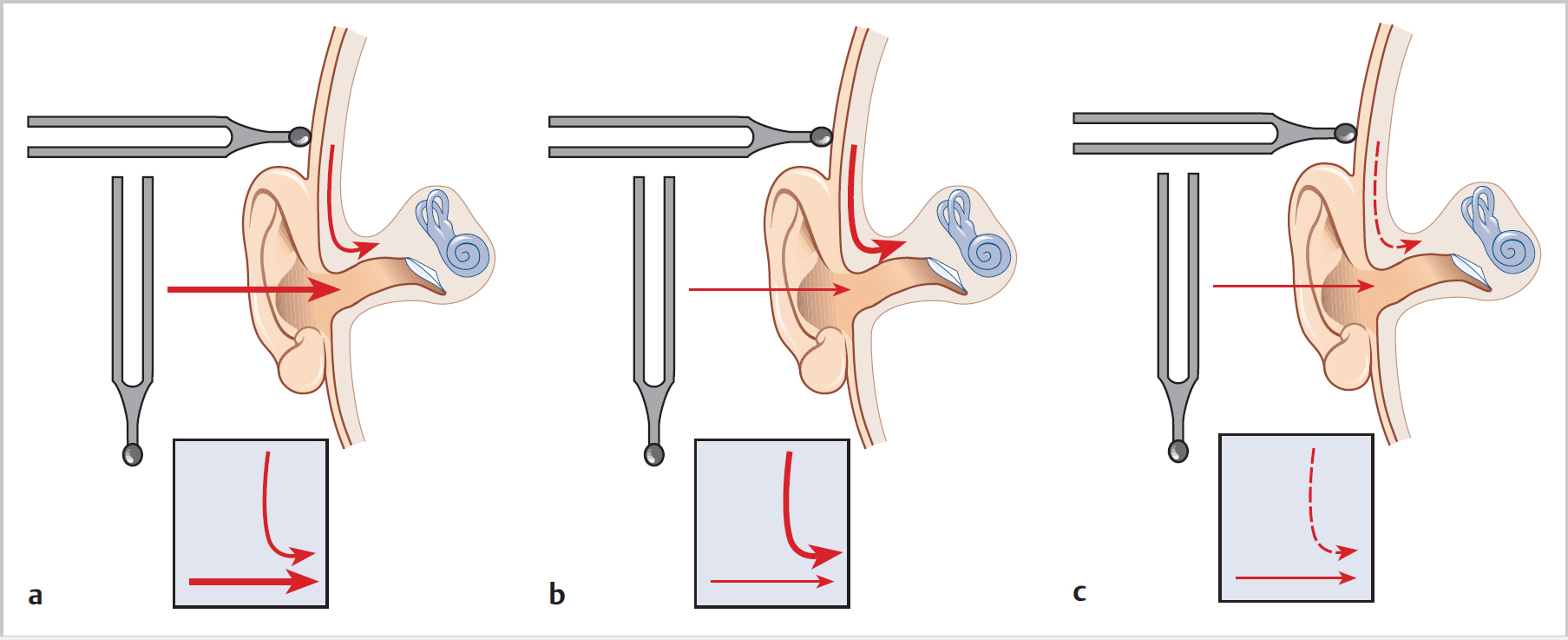
14 Audiology—Terminology and Tests • Subjective loudness is proportional to equal multiples of sound intensity • Bel = log10 (sound intensity/intensity reference (10–12 W/m2); 10 × ratio = dB • Sound intensity ∝ sound pressure2; sound intensity (dB) = 20 log10 sound pressure level • Doubling sound intensity = 3 dB increase; each 10 dB increase = 3.3 increase in sound pressure • Sound pressure level scale (dB SPL)—produces curved audiogram in normal circumstances because the auditory system is less efficient at detecting sounds at certain frequencies • Hearing level scale (dB HL/ISO)—designed so that 0 dB = expected threshold for every frequency—reference zero = group of otologically normal young adults; 0 dB HL is the intensity needed for a normal ear to perceive sound 50% of the time • A-weighted scale (dB A)—reduced contribution of the lowest and highest frequencies; used in industrial and noise-exposure settings • Free-field thresholds equate to the voice and distance level the subject gets >50% correct • Use number and letter combinations • Mask nontest ear with tragal rub (attenuate by ~50 dB) for whispered and conversational speech, Barany box (attenuates by ~90 dB when held at right-angle to ear) for loud voice • Test order: whisper 2 ft (60 cm) then 6″ (15 cm), conversation 2 ft then 6″, loud voice 2 ft then 6″ • If cannot hear whisper at 2 ft, subject is hearing impaired (normally can hear this at 12 ft [3.5 m]); if can hear this pure tone thresholds will be better than 30 dB • If hear whisper at 6″ or conversation at 2 ft 6″, threshold in range 30 to 70 dB HL • If only hear loud voice, thresholds >70 dB HL • Usually use 512-Hz tuning fork as tone does not decay too quickly or produce too much vibration • Activation by finger compression produces sound level ~70 dB; on knee (without pain) ~90 dB • Weber test (Fig. 14.1): • Rinne test (Fig. 14.2): • Stenger test: • A subjective test of a patient’s hearing compared with an established “normal” • Test performed according to standard protocols (British Society of Audiology) Fig. 14.1a–d The Weber test. A vibrating tuning fork is placed on the midline of the skull. a Equal loudness perceived in both ears means symmetrical hearing. b Lateralization of sound to the affected ear (right) is present in the case of conductive hearing loss. c In cases of sensorineural hearing loss, the sound is lateralized to the better ear (left). d Correct orientation of the tuning fork. • Soundproofed facilities needed for definitive/diagnostic testing • Test order of frequencies 1, 2, 4, 8 kHz then 500 and 250 Hz; repeat 1 kHz again to check within 5 dB of first result • Subjectively better-hearing ear tested first • Test to within 5 dB (to account for test–retest variability) • Testing involves ascending in 5-dB increments until patient gets 50% responses correct, then descending 10 dB and ascending in 5 dB again • BC at 250 Hz causes more vibration than sound, so test 0.5 to 4 kHz range (test–retest variability >10 dB, so differences only considered significant if at least this) • Subjective loudness sensation greater than expected with an increase in sound intensity Fig. 14.2a–c The Rinne test. Air and bone conduction are compared in the same ear. a Rinne positive, normally hearing ear. Air conduction is perceived louder than bone conduction in the test ear. b Rinne negative, conductive hearing loss. Bone conduction is perceived louder than air conduction. c Rinne positive, sensorineural hearing loss. Air conduction is perceived louder or longer than bone conduction (but the duration is shorter than in normal hearing).
14.1 Decibels and Decibel Scales
14.2 Clinical Hearing Testing
14.3 Tuning Fork Tests
 Tuning fork placed in midline
Tuning fork placed in midline
 With unilateral or asymmetric HL if conductive localizes to affected ear, if sensorineural localizes to nonaffected ear
With unilateral or asymmetric HL if conductive localizes to affected ear, if sensorineural localizes to nonaffected ear
 Can detect as little as a 5 dB loss, but error rate up to 25%
Can detect as little as a 5 dB loss, but error rate up to 25%
 Hold tuning fork next to ear, then onto mastoid process—which sound is heard loudest? (Originally described as fork held next to ear until no longer heard, then see if heard via bone)
Hold tuning fork next to ear, then onto mastoid process—which sound is heard loudest? (Originally described as fork held next to ear until no longer heard, then see if heard via bone)
 Positive when air conduction (AC) > bone conduction (BC); i.e., normal ears or SNHL in test ear
Positive when air conduction (AC) > bone conduction (BC); i.e., normal ears or SNHL in test ear
 Negative when BC > AC (conductive loss in test ear)
Negative when BC > AC (conductive loss in test ear)
 In dead ear get false negative due to transcranial stimulation of nontest ear; hence need to mask (e.g., with Barany box)
In dead ear get false negative due to transcranial stimulation of nontest ear; hence need to mask (e.g., with Barany box)
 Test less sensitive than Weber; for ABG 20 dB, sensitivity 50 to 70%, specificity ~95%; for ABG 40 dB, sensitivity and specificity ~95%
Test less sensitive than Weber; for ABG 20 dB, sensitivity 50 to 70%, specificity ~95%; for ABG 40 dB, sensitivity and specificity ~95%
 Can help detect patient with a nonorganic unilateral HL
Can help detect patient with a nonorganic unilateral HL
 Relies on fact that if pure tones of same frequency but different intensities are presented simultaneously to each ear, patient will only be aware of the louder stimulus
Relies on fact that if pure tones of same frequency but different intensities are presented simultaneously to each ear, patient will only be aware of the louder stimulus
 Present two tuning forks, but one to “deaf” ear closer; if genuine will hear fork in good ear, if “fake” will only be aware of sound in “deaf” ear so will deny hearing anything
Present two tuning forks, but one to “deaf” ear closer; if genuine will hear fork in good ear, if “fake” will only be aware of sound in “deaf” ear so will deny hearing anything
 Equivalent test can be performed with audiometer
Equivalent test can be performed with audiometer
14.4 Pure-Tone Audiometry (Fig. 14.3)
14.5 Loudness Recruitment
Audiology—Terminology and Tests
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


