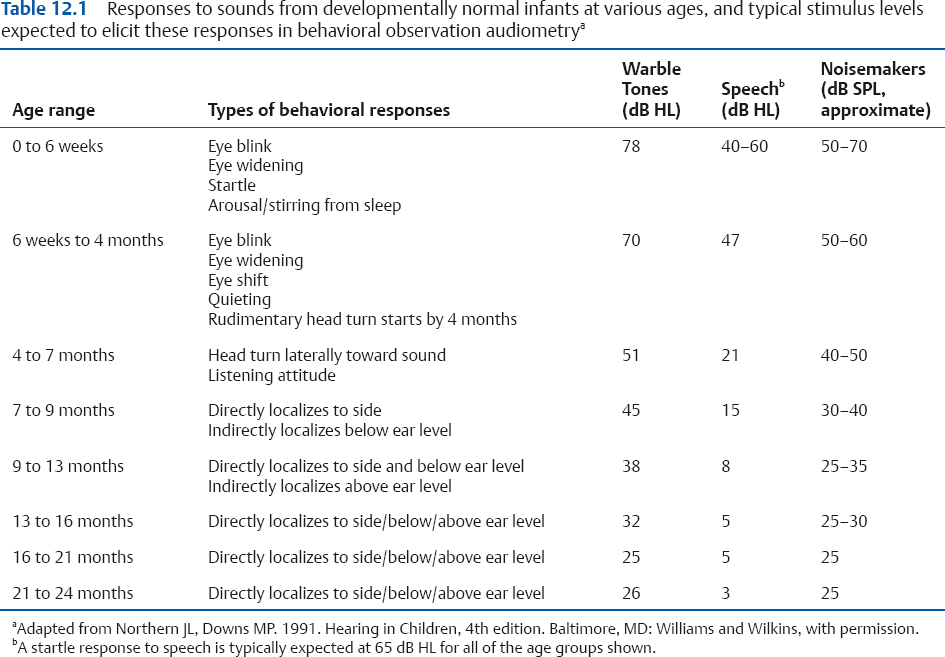
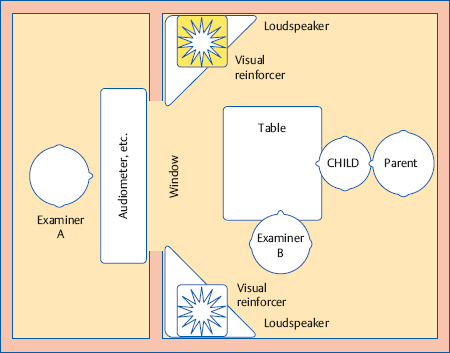
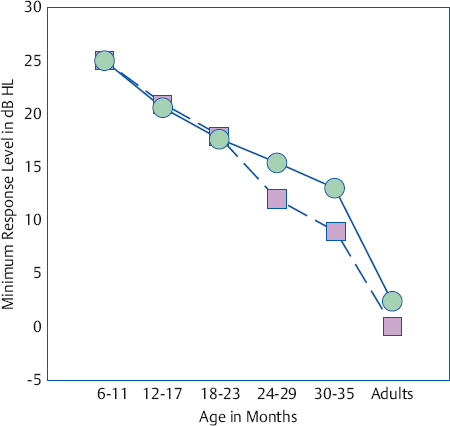
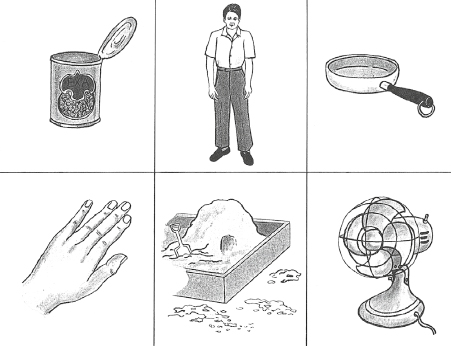
12 Assessment of Infants and Children This chapter is concerned with the audiological evaluation of children. Here, we are concerned with audiological procedures that have been modified or specially developed for use with infants and children at various levels of development, and with the clinical considerations that pertain to this population. The student should notice more than a few similarities between what is discussed here and what is covered in the context of audiological screening for children in Chapter 13. This is not surprising because screening tests are usually simplified and/or abbreviated clinical procedures. In fact, some procedures used for screening purposes are equally useful clinically. For example, the acoustic immittance methods used to screen for the presence of middle ear fluid are also used as part of the clinical immittance assessment and are often used to monitor a patient’s middle ear status over time. However, the greater depth and scope involved in clinical assessment and the knowledge and expertise demanded of those who accomplish it should be readily apparent as well. For example, the auditory brainstem response is used on a “pass/fail” basis for screening purposes, but its clinical use involves extensive and sophisticated testing procedures. Similarly, the screening use of the hearing loss risk factors enumerated in Chapter 13 is to indicate the need for a referral, but they are also used clinically as part of the case history that contributes to the diagnostic assessment of the child. By convention, children are considered infants from birth to 3 years old. The first 28 days of life are generally referred to as the neonatal period. They are preschoolers from ages 3 to 5, and school-age from then through high school. We will use these terms loosely because phrases like 2-week-old infant and 14-month-old child are self-explanatory. However, we must be aware of certain kinds of ages that have specific meanings and that are pertinent when dealing with children. For example, we are all aware that chronological age means age since birth, and that mental age expresses an individual’s cognitive ability (usually as measured on an intelligence test) in terms of the age when an average normal person achieves the same level of performance. Gestational age is the time period between conception and birth, and is conventionally measured from the time of the last menstruation until the time when the baby is born. Conceptional age is the child’s age measured from the date of conception; in other words, it includes the gestational age plus the time since the baby was born. Consider two babies born on the same day, one following a full-term pregnancy, and the other who was born one month early. Even though their chronological ages will be the same on the day when they eat their first birthday cakes, they will be 1 month apart in conceptional age (21 and 20 months). This difference brings us to the notion of developmental age, which is the individual’s age in terms of his level of maturation; for example, if a 12-month-old (chronologically) functions in a manner that is typical of the average normal 8-month-old, then his developmental age would be 8 months. For audiological purposes, it is often helpful to consider an infant’s prematurity-adjusted or corrected age, which is determined by subtracting the number of weeks of prematurity from his chronological age (e.g., Moore, Wilson, & Thompson 1977; Moore, Thompson, & Folsom 1992; ASHA 2004). The initial aspects of the audiological evaluation of a child involve obtaining a case history, carrying out a physical inspection of the ears and related structures, and taking the time to observe and informally interact with the child to develop a clinical impression of her developmental level and communicative abilities. The physical inspection of the ears and related structures is necessary to identify anomalies that affect audiological procedures, suggest the possibility of hearing-related abnormalities, and/or indicate the need for medical referral. The child’s case history is generally obtained from the parents or other caregivers, and should address the child’s medical history, her physical and neuromotor development, and her communicative behavior and development. As pointed out in Chapter 6, the specific material to be covered in the case history should come from a knowledge and understanding of auditory and related disorders (Chapter 6) and risk indicators (JCIH 2007; see Chapter 13, Table 13.2), and a firm background in child development in general and in speech-language in particular (e.g., Linder 1990; Nelson 1993). In addition to providing diagnostic insight, the history is used in combination with an informal observation of and interaction with the child to help determine what kinds of audiological testing methods might be most appropriate to use with her. It is so obvious that nobody expects an infant to raise her hand every time she hears a tone, that it seems ridiculous to say so. Yet what makes such a statement preposterous or humorous is a common albeit general understanding that there is a developmental sequence for what sounds babies will respond to and how they will go about responding. The details of this developmental sequence form the foundation for the audiological evaluation of infants and young children. Table 12.1 is an Auditory Behavior Index (Northern & Downs 1991) that summarizes many of the responses to sound expected from infants during the first 2+ years of life, along with the levels of various kinds of sounds expected to elicit these responses. Before proceeding to the details, it is a good idea to peruse this chart for several important general principles. First, notice that the earliest responses are gross, reflexive behaviors and that they become finer and more specific with the infant’s development. The behavioral assessment of hearing depends on knowing which responses to look for at which age range in the child’s development. In addition, the audiologist must also be alert for responses that are characteristic of children who are appreciably younger than the one being tested, indicating the possibility of developmental intellectual disorders or other developmental issue and the need for an appropriate referral. An example of such a developmentally delayed response would be an 18-month-old who can localize sounds to one side or the other, but not above or below eye level. Fig. 12.1 The improvement of infants’ minimum response levels with maturation from 6 to 35 months of age using visual reinforcement audiometry and adult thresholds for comparison. (Based on data by Matkin [1977].) Second, comparing the stimulus intensities needed for a normal infant to respond to warble tones versus speech or noisemakers reveals that infants are not equally responsive to all kinds of sounds. Third, looking down any of the three representative stimulus columns shows that normal infants elicit developmentally appropriate responses to sounds at progressively lower intensity levels with increasing age. This does not mean that the normal infant’s hearing sensitivity improves with age. Rather, it highlights the fact that we are often looking at the infant’s responsiveness to the presence of a sound, which must be distinguished from the threshold of hearing for that sound. Similarly, the lowest levels at which infants respond also tend to improve with increasing age, as shown in Fig. 12.1. In recognition of these points, the lowest level at which an infant produces a behavioral response at a given time is often called the minimum response level (MRL) rather than the threshold (Matkin 1977). Behavioral observation (or behavior observation audiometry, BOA) involves watching the baby’s responses to relatively sudden and intense stimulus sounds presented in the sound field, such as a speech signal (e.g., “bah-bah-bah”), warble tones, narrow band noises, and various hand-held noise-makers. Behavioral observation is preferred over the older term behavior observation audiometry, because it helps provide insight about the development of global auditory skills but does not actually involve hearing assessment (AAA 2012). Remember that sound field testing means that we do not know whether a response resulted from hearing in both ears or just one of them. The stimulus levels expected to elicit responses from normal infants at various ages are shown in Table 12.1. Because wide-band stimuli are being used, any information we might get about hearing in different frequency regions is limited at best. In addition, we must keep in mind that many of the toys used as noisemakers for behavioral observation are unstandardized sound sources, the characteristics of which are unknown to us unless we actually measure their spectra (which is done with embarrassing rarity). This is not a minor point because, for example, an apparently “high-frequency” toy may have a very complex spectrum including considerable energy at much lower frequencies than we might think. Behavioral observation should involve two examiners, typically one with the infant and the other in the control room with the audiometer, who observes the patient through the control room window. It is preferable for both examiners to be audiologists, but one audiologist and a knowledgeable and experienced assistant is a commonly used alternative. The infant should be placed on an examining table so that his whole body is clearly seen by both examiners. Depending on the infant’s age and state, it may be necessary for him to be held by a parent or an assistant, but it is essential for the person holding the child to not respond during testing. During the first 4 months of life the infant’s response may include any of several reflexes and a change in its state, either alone or in combination. Startle reflexes are often seen as a body shudder and/or considerable gross movements of the arms, legs, and/or the body. The startle response is often called the Moro reflex when the body is thrown into a hugging or embracing posture. Eye-related reflexes are often seen as well, and include eye blinks and opening or widening of the eyes. The reflexive contraction of the muscles around the eyes, producing a blink, is known as the auropalpebral reflex (APR). The startle and APR reflexes habituate rather quickly with repeated presentations of the stimulus sounds. Habituation means that the child stops responding after several stimulus presentations. The most typical changes in state that we watch for are arousal from sleep or stirring in response to the stimulus sound. Later during this period (between roughly 6 weeks and 4 months), we can observe quieting in response to the stimulus, eye shifts toward the sound source (the cochleo-oculogyric or auro-oculogyric reflex), and some rudimentary head turning toward the sound source. Although behavioral assessments provide insights about the infant’s auditory behavior and help us corroborate parent or caregiver reports, it is well established that they are simply too variable to provide reliable estimates of hearing sensitivity during the birth to 4 month period (Thompson & Weber 1974; Widen 1993; Hicks, Tharpe, & Ashmead 2000; ASHA 2004). Several sources of variability and subjectivity in behavioral observation have been outlined by Widen (1993). First, examiner judgments are subject to bias because the response itself can be elusive in the sense that it varies depending on such factors as the infant’s state and age, and with the nature of the stimulus. For example, decisions about the infant’s responses are biased by whether the examiner knows when the stimulus was presented (Ling, Ling, & Doehring 1970; Gans & Flexer 1982). Second, it is the infant’s responsiveness to the presence of sound rather than his threshold that is being measured, and this responsiveness differs for different kinds of sounds. Third, the intensity levels at which responses occur and the nature of those responses vary with the age of the infant. The fourth issue is that habituation leads to variability in the responses obtained from the same child. The fifth source of variability is that normal infants respond over such a wide range of levels that the examiner can be hard-pressed to tell when a given child’s responses are within or beyond the normal range. During the 4- to 7-month age period, the infant becomes more interested in softer sounds, an active listening attitude becomes apparent, and her neuromotor control matures to the extent that she begins to develop a localization response that involves turning her head toward the sound source. As shown in Table 12.1, these responses begin as horizontal localizations at ear level, and then mature to include localizations below (at ~ 9 to 13 months) and finally above ear level around 13 to 16 months. Testing approaches that make use of these localization responses are sometimes referred to as “localization audiometry.” When the infant reaches about 5 to 6 months of age, the localization responses are robust enough for us to move from behavioral observation, which involves the observation of unconditioned behaviors, to the use of conditioned responses. Hearing measurement using a conditioned localization response and a visual reinforcer is generally known as visual reinforcement audiometry (VRA) (Lidén & Kankkunen 1969). The basic approach was described by Suzuki and Obiga (1961), who called it the conditioned orientation reflex (COR). In their method, the child is placed in the test room with loudspeakers off to each side, as shown schematically in Fig. 12.2. Presenting a sound from one of the loudspeakers elicits an orientation or localization response from the child, which involves turning toward the stimulus speaker. This response is followed by the illumination of a visually appealing object that is associated with that loudspeaker, which serves as a reward or reinforcer. An example is shown in Fig. 12.3, where the visual reinforcer is mounted on top of each speaker. This process constitutes conditioning because the visual reinforcer increases the chances that the child will continue responding to subsequent stimulus presentations. Fig. 12.2 Typical testing arrangement for visual reinforcement audiometry, with the child sitting on its parent’s lap at a table. The reinforcer devices in this diagram are on top of the two corner loudspeakers. Some methods, like COR, use loudspeakers and reinforcers on one side, but many (though not all) contemporary VRA approaches place the loudspeaker and reinforcer(s) on just one side, which is represented by the brightly-filled star (representing that it is being illuminated). Various visual reinforcement audiometry approaches and testing protocols are available (e.g., AAA 2012; Day, Green, Munro, et al 2008; Haug, Baccaro, & Guilford 1967; Lidén & Kankkunen 1969; Moore, Thompson, & Thompson 1975; Matkin 1977; Diefendorf & Gravel 1996; Gravel & Hood 1999; Gravel & Wallace 2000; Widen, Folsom, Cone-Wesson, et al 2000; Widen, Johnson, White, et al 2005), of which the one developed by Moore et al (1975) is one of the most extensively documented and studied. The major characteristics of this VRA method are as follows: 1. A single loudspeaker and associated visual reinforcer(s) on one side are used; although it should be known that speakers and reinforcers on both sides are often used as well. The loudspeakers and reinforcers are often placed at 45° angles, as shown in Fig. 12.2, but 90° angles have been recommended so that the child’s head turn will be clearly observable (AAA 2012). 2. The reinforcement device usually is a toy that is illuminated and moves in place. Typical examples of these animated reinforcers include mechanical stuffed animals or a clown that plays the drums or cymbals (silently) when activated. The same switch activates the mechanical toy and the light. (Keep in mind that some children are frightened by clowns, so it is wise to ask the parents about this issue before using them as reinforcers.) The toy is mounted inside a dark Plexiglas box so that it is not visible until it is lit up for reinforcement purposes. A selection of several different animated toy reinforcers may be used instead of just one (e.g., Merer & Gravel 1997; Gravel & Wallace 2000; Widen et al 2005). 3. To be acceptable, the infant’s response must be a clear head turn toward the loudspeaker/reinforcer. 4. Responses are judged by two examiners. 5. There are clearly defined criteria for when the patient is considered to be conditioned (e.g., three correct responses in a row) and habituated (e.g., four nonresponses out of five consecutive trials). Depending on the infant’s age, neuromotor status, and state, she is seated on a chair (or on a parent’s lap), held, or placed on an examining table. The examiner with the infant usually manipulates quiet toys or pictures on a table in front of the child, which are used as midline distractors (AAA 2012) to keep her passively attendant and facing forward. The person holding the child should not respond during testing, and parents in particular must be instructed not to participate in the testing process. Thresholds may be obtained using modifications of conventional threshold search approaches, or with sophisticated programmed approaches (e.g., Bernstein & Gravel 1990). Unlike the usual “up 5 dB/down 10 dB” threshold method used in routine pure tone audiometry, visual reinforcement audiometry often involves an “up 10 dB/down 10 dB” or an “up 10 dB/down 20 dB” approach, or more sophisticated computer-assisted techniques (e.g., Gravel 1989; Eilers, Miskiel, Ozdamar, Urbano, & Widen 1991; Eilers, Widen, Urbano, Hudson, & Gonzales 1991; Gravel & Hood 1999; Tharpe & Ashmead 1993). On the basis of findings obtained using computer simulations, for example, Tharpe and Ashmead (1993) suggested that an efficient threshold testing strategy for visual reinforcement audiometry involves the following characteristics: (1) beginning the test without conditioning (i.e., training) trials in which the test tone and reinforcer are paired, (2) an initial test level of 30 dB HL (which is raised in 20 dB steps if there is no response at 30 dB HL), and (3) the use of an “up 10 dB/down 20 dB” technique. Fig. 12.3 An example of a typical illuminated visual reinforcer used in VRA. The characteristics of effective reinforcers were investigated by Moore et al (1977). They found that the highest rate of responses among 12- to 18-month-old infants occurs when using complex visual reinforcers such as toys that were lit up and moved in place. Progressively lower response rates are obtained with a simple visual reinforcer such as a flashing light; social reinforcers such as verbal praise, a pat on the shoulder, and/or smiling; and without any reinforcement at all. Video clips from movies or television shows that are appealing to young children provide another useful class of visual reinforcers (Schmida, Peterson, & Tharpe 2003; Lowery, von Hapsburg, Plyler, & Johnstone 2009; Karzon & Banerjee 2010). Visual reinforcement audiometry can be effective with full-term infants who are at least 5 to 6 months old (Moore et al 1977) and is typically recommended up to roughly 24 months of age (ASHA 2004; AAA 2012). Babies who were born prematurely can be expected to respond effectively to VRA at a corrected age of 8 months (Moore et al 1992). Recall that the corrected age is the child’s chronological age minus the estimated number of weeks of prematurity. One- and 2-year-olds tend to be conditioned for visual reinforcement audiometry quickly and easily, and are similar in terms of the rate of conditioning (how quickly they learn to perform the task) and the consistency of their responses (Primus & Thompson 1985). Unfortunately, however, infants do not continue responding to the stimulus forever. Instead, their responses habituate, or die out, as the stimulus trials are repeated over the course of the testing session. Habituation occurs more quickly for 2-year-olds than for 1-year-olds (Primus & Thompson 1985; Thompson, Thompson, & McCall 1992). Habituation is a major consideration with young children because the amount of information we can get about the child’s hearing depends on how many times he will respond. The number of responses obtained before habituation occurs can be increased by using different reinforcers instead of using just one (e.g., Primus & Thompson 1985; Thompson et al 1992). Giving the child a 10-minute break after habituation has occurred and then beginning a second test session significantly increases the total number of responses obtained from 1-year-olds, but not from 2-year-olds (Thompson et al 1992). Culpepper and Thompson (1994) showed the number of responses from 2-year-olds before habituation increased as the duration of the reinforcer was reduced from 4 seconds to a half-second. Tangible reinforcement operant conditioning audiometry (TROCA) (Lloyd, Spradlin, & Reid 1968) is a highly structured testing approach originally described for use with difficult-to-test patients, such as those with developmental disabilities. Difficult-to-test is a general term used to mean those who cannot be readily assessed with conventional behavioral tests, so that special methods are needed. Patients may be difficult to test due to physical, developmental, perceptual, cognitive, emotional, or other problems, or to any combination of these factors. Approaches like TROCA, which were developed for the difficult to test, are also effective with normal young children. Upon hearing a tone (or other test signal), the child is required to push a response button or to make another simple but specific motor response within his range of neuromotor capabilities. Correct responses are reinforced by the delivery of a tangible reward, which might be cereal, candy, tokens, or other small trinkets. False-positive responses are discouraged because they are followed by time-out periods. The entire procedure is accomplished with instrumentation programmed to present the stimuli, monitor the responses, and deliver the reinforcers according to a predefined operant conditioning schedule. In visual reinforcement operant conditioning audiometry (VROCA) (Wilson & Thompson 1984; Thompson, Thompson, & Vethivelu 1989) the child is required to press a response button (which is a large, bright box) instead of turning toward the loudspeaker, after which a visual reinforcer is presented. The visual reinforcer itself is the same kind used in visual reinforcement audiometry. When VROCA is employed with sound field testing, the loudspeaker is kept in front of the child so he is not distracted from the response box, as opposed to being placed off to one side as is done for a head turning response. Conditioned play audiometry, or play audiometry, involves training the child to listen for stimuli and then make a specific motor response within the framework of a game, usually in combination with social reinforcement such as smiles, praise, etc. For example, the child might be trained to place a peg into a pegboard after each test sound. Other commonly used games include stacking blocks or cups, placing small items into a container (or taking them out), or just about any other simple activity that can be repeated over and over again. Play audiometry is often appropriate for children between about 2 and 5 years of age (Northern & Downs 1991; AAA 2012). However, one should keep in mind that this is a wide age range as far as child development is concerned; and it is not surprising to find that the successful use of conditioned play audiometry improves with age, especially beyond the second year (e.g., Nielsen & Olsen 1997). Hence, we should not expect that all youngsters will be ready to be conditioned for play audiometry at age 2 (Thompson et al 1989). If at all possible, the mother or father should not be in the room during play audiometry. Parents in the control room are also undesirable, especially if the child can see them through the observation window. A parent who simply must be in the room should be seated quietly out of the child’s direct line of sight, and instructed not to interact with the child or participate in the testing process in any way. Play audiometry employs two clinicians who communicate by intercom and visually through the window between the control and test rooms. One of them operates the audiometer and the other stays with the child. The child is generally seated at a small table, which is the play surface, either next to or opposite one of the examiners. A collection of games should be kept on hand so that when the child gets bored with one activity you can quickly and smoothly replace it with another. Keep the backup games out of sight so they do not distract the child from the task at hand. If accepted by the child, earphone testing may be attempted at the start, or at least as soon as possible. Some children accept earphones immediately. In other cases, getting the child to accept earphones is a challenge in which the audiologist’s personal “way with kids” comes to the fore. A knowledge of the most current children’s cartoon series and action toy fads is a valuable asset in this context. Earphone acceptance is sometimes facilitated if the clinician first puts on her own headset (which houses the intercom and permits her to monitor the test signals). A reasonable amount of good-natured firmness and confident tenacity often works, but keep in mind that “winning” means getting the child to cooperate sufficiently that valid and reliable audiological information can be obtained, which will not happen if he is crying hysterically. If earphones are simply out of the question, then in the most matter-of-fact manner try the bone-conduction vibrator or insert earphones. If all reasonable attempts fail, simply place the headset on the table where the child can see it, and start the test in sound field. The goal is to condition the child to perform a specific, observable action every time he hears a tone, and then to manipulate the level of the tone to find the child’s threshold. The basic game used in conditioned play audiometry involves having the child hold a peg up to his ear while listening for a tone, and then placing it into a hole in the pegboard when a tone is heard (or adding it to a pile, etc.). Tell and demonstrate what to do. Then tell the child it is now his turn. It is often necessary to take the child’s hand and lead him through the task physically at first while verbalizing what he is doing. Then let him try. Praise the child for doing the task correctly. Reinstruct the child if necessary (this usually involves reminding him to wait for the tone before responding), but keep the emphasis on reinforcing the desired behavior. Once the child has learned the task, we need to obtain thresholds efficiently before habituation occurs. Northern and Downs (1991) recommend starting in the 40 dB HL to 50 dB HL range and descending in 10 or 15 dB steps, and then using ascending presentations to find the threshold, with two responses as the criterion; or one may use the threshold search methods described earlier in the section on visual reinforcement audiometry. Habituation will most likely limit the number of thresholds that can be obtained in any one session, which means we must begin testing at the frequencies that will provide the most information about the child’s audiogram as quickly as possible. For this reason it is usually desirable to obtain thresholds at 500 and 2000 Hz for both ears first. The other frequencies can then be filled in as long as the child remains “on task.” Northern and Downs recommended that these frequencies generally be added in the following order: 1000 Hz, 250 Hz, and 4000 Hz. Physiological methods are playing an increasing role in the audiological evaluation of infants and young children. These allow us to assess neonates and younger infants in ways that cannot be done by behavioral observation audiometry because they (1) do not require the child’s cooperation, (2) allow us to test each ear individually, and (3) directly assess the physiological integrity of at least the lower portions of the auditory system. On the other hand, we must keep in mind that physiological measurements give us a limited perspective of the infant’s world of sound because they do not involve a behavioral response. As previously indicated, physiological tests are often useful even with children who can be tested with behavioral methods, because they provide us with valuable cross-checks on the behavioral results (Jerger & Hayes 1976; ASHA 2004; JCIH 2007; AAA 2012) and also provide additional differential diagnostic information. The physiological tests regularly used in pediatric audiology include the auditory brainstem response (ABR), auditory steady-state response (ASSR), otoacoustic emissions (OAEs), and acoustic immittance tests. The later evoked potentials (see Chapter 11) are not routinely used with infants and younger children because they are affected by sleep and sedation. This is a significant factor because it is often necessary for young children and difficult-to-test patients to be asleep or sedated for results to be obtained. (This involves the participation of a physician because sedation and other forms of anesthesia are medical activities.) However, the later evoked responses cannot be totally discarded for use with young children. For example, Shimizu (1992) pointed out that it is possible to obtain cortical evoked potentials from young children during certain sleep stages, and that this can provide important information, particularly in children with absent ABRs. Other physiological approaches have also been used in the past. Examples include the monitoring of respiratory and/or cardiac responses to sound (Bradford 1975; Eisenberg 1975) and the psychogalvanic skin response (PGSR) (Ventry 1975). These methods were more cumbersome and less practical than modern approaches, in addition to which the PGSR was unnecessarily traumatic for the child. Although there are maturational effects that must be considered, the auditory brainstem response (ABR) and the auditory steady-state response (ASSR) are particularly well suited for use in pediatric audiology (Jacobson 1985; Dimitrijevic, John, Van Roon, et al 2002; Stapells 2002; Hall 2006; ASHA 2004; Rance, Tomlin, & Rickards 2006; Picton 2007; Sininger 2007; JCIH 2007; AAA 2012; see Chapter 11). Very young as well as seriously disabled children can be tested by ABR and ASSR because they do not involve a behavioral response and they are reasonably unaffected by sleep and sedation. Both techniques provide separate results for each ear. Frequency-specific results are needed to estimate the audiogram, and are provided by the ABR using tone burst stimuli or with the ASSR. Diagnostic information about the child’s neurological integrity at the brainstem level is provided by the ABR when click stimuli are used. Moreover, ABR and ASSR testing with bone-conduction stimuli in addition to air-conduction signals allows us to assess the type of hearing loss. Distortion product (DPOAE) and transient-evoked (TEOAE) otoacoustic emissions, described in Chapter 11, have considerable value in pediatric audiological assessment (e.g., ASHA 2004; JCIH 2007; AAA 2012). In contrast to the ABR, acoustic reflexes, and other tests that rely on both sensory and neural activity, otoacoustic emissions are “preneural,” relying only on the integrity of the cochlea before the auditory nervous system gets involved in the processing of a signal; hence, they can be measured even when there are neurological deficits that affect other measures. Otoacoustic emissions do not require a behavioral response, are reliably obtained in normal infants and young children, are very sensitive to hearing loss, are obtained separately for each ear, and can provide information at different frequencies. Tympanometry and acoustic reflex tests are a central part of the evaluation of infants and young children. The use of acoustic immittance tests with infants and children is covered in Chapter 7. Acoustic immittance measurements allow us to monitor middle ear conditions over time, and also can provide us with information about the status of the middle ear when reliable masked thresholds cannot be obtained, as is often the case with very young children. Acoustic reflex measurements provide information about the integrity of several aspects of the peripheral ears and lower parts of the auditory pathway, and also help us distinguish between the presence and absence of significant amounts of hearing loss. Speech signals are used in the behavioral assessment of infants and children from birth onward. The initial use of speech may be to elicit a startle response from a neonate; months later, speech signals may be used to elicit localizing behavior. Olsen and Matkin (1991) have suggested some guidelines for determining the threshold for speech depending on the child’s overall level of functioning, which is effectively her developmental age. As with other aspects of assessment in pediatric audiology, there is no clear line of demarcation between the times when one type of method or the other should be used, which is implied by Olsen and Matkin’s subtle use of overlapping age ranges. They recommended that a speech detection threshold (SDT) using a repetitive speech utterance be obtained from children who are functioning below the 3-year-old level. The speech detection threshold is obtained using the same kinds of techniques described earlier in this chapter. Unconditioned responses are used for those functioning at the lowest developmental levels, whereas conditioned responses can be obtained from children who can be tested by VRA, play audiometry, TROCA, or VROCA. A modified speech recognition (reception) threshold (SRT) can be obtained from many children from ~ 30 months to roughly 6 years old. This can be accomplished by, for example, presenting a group of easily recognizable objects or pictures that depict words selected to be within the child’s receptive vocabulary (e.g., a toy airplane, baseball, cowboy, toothbrush, etc.) and having her identify them as they are named by the examiner. It is also possible to have a child respond by pointing with an eye gaze in the direction of a selected picture (Byers & Bristow 1990). This kind of technique can be used for testing either speech thresholds or word recognition performance, and is useful with some children regardless of age (and adults, for that matter) who have cerebral palsy or other disorders that prevent them from pointing manually. Older children within this range are often able to give a verbal response to selected spondee words. A conventional SRT can often be obtained from children who function in the 5- to 10-year-old range, although a children’s spondee list is recommended for them. A list of spondee words considered to be within the receptive vocabularies of most children (ASHA 1988) is included in Appendix B. A conventional SRT based on standard spondee word lists is expected from children functioning at the level of 10 years and above. Testing the speech recognition threshold by bone-conduction and comparing it to the air-conduction SRT can provide insights about the type of hearing loss, which can be quite valuable if reliable tonal results have yet to be obtained (Olsen & Matkin 1991; Northern & Downs 1991). However, calibration values for speech presented via the bone-conduction vibrator must be determined empirically before this procedure is used. In general, speech recognition tests (Chapter 8) are used to reveal the accuracy of the patient’s auditory reception and processing of speech material, usually in terms of a percent correct score for monosyllabic words. This can be problematic when testing children because their speech recognition scores are affected by their level of language development as well as by their auditory capabilities. As a result, normal children’s speech recognition scores on many tests increase as they get older, eventually becoming comparable to adult scores at roughly 10 to 12 years of age, when they are familiar with most if not all of the test words. The situation is exacerbated in patients who have speech-language disorders, or other problems that impair either the level of linguistic functioning or the ability to respond during the test. In addition, we must remember that speech-language disorders are common among children with significant amounts of hearing impairment. Consequently, we should try to use speech recognition tests that include words within the child’s receptive vocabulary and employ responses that she is capable of making, at least to the extent that this is possible. Moreover, in light of the fact that practical tests often cannot realize these lofty goals, we must consider the individual child’s receptive vocabulary and response limitations when interpreting and reporting speech recognition test results. Several open-set tests are available for children who are not ready for adult speech recognition measures. Recall from Chapter 8 that the open-set format is essentially the same as a fill-in test. The speech recognition ability of children who are ~ 6 to 9 years old can often be tested with the Phonetically-Balanced Kindergarten or PBK-50 lists (Haskins 1949). The PBK-50 test is made up of 50-word lists based on a kindergarten-level vocabulary, and the word recognition score is simply the percent of the words that were repeated correctly. The four PBK-50 lists are included in Appendix K. Although PBK-50 lists 1, 3, and 4 are usually considered to be equivalent, list 2 is rarely used clinically because Haskins found it to be easier than the other three. Meyer and Pisoni (1999) demonstrated that compared with the words in the other three “equivalent” lists, the words in the easier list 2 have a higher frequency of occurrence and are less likely to be confused with other words. Boothroyd’s isophonemic word lists (Boothroyd 1968, 1970, 1984; Boothroyd & Nittrouer 1988) can also be used with children in this age range. The isophonemic word test was discussed in Chapter 8, and may also be found in Appendix H. Each isophonemic word test list includes 10 consonant-vowel-consonant (CVC) words that are scored on a phoneme-by-phoneme basis. In other words, scores on the isophonemic word test are based on 30 phonemes. The Lexical Neighborhood Test (LNT) and the Multisyllabic Lexical Neighborhood Test (MLNT) were developed to facilitate the assessment of children with profound hearing losses with cochlear implants (Kirk, Pisoni & Osberger 1995; Kirk 1999; Kirk, Eisenberg, Martinez, & Hay-McCutcheon 1999). Because many of these children have limited vocabularies, the words on these tests were chosen from those known to be familiar to 3- to 5-year-olds based on Logan’s (1992) analysis of the Child Language Data Exchange System (CHILDS) database (MacWhinney & Snow 1985). The LNT includes 25 lexically hard monosyllabic words and 25 lexically easy monosyllabic words. (Recall that words with a high frequency of occurrence and few similar-sounding alternatives are lexically easy, whereas low-frequency words with many alternatives are lexically hard.) Instead of using monosyllabic words, the MLNT involves presenting 24 two- and three-syllable words. As with the LNT, half of the words on the MLNT are lexically hard and half are lexically easy. The two LNT and MLNT lists are shown in Appendices I and J. Several closed-set or multiple-choice format monosyllabic word recognition tests are available for children who are at least about 3 years of age. The most widely used tests of this type are the Word Intelligibility by Picture Identification (WIPI) Test (Ross & Lerman 1970, 1971), the Northwestern University Children’s Perception of Speech (NU-CHIPS) Test (Kalikow, Stevens, & Elliott 1977; Elliott & Katz 1980), and the Pediatric Speech Intelligibility (PSI) Test (Jerger, Lewis, Hawkins, & Jerger 1980; Jerger, Jerger, & Lewis 1981; Jerger & Jerger 1984), although others are also available. In the WIPI test, the child points to a picture that corresponds to the stimulus word from a choice of six color pictures. Each set of six pictures is arranged on the same page of a test book. An administration of the WIPI includes 25 items, and there are four test lists. Fig. 12.4 shows an example of a response plate from the WIPI test, and the test words are listed in Appendix L. The NU-CHIPS test is made up of 50 words that are within the receptive vocabularies of inner-city 3-year-olds, which are listed in Appendix M, including four recorded randomizations of these words. The child is presented with a page showing four picture choices for each test word, as in Fig. 12.5, and responds by pointing to the picture that corresponds to the test word. The material in the PSI test was derived from the vocabularies and sentence structures used by normal 3- to 6-year-old children. The test words are 20 monosyllabic nouns. The child responds by pointing at the picture corresponding to the test word or sentence. Two sentence formats may be used on the PSI test, depending on the child’s language level, which are referred to as Format I (e.g., “Show me a bear combing his hair”) and Format II (e.g., “A bear is combing his hair”). Other speech recognition tests have also been developed for use with children. For example, the Auditory Perception of Alphabet Letters (APAL) Test can be used for younger children who are familiar with the alphabet even if their vocabularies are inadequate for word recognition testing (Ross & Randolf 1988). Robbins and Kirk (1996) described a technique for assessing speech recognition in pre-schoolers with limited vocabularies by having them follow verbal directions to assemble the familiar Mr. Potato Head toy. A number of speech recognition tests for children employ a sentence format. Weber and Redell (1976) devised a modification of the WIPI test in which the test items are presented in a sentence format. Another children’s sentence test was developed by Bench, Kowal, and Bamford (1979) and is called the BKB Sentences Test. One version of the BKB test is composed of 16 sentences that are presented to older children in an open-set format, and the test is graded on the basis of how many key words are repeated correctly. The other version is intended for use with younger children and involves a picture pointing response. The Hearing in Noise Test for Children (HINT-C) (Nilsson, Soli, & Gelnett 1996) is a pediatric version of the Hearing in Noise Test (HINT) (described in Chapter 8) and is used to measure the SRT for sentences.
 Behavioral Assessment
Behavioral Assessment
Behavioral Observation
Visual Reinforcement Audiometry

Tangible and Visual Reinforcement Operant Conditioning Audiometry
Conditioned Play Audiometry
 Physiological Measures
Physiological Measures
Auditory Evoked Potentials
Otoacoustic Emissions
Acoustic Immittance
 Speech Audiometry
Speech Audiometry
Threshold for Speech
Speech Recognition
Open-Set Tests
Closed-Set Tests
Sentence Tests
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


