12 This chapter will review several anterior segment vitrectomy procedures that use anterior and posterior segment instrumentation, including management of (1) vitreous loss at cataract surgery, (2) late complications of vitreous in the anterior chamber, (3) inadequate pupillary space, (4) lens surgery, (5) hyphema, and (6) epithelium in the anterior chamber.
Anterior Segment Vitrectomy Procedures
Indications
General Principles
 Incision site: Limbus versus pars plana.
Incision site: Limbus versus pars plana.
 Choose limbal approach if mechanical objectives or problems are anterior to the pars plana; this approach has less risk of retinal damage (because of vitreous incarceration in the pars plana sclerotomy site, with secondary vitreoretinal traction and retinal tear formation).
Choose limbal approach if mechanical objectives or problems are anterior to the pars plana; this approach has less risk of retinal damage (because of vitreous incarceration in the pars plana sclerotomy site, with secondary vitreoretinal traction and retinal tear formation).
 A pars plana approach offers better access to retroiridal space (e.g., for lysis of iridovitreal adhesions), use of intraocular illumination, and access to the posterior two thirds of the vitreous cavity.
A pars plana approach offers better access to retroiridal space (e.g., for lysis of iridovitreal adhesions), use of intraocular illumination, and access to the posterior two thirds of the vitreous cavity.
 Tissue engagement in the vitrectomy probe. Stiff tissue is best incarcerated and cut with the vitrectomy machine set to low cutting rate (e.g., 100–300 cpm) and high vacuum (e.g., 200–300 mm Hg), as these settings enable greater molding of the tissue to the cutting port (Table 12.1). If vacuum is high, infusion pressure must be increased to prevent globe collapse.
Tissue engagement in the vitrectomy probe. Stiff tissue is best incarcerated and cut with the vitrectomy machine set to low cutting rate (e.g., 100–300 cpm) and high vacuum (e.g., 200–300 mm Hg), as these settings enable greater molding of the tissue to the cutting port (Table 12.1). If vacuum is high, infusion pressure must be increased to prevent globe collapse.
| Tissue Engagement | Stiff | Soft |
|---|---|---|
| Port Size | Large | Small |
| Cutting Rate | Slow | Fast |
| Infusion Pressure | High | Low |
| Vacuum | High | Low |
 Cutting mechanism: Guillotine versus rotary cutting. New rotary cutters offer highly efficient vitreous removal. Guillotine cutters may provide more effective cutting of stiff tissue without inducing traction on the tissue.
Cutting mechanism: Guillotine versus rotary cutting. New rotary cutters offer highly efficient vitreous removal. Guillotine cutters may provide more effective cutting of stiff tissue without inducing traction on the tissue.
 Techniques for cutting stiff tissue:
Techniques for cutting stiff tissue:
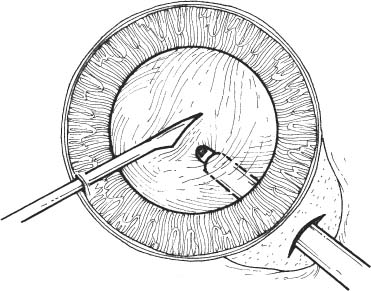
Figure 12.1
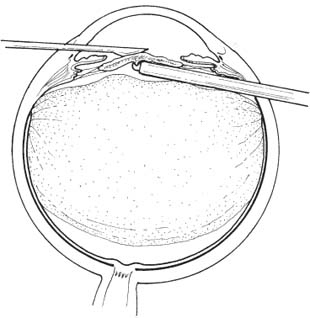
Figure 12.2
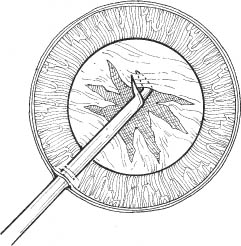
Figure 12.3
 Chopping block (Figs. 12.1 and 12.2).
Chopping block (Figs. 12.1 and 12.2).
 Intraocular scissors (Fig. 12.3).
Intraocular scissors (Fig. 12.3).
 Diathermy.
Diathermy.
 Management of bleeding
Management of bleeding
 Increase intraocular pressure by increasing the infusion pressure, as vitrectomy incisions are watertight (a hydraulically closed system).
Increase intraocular pressure by increasing the infusion pressure, as vitrectomy incisions are watertight (a hydraulically closed system).
 Diathermy.
Diathermy.
 Vitrectomy via limbal incisions (e.g., management of vitreous loss at cataract surgery).
Vitrectomy via limbal incisions (e.g., management of vitreous loss at cataract surgery).
 Excise enough vitreous to prevent vitreous prolapse into the anterior chamber (anterior to the plane of the iris diaphragm).
Excise enough vitreous to prevent vitreous prolapse into the anterior chamber (anterior to the plane of the iris diaphragm).
 Excise vitreous along pupillary-axis: direct probe into center of pupillary space.
Excise vitreous along pupillary-axis: direct probe into center of pupillary space.
 Work in anterior one third vitreous cavity: place probe just posterior to iris diaphragm with cutting port in clear view at all times. (Operating microscope does not permit focus on probe tip if it is advanced deeper than anterior ~1/3 of vitreous cavity unless special lenses are used.)
Work in anterior one third vitreous cavity: place probe just posterior to iris diaphragm with cutting port in clear view at all times. (Operating microscope does not permit focus on probe tip if it is advanced deeper than anterior ~1/3 of vitreous cavity unless special lenses are used.)
 Infusion: Sleeve versus second instrument.
Infusion: Sleeve versus second instrument.
 Infusion sleeve offers simultaneous fluid infusion and vitreous removal through a single incision. However, the incision is somewhat large (to accommodate the sleeve), and the infusion is directed at the probe tip, which may impair efficient incarceration of vitreous into the probe.
Infusion sleeve offers simultaneous fluid infusion and vitreous removal through a single incision. However, the incision is somewhat large (to accommodate the sleeve), and the infusion is directed at the probe tip, which may impair efficient incarceration of vitreous into the probe.
 Second instrument offers bimanual capabilities (e.g., displacement of iris peripherally to visualize residual peripheral lens cortex) but requires a second entry site. Usually this limbal site has already been created during the cataract surgery.
Second instrument offers bimanual capabilities (e.g., displacement of iris peripherally to visualize residual peripheral lens cortex) but requires a second entry site. Usually this limbal site has already been created during the cataract surgery.
 Illumination: fiber optic probe versus coaxial illumination of the operating microscope.
Illumination: fiber optic probe versus coaxial illumination of the operating microscope.
 Fiber optic probe can be used externally (probe placement at limbus with visualization by scleral scatter) or internally (through a separate incision). Fiber optic probe probably offers better visualization of vitreous strands in the anterior chamber and better visualization of the anterior vitreous cavity than coaxial illumination of the scope.
Fiber optic probe can be used externally (probe placement at limbus with visualization by scleral scatter) or internally (through a separate incision). Fiber optic probe probably offers better visualization of vitreous strands in the anterior chamber and better visualization of the anterior vitreous cavity than coaxial illumination of the scope.
 Coaxial illumination of the operating microscope avoids need for second instrument in the eye but offers more limited view of vitreous cavity and vitreous prolapse into the anterior chamber.
Coaxial illumination of the operating microscope avoids need for second instrument in the eye but offers more limited view of vitreous cavity and vitreous prolapse into the anterior chamber.
 Instrument removal: Steps to avoid vitreous prolapse into anterior chamber and limbal incision.
Instrument removal: Steps to avoid vitreous prolapse into anterior chamber and limbal incision.
 Lower intraocular pressure.
Lower intraocular pressure.
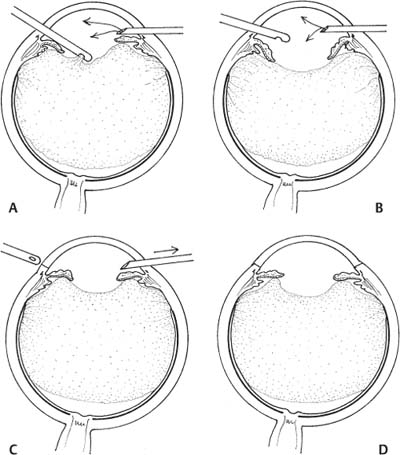
Figure 12.4
 Some surgeons infuse air to prevent vitreous incarceration in wounds (Figs. 12.4A,B).
Some surgeons infuse air to prevent vitreous incarceration in wounds (Figs. 12.4A,B).
 Withdraw instruments (Figs. 12.4C,D).
Withdraw instruments (Figs. 12.4C,D).
 If air has been infused, replace air with balanced salt solution.
If air has been infused, replace air with balanced salt solution.
Preoperative Procedure
See Chapter 3.
Pupil management: For procedures requiring good visualization behind the iris (e.g., excision of retained peripheral lens cortex) dilate the pupil preoperatively (e.g., Cyclogyl 1% plus phenylephrine 2.5% every 15 minutes × 3, starting 1 hour before surgery) or use flexible iris retractors intraoperatively. In other cases (e.g., anterior vitrectomy preceding placement of a secondary intraocular lens [IOL]), dilation may be unnecessary.
Instrumentation
 Lid speculum
Lid speculum
 Vitrectomy suction/cutting instrumentation. In this chapter, the Alcon Accurus vitrectomy machine (Alcon, Inc., Fort Worth, TX, US) is used for illustrative purposes. The authors recognize that other excellent machines are available and have no financial interest in the Accurus system.
Vitrectomy suction/cutting instrumentation. In this chapter, the Alcon Accurus vitrectomy machine (Alcon, Inc., Fort Worth, TX, US) is used for illustrative purposes. The authors recognize that other excellent machines are available and have no financial interest in the Accurus system.
 Sutures (10–0 nylon, 7–0, 8–0 Vicryl, 6–0 plain gut)
Sutures (10–0 nylon, 7–0, 8–0 Vicryl, 6–0 plain gut)
 Fine-toothed tissue forceps (e.g., 0.12 mm straight Castroviejo or Colibri)
Fine-toothed tissue forceps (e.g., 0.12 mm straight Castroviejo or Colibri)
 Needle holder
Needle holder
 Lens loop
Lens loop
 23 gauge butterfly infusion needle or cannula
23 gauge butterfly infusion needle or cannula
 Acetylcholine solution (e.g., Miochol)
Acetylcholine solution (e.g., Miochol)
 Cyclodialysis spatula or vitreous sweep
Cyclodialysis spatula or vitreous sweep
 Tuberculin syringe with 30 gauge cannula
Tuberculin syringe with 30 gauge cannula
 Cellulose sponges
Cellulose sponges
 Jeweler’s forceps
Jeweler’s forceps
 Vannas scissors
Vannas scissors
 Westcott scissors
Westcott scissors
 Cautery (underwater eraser or disposable)
Cautery (underwater eraser or disposable)
 Microsurgical knife (e.g., Beaver #75M blade)
Microsurgical knife (e.g., Beaver #75M blade)
 20-gauge microvitreoretinal (MVR) blade
20-gauge microvitreoretinal (MVR) blade
 Gills-Vannas or 20 gauge vitreous scissors
Gills-Vannas or 20 gauge vitreous scissors
 20 gauge intraocular forceps
20 gauge intraocular forceps
Operative Procedure
Managing Vitreous Loss at Cataract Surgery
At the time of posterior capsule or zonular rupture, the extent of capsular damage and the presence or absence of vitreous loss must be assessed. In select cases demonstrating adequate capsular support, a posterior chamber intraocular lens (PCIOL) can be fixated in the ciliary sulcus. Removal of prolapsed vitreous with automated instruments permits complete vitreous excision from the anterior chamber while minimizing vitreoretinal traction, compared with vitreous removal from the anterior chamber using cellulose sponges and scissors to directly cut the vitreous strands. Following is a description of the management of an eye with significant operative capsular disruption and vitreous loss.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


