26 Atypical Adenoma, Pituitary Carcinoma, and the Role of Chemotherapy in the Management of Refractory Pituitary Adenoma
 Pituitary Tumor Classification
Pituitary Tumor Classification
Pituitary adenomas are the most common intracranial tumors, and although they may cause significant morbidity due to hormonal hypersecretion or local mass effect, the overwhelming majority are typical adenomas confined to the sella. Pituitary carcinomas are very rare and are diagnosed when cerebrospinal or systemic metastasis is demonstrated. Pituitary carcinomas exhibit increased mitoses, Ki-67 labeling index (LI) >3%, and prominent nuclear staining for p53. Atypical adenomas are tumors that display a more aggressive phenotype characterized by early recurrence, local invasion of surrounding structures, or progression despite surgical resection, medical therapy, and radiotherapy.1 Like pituitary carcinomas, they are characterized by increased mitoses, Ki-67 LI >3%, and nuclear staining for p53. Atypical adenomas are believed to represent a biologically intermediate stage in tumor progression along the continuum from benign adenomas to carcinomas.2
However, the term atypical adenoma should not be confused with the term invasive adenoma as applied in the literature. Invasive pituitary adenomas, which infiltrate and destroy the dura, bone, blood vessels, and nerve sheaths, are relatively commonly encountered, with a variable incidence of 5 to 20%.3,4 If pituitary tumors exhibiting microscopic dural invasion are also included, up to 69% of microadenomas and 94% of macroadenomas can be termed invasive.5
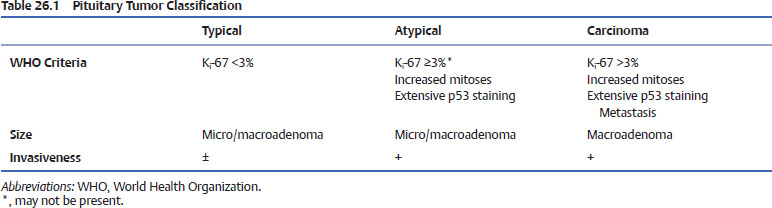
The 2004 edition of the World Health Organization (WHO) text Histological Typing of Endocrine Tumors incorporated advances in immunohistochemistry as a primary feature of distinction among these pituitary tumor types (Table 26.1). However, histopathologic evaluation of these tumors is not always able to clearly distinguish pituitary carcinomas from atypical pituitary tumors and typical adenomas.
Information about presentation, management, and treatment of atypical pituitary tumors and carcinomas is sparse and derived largely from isolated case reports and is thus somewhat limited. This chapter provides a general overview of the presenting features of each tumor type and discusses treatment options and outcomes for pituitary carcinomas based on this albeit scant and occasionally anecdotal literature.
 Pituitary Carcinomas
Pituitary Carcinomas
Epidemiology and Presenting Symptoms
Pituitary carcinoma is defined by the presence of a pituitary tumor that is either noncontiguous with the primary sellar tumor or has spread to sites distant from the primary. They are very uncommon and represent fewer than 0.2% of pituitary tumors. Up until 2008, there were only 124 reports of pituitary carcinoma in the literature describing a total of 154 patients.6–8 Due to the often silent nature of pituitary metastatic lesions, some cases may be missed, a contention supported by the diagnosis of pituitary carcinoma only after autopsy in up to 75% of cases reported prior to 1994.9 Occasionally, cancers of the breast, lung, kidney, and colon can metastasize to the sella or pituitary gland and are difficult to distinguish from primary disease.10,11 However, metastatic pituitary lesions typically cause partial or panhypopituitarism, particularly diabetes insipidus, which is rarely seen in primary pituitary carcinomas.10
No gender or ethnic predilection has been reported for pituitary carcinomas, and patients typically present in the third to fifth decades of life.8,12 Patients usually present with nonendocrine complaints due to local mass effect from the primary lesion, such as visual disturbances, with diplopia reported in 47% of cases and headaches in 27% of patients.8 As would be expected, the endocrine findings differ significantly depending on the type of tumor. Although nonfunctioning pituitary tumors are the most commonly encountered pituitary tumors, for unclear reasons the two most commonly occurring pituitary carcinomas are prolactin (PRL)-secreting and corticotroph-secreting carcinomas.8,12–14 Growth hormone (GH)- and gonadotropin-secreting carcinomas occur much less frequently, and, although reported, thyrotropinsecreting carcinomas are exceedingly rare.
Prolactin-Secreting Carcinoma
There are no particular factors that help differentiate PRL-secreting adenomas that will follow a benign course from those that will progress to carcinoma.15 Like their benign counterparts, PRL-secreting carcinomas present with PRL-mediated symptoms of amenorrhea, galactorrhea, or impotence, and PRL levels are largely similar to those in patients with typical macroadenomas.12 However, with disease progression, patients usually demonstrate persistently increasing PRL levels despite appropriate therapy, which is uncharacteristic of typical adenomas that usually respond extremely well to D2-agonist therapy in 85% of cases.16 In one series serum PRL levels ranged between 6 and 21,560 ng/mL.8
Corticotroph Carcinoma
Most adrenocorticotropic hormone (ACTH)-secreting pituitary carcinomas present with distant metastases and typical features of ACTH and cortisol excess, including moon facies, central obesity, abdominal striae, hypertension, diabetes, osteoporosis, altered menses, and delayed wound healing.8,13,17 Cases have also been reported in the setting of Nelson’s syndrome, whereby the ACTH-secreting pituitary tumor grows rapidly following adrenalectomy in patients with Cushing’s disease, leading to markedly elevated ACTH levels, often in excess of 100,000 pg/mL.8,18 In other cases of ACTH-secreting pituitary carcinomas clinical signs of Cushing’s syndrome are absent, characteristic of so-called silent corticotroph tumors, which even when nonmetastatic and confined to the sella often run an indolent course.19,20
Growth Hormone–Secreting Carcinoma
As of 2001, there were only 10 reported cases of GH-secreting carcinomas presenting with clinical manifestations of acromegaly and elevated levels of GH and insulin-like growth factor-1/somatomedin C (IGF-1/SmC).21,22 Unlike other pituitary carcinomas, GH-secreting carcinomas present at a relatively younger age, with an age range of 24 to 56.12
Gonadotroph Carcinoma
Gonadotroph carcinomas are rare, with only a few published reports, in which clinical symptoms included sexual impotence in males and oligomenorrhea in females.23–26 Variable levels of serum of luteinizing hormone, follicle-stimulating hormone, and α-subunit have been reported.23 Interestingly, one reported case presented with partial hypopituitarism, which as noted previously is an uncommon feature of pituitary carcinomas.23
Thyrotropin-Secreting Carcinoma
The first case of thyrotropin (thyroid-stimulating hormone [TSH])-secreting carcinoma was reported in 1993.27 On histology, the primary lesion stained positively for PRL, TSH, and α-subunit. Serum TSH levels were elevated and ranged from 16 to 31 mU/mL (normal 0.4–4.6 mU/L) and α-subunit levels were very high, ranging from 125 to 150 ng/mL (normal <5 ng/ mL). A possible case of a PRL-and TSH-co-secreting carcinoma was reported in 2007, although immunostaining of a resected brain metastasis was positive for PRL only.14 As of 2007, no other cases have been reported in the English-language literature, making this the rarest subtype of pituitary carcinoma.
Evaluation and Management
In the setting of atypical or suspected pituitary carcinoma, the extent of central nervous system (CNS) disease is best defined by magnetic resonance imaging (MRI).28 Pituitary carcinomas usually present in the setting of a known macroadenoma, exhibit significant suprasellar extension, and invade into either or both cavernous sinuses.8 Unless the index of suspicion is high, cervical or more distant spine imaging is not routinely performed, and evaluation is best guided by clinical symptoms (e.g., neck pain) or if there is discordance between the volume of tumor discernible and the biochemical markers. It is important to note that neuroimaging cannot distinguish a carcinoma from an adenoma, unless cerebrospinal metastasis is evident.29 Furthermore, systemic metastasis are not infrequently found incidentally during computed tomography (CT)/MRI scans for seemingly unrelated symptoms.
Pituitary carcinomas can metastasize either locally within the CNS via invasion into the subarachnoid space, leading to tumor seeding, or systemically via lymphatic and hematogenous spread.30,31 The extent of involvement can vary from a single lesion to widespread dissemination.13 Previously reported sites of metastasis have included the cerebral cortex, cerebellum, spinal cord, leptomeninges, eyes, heart, lung, cervical lymph nodes, pancreas, liver, kidney, pelvic lymph nodes, ovary, myometrium, and bone.32–35 There are also reports of metastatic pituitary carcinoma cells isolated from both cerebrospinal fluid (CSF) and pleural effusions.27,36
Pituitary carcinomas tend to disseminate systemically rather than via craniospinal spread, with a reported frequency of 47% for systemic metastases, 40% for craniospinal metastases, and 13% exhibiting both.8 Systemic metastasis appear to be more common in PRL-secreting carcinomas (71% in one series) with ACTH-secreting carcinomas exhibiting the second highest rates (57% in the same series), with a predilection for the liver.8 In contrast, GH-secreting carcinomas more commonly present with cerebrospinal metastasis, although it must be acknowledged that the number of patients included is low.12
Tumorigenesis
The mechanisms involved in the transformation of a typical pituitary tumor to an atypical tumor and particularly to pituitary carcinoma are poorly understood. Previously, concern was voiced that changes induced following radiation therapy or manipulation during surgical procedures played a role in the progression of these tumors. However, given the large numbers of pituitary adenomas that are routinely resected or irradiated in comparison with the small number of pituitary carcinomas reported, this relationship is unsubstantiated. Pituitary carcinomas are now thought to transform via progressive genetic mutations that arise in pituitary adenomas.1,12,26
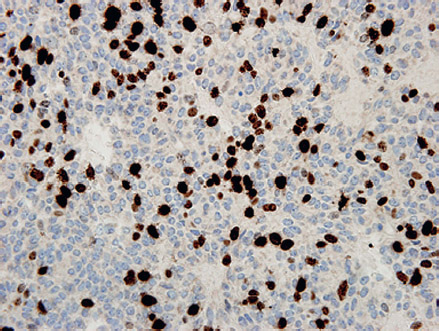
Fig. 26.1 Immunostaining for the proliferative marker Ki-67 in an atypical pituitary adenoma highlights approximately 25% of nuclei, a significantly higher index than the 1 to 2% immunopositivity of the usual adenoma. Original magnification (400×).
The time interval, or latency period, between the initial diagnosis of a pituitary adenoma and the occurrence of metastatic carcinoma varies considerably, ranging from 4 months to 18 years (mean 6.6 years).8 Some studies have identified variable latency periods for different tumor subtypes, with patients with ACTH-secreting adenomas having latency periods twice as long as those with PRL-secreting adenomas (9.5 versus 4.7 years).8
Role of Molecular Markers in Pituitary Tumors
Cell Atypia and Mitoses
Given the typically low proliferation rates in pituitary adenomas, most generally accepted morphologic and histologic criteria of tumor aggressiveness, such as the number of mitoses, the degree of nuclear pleomorphism or atypia, and necrosis, are of limited use in distinguishing pituitary carcinomas from typical or atypical pituitary tumors.37–39 For example, the presence of mitoses, which is considered a reliable marker of growth in many tumor tissues, may be scarce in aggressive pituitary tumors, and many of these changes are observed in both pituitary adenomas and carcinomas, which makes them of limited predictive value.7,36
Ki-67
Ki
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


