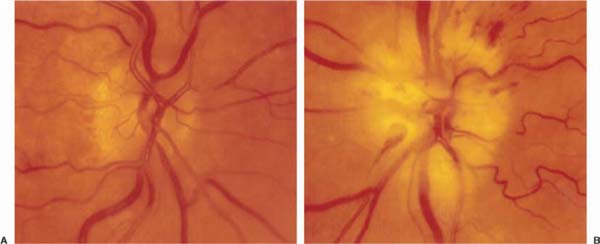
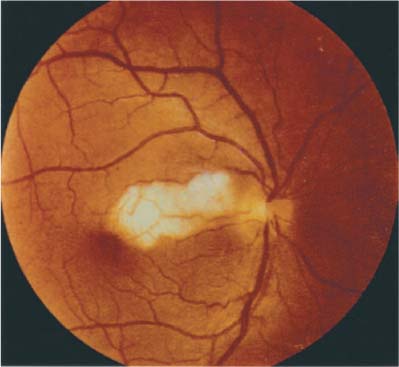
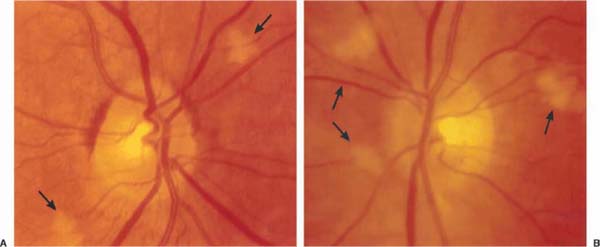
Chapter 18 Arteritic anterior ischemic optic neuropathy (arteritic AION) causes ischemic damage to the optic nerve secondary to the disease giant cell arteritis (GCA). It presents as unilateral or bilateral severe visual loss in isolation or in the context of other symptoms of GCA. Initial evaluation is directed at confirming visual loss from optic nerve infarction or choroidal infarction, obtaining a complete review of systems looking for other systemic symptoms commonly seen in the disease state, and obtaining confirmatory laboratory studies. When the suspicion of arteritic AION is high, IV methylprednisolone or high-dose prednisone should be started immediately.1 The patient referred with suspected arteritic AION should be sent for a STAT complete blood count (CBC) and sedimentation rate, and evaluated by an ophthalmologist the same day. Immediate evaluation is imperative in hope of preventing visual loss in the unaffected eye. Arteritic AION occurs almost exclusively over the age of 60 and in women more often than men. The incidence rises with increasing age. Acute severe visual loss occurs in one or both eyes, and may be preceded by transient monocular visual loss.2 Visual loss usually involves both central and peripheral visual fields, with central visual acuity measuring <20/200 in the majority of cases. Severe, constant headache, associated with scalp and temporal tenderness, is a frequent accompaniment of the optic neuropathy. Jaw claudication is less common, but is highly specific for arteritis. • Anorexia and weight loss • Generalized malaise and fatigue • Generalized muscle and joint pain exacerbated by movement (e.g., turning over in bed) • Fever and night sweats Visual acuity is frequently severely diminished, with the majority of patients <20/200. Although altitudinal visual field loss is the most common pattern in nonarteritic AION, severe generalized depression of the visual field is more common in the arteritic form. A prominent afferent pupillary defect is invariably present if there is unilateral or bilateral asymmetric disease, but not if there is bilateral symmetric disease. Diffuse pallid swelling of the optic nerve is invariably present, often associated with severe vascular narrowing, flame hemorrhages, and cotton wool spots (Fig. 18–1). Occasionally, optic neuropathy occurs in the absence of disc edema, so-called posterior ischemic optic neuropathy. Occasionally, optic neuropathy occurs in the absence of disc edema, so-called posterior ischemic optic neuropathy. If there is occlusion of the central retinal or a cilioretinal artery, retinal edema with a cherry-red spot may result (Fig. 18–2). Prior to optic nerve infarction, hyperemic swelling of the nerve and/or cotton wool spots in the macular area may be the only ophthalmologic finding (Fig. 18–3). Following resolution of the optic nerve swelling the optic nerve is usually diffusely pale and atrophic with a clinically absent nerve fiber layer and severe vascular attenuation (Fig. 18–4). FIGURE 18–1 A: Fundus photograph of posterior pole of right eye with only age-related vascular narrowing. B: In contrast, arteritic anterior ischemic optic neuropathy (AION) of the fellow eye secondary to giant cell arteritis (GCA) (left eye); there is pallid swelling with associated hemorrhage and severe vascular narrowing of the involved eye. FIGURE 18–2 Cilioretinal artery occlusion (right eye) secondary to giant cell arteritis.1 (Courtesy of Prof. F. Ghanchi, M.D., Glasgow.) • Choroidal ischemia or cilioretinal artery occlusion may accompany or occur in isolation of the optic neuropathy. • Choroidal ischemia may be confirmed by fluorescein angiography (delayed, incomplete choroidal filling). This is noted only in the first few seconds of the angiogram. (Fig. 18–5). Temporal artery or scalp vessel tenderness is common, with nodularity and decreased pulse, whereas scalp necrosis is a rare occurrence. Extraocular muscle dysfunction due to ischemic myopathy or cranial nerve palsy may be present. The following features should raise the question of alternate diagnoses: FIGURE 18–3 Cotton wool retinal infarct (arrow), in a visually asymptomatic patient with giant cell arteritis.
ARTERITIC ANTERIOR ISCHEMIC OPTIC NEUROPATHY
URGENCY OF EVALUATION
DIAGNOSIS
SYMPTOMS
Demographics
Visual Loss
Pain
Systemic Symptoms of Temporal Arteritis
SIGNS
Visual Acuity
Visual Field
Pupils
Optic Disc
Other Abnormalities (Table 18–1)
Red Flags
 Age below 60, simple altitudinal visual field loss, visual acuity >20/200, lack of headache or other systemic symptoms (suggests nonarteritic AION)
Age below 60, simple altitudinal visual field loss, visual acuity >20/200, lack of headache or other systemic symptoms (suggests nonarteritic AION)
 Severe bilateral hyperemic optic disc edema, nausea, and vomiting (suggest elevated intracranial pressure from a mass)
Severe bilateral hyperemic optic disc edema, nausea, and vomiting (suggest elevated intracranial pressure from a mass)
 Severe optic neuropathy with mild optic disc edema and multiple nonlocalizing cranial neuropathies (suggests meningeal carcinomatosis)
Severe optic neuropathy with mild optic disc edema and multiple nonlocalizing cranial neuropathies (suggests meningeal carcinomatosis)
 Presence of embolic disease, for example, Hollenhorst plaques within the retinal circulation (suggests a carotid or cardiac source of embolic vascular occlusive disease).
Presence of embolic disease, for example, Hollenhorst plaques within the retinal circulation (suggests a carotid or cardiac source of embolic vascular occlusive disease).
DIFFERENTIAL DIAGNOSIS
Nonarteritic Anterior Ischemic Optic Neuropathy (Chapter 19)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


