Anterior Capsule Management
M. Edward Wilson
Rupal H. Trivedi
Anterior capsulotomy, specifically a continuous curvilinear capsulorhexis (CCC), is notoriously difficult in infants and young children because of the extreme elasticity of the anterior capsule, positive vitreous pressure, and at times, poor dilatation of the pupil.1,2 The availability of better operating microscopes and microsurgical instruments combined with higher-viscosity ophthalmic viscosurgical devices (OVDs) is helpful, but the creation of an intact capsulorhexis in infants remains a challenge. Unique characteristics of the anterior capsule in children have created the need for variations in techniques used for anterior capsulotomy in adult eyes. A surgeon who applies adult anterior capsule maneuvers to the pediatric anterior capsule may be surprised and disappointed at the outcomes. This is especially true in infant eyes. This unpredictability has led researchers and surgeons to use alternative methods to open the anterior capsule in children.3,4,5,6,7,8,9,10,11 The desired end result of any alternative is the consistent achievement of a continuous curvilinear anterior capsulotomy of a desired size and shape, centered on the visual axis. In addition, the capsule opening should be smooth and strong with no tags, tears, or right-angled edges. Prior to the late 1980s, the strength and size of the capsulotomy was of little concern in pediatric eyes. In fact, when the vitrector was introduced as an instrument to remove pediatric cataracts, the entire lens capsule was often removed—even the capsular equator—to assure that secondary closure of the capsulotomy did not occur.
The current widespread acceptance of intraocular lens (IOL) implantation in the pediatric eye has created the need for an opening in the anterior capsule that can be made to a specific size and shape and with an edge that can withstand the stress of implantation maneuvers. An intact anterior capsulotomy supports all the subsequent steps of lens aspiration and IOL implantation. Anterior capsulotomy techniques have evolved in pediatric cataract surgery. Adult techniques have been modified, and some uniquely pediatric techniques have been developed. For surgeons experienced in adult procedures, the pediatric anterior capsulotomy is often mentioned as the operative step requiring the most adjustment from the adult routine. Wilson detailed the evolution of pediatric capsulotomy and compared various capsulotomy options (using clinical, cadaveric, and porcine data and including scanning electron microscopy [SEM]) in a thesis submitted as partial requirement for membership in the American Ophthalmological Society.2
CHARACTERISTICS OF THE PEDIATRIC ANTERIOR CAPSULE
The anterior capsule is thinnest at birth, increasing in thickness with age until approximately age 75 years.12 Seland13 described the neonatal anterior lens capsule as uniform and approximately 4 mm in thickness. By old age, the capsule had increased to 20 to 25 mm centrally and 30 mm near the lens equator.13 Krag et al.12 analyzed 67 human eyes from age 7 months to 98 years and found that anterior capsule thickness increased from 11 to 33 mm. The association of thickness with age fit a straight line from birth to age 75 years, after which it changed slope and thinned slightly.12 In conjunction with these anatomic changes, the anterior capsule’s biomechanical properties are also altered with age.
The young anterior lens capsule is strong and very elastic. The elderly anterior lens capsule is, by comparison, weak and inelastic. Krag et al.12 found that anterior lens capsule extensibility was maximal in infancy and decreased about 0.5% per year throughout life (measured range, 108% to 40%). Aging of the human anterior lens capsule leads to a progressive loss of mechanical strength. Overall tensile strength decreases by a factor of five during the life span, and the extensibility decreases by at least a factor of two. In surgery, the young capsule is highly elastic and difficult to puncture. Much more force is required before tearing begins. In contrast, the capsule of the elderly is much less extensible, easier to open, and tears with much less force. These differences between the adult and child must be understood and accounted for when planning for surgery on the pediatric lens.
ANTERIOR CAPSULOTOMY TECHNIQUES
The first anterior capsulotomy technique associated with an IOL implantation, performed by Sir Harold Ridley in the 1950s, was an uncontrolled tear using forceps without the aid of microscope magnification.14 It served only as a means to gain access to the lens contents. Complete removal of the anterior capsule was desired. If remnants or tags were seen after nucleus expression, they were torn with smooth-bladed capsule forceps. This maneuver at times resulted in the entire posterior capsule’s also being delivered from the eye, effecting an unplanned intracapsular surgery.
Can-Opener Capsulotomy
To reduce stress placed on the zonular fibers and produce a more rounded capsulotomy with fewer tags, the multipuncture or can-opener capsulotomy came into common use. A capsulotomy was made by punching a 27-gauge bent-needle cystitome repeatedly through the anterior capsule in a postage stamp or can-opener fashion and connecting the punches to form a circular opening. A jagged but circular opening in the capsule was formed. Frequently, however, radial extensions of the capsulotomy occurred during lens removal or IOL insertion. These tears resulted in uncertainty regarding the stability of the capsular bag and the position of the IOL after implantation. The can-opener technique puts more stress on the zonular fibers and is more likely to leave capsule tags or strands that can interfere with lens aspiration. Pediatric surgeons seldom use the can-opener capsulotomy method, but when needed, it is safer and more effective in children than in adults. The elastic nature of the pediatric capsule causes each can-opener puncture to convert to a small arc tear similar to a mini manual CCC.
Manual CCC
The technique known today as manual CCC was developed simultaneously in North America by Gimbel and in Europe by Neuhann.15 The CCC method clearly creates the “gold standard” capsulotomy edge. While a manual CCC is ideal for adults, it is more difficult to perform in infantile eyes with cataracts. However, it is still the gold standard since it resists tearing once completed successfully. Because of the increased elasticity of the pediatric anterior capsule, more force is required when pulling on the capsular flap before tearing begins. Control of the capsulectomy and prevention of extensions out toward the lens equator are inversely related to the force needed to generate the tear. As a result, inadvertent extensions out to the lens equator (known as the “runaway” rhexis) are common in children. In addition, reduced scleral rigidity in children produces what has been called posterior vitreous “pressure” when the eye is entered. The vitreous in children is formed and less liquefied. Scleral collapse causes an “upthrust” from the formed vitreous that pushes the lens anteriorly and keeps the anterior capsule domed, convex, and taut. This results in the tendency for the capsulorhexis to spiral outward.
When performing a manual CCC capsulotomy in children, the following caveats are offered2:
Use a high molecular weight OVD to flatten the anterior capsule and deepen the anterior chamber. This will create laxity in the anterior capsule and combat the effects of low scleral rigidity.
Aim for a slightly smaller-than-desired capsulotomy. With the stretch in the anterior capsule, the opening is usually larger at completion than it appears to be during the active tearing.
When creating the manual CCC capsulotomy, frequently release the capsular flap and inspect the size, shape, and direction of the tear. Regrasp near the site of the continuous tear and readjust the direction of pull if needed to keep the capsulotomy on the planned course. Pulling the leading edge along the path of the tear is called “shearing,” and this is the predominant force used in adult capsulotomy. In children, more pull is often needed toward the center of the pupil (90 degrees to the path of the tear) to avoid an extension of the manual CCC out toward the lens equator. This is referred to as “tearing.”
Additional OVD should be added as needed to keep the capsule lax during the tearing. Use of capsular dye can be beneficial (Fig. 17.1). To rescue a manual CCC that begins to extend peripherally, regrasp near the leading edge of the capsulotomy and redirect the capsular tear by pulling back in the direction from which the tear was originating (so-called “pull-back” technique). Rarely, the
vitrector or the Kloti radiofrequency diathermy device is used to rescue the errant capsular tear and round out the capsulorhexis.
vitrector or the Kloti radiofrequency diathermy device is used to rescue the errant capsular tear and round out the capsulorhexis.
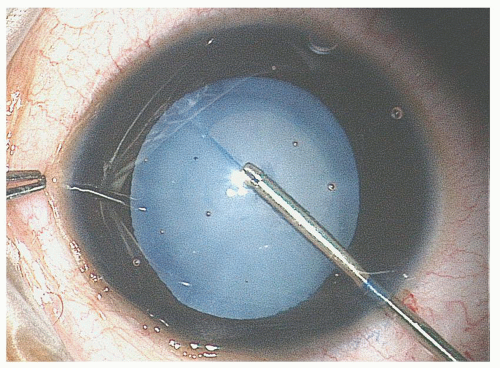 Figure 17.1. Manual CCC using trypan blue in a 2-year-old child with total cataract. |
Some surgeons have altered the adult technique even more substantially in order to facilitate CCC in elastic capsules. Auffarth et al.4 developed a modified CCC technique for use in experiments on eyes of young albino rabbits and suggested that it be used for young human capsules as well. The technique begins with a puncture of the lens capsule at the superior border of the intended capsulotomy using a 27-gauge needle. Capsulorhexis forceps are then used to grasp the anterior capsule centrally. The capsular flap is torn toward the 6 o’clock position until a half-circle is completed. The force is then reversed toward 12 o’clock position, pulling with equal force to both tearing edges. The authors reported a radial tear in only 2 of the 32 rabbit eyes.
Nischal8 described a modification of the Auffarth technique in which two stab incisions are made in the anterior capsule, outlining the desired diameter of the capsulorhexis (two-incision push-pull, or TIPP). Capsulorhexis forceps are used to grasp one end of the distal edge of the proximal anterior capsule stab incision. The grasped edge is gently pushed toward the corresponding point of the distal stab incision until the edge reaches halfway to the distal stab. The corresponding end of the proximal edge of the distal stab incision is similarly grasped but with the capsule pulled gently toward the proximal stab incision. The two tears meet to form the CCC. This is repeated for the other end of each stab incision to complete the entire CCC. The tearing force, using this technique, is always directed toward the center of the pupil.16
Vitrectorhexis
Mechanical suction and cutting instruments began to be utilized for pediatric cataract surgery in the late 1970s and early 1980s. Parks17 and Taylor18 were among the first to advocate for the performance of a primary mechanized posterior capsulectomy and anterior vitrectomy during pediatric cataract surgery. Taylor also described removal of the anterior capsule mechanically.18 A mechanized (vitrector-cut) anterior capsulotomy technique combined with IOL insertion in children was first described, studied, and popularized by Wilson et al. in the mid-1990s.3,19 It rapidly replaced the can-opener and even the manual CCC for infants and toddlers having cataract surgery, whether or not an IOL was implanted primarily.
The commonly used term “vitrectorhexis” emphasizes the fact that it is a substitute for capsulorhexis performed using the vitrector. It is, in reality, a misnomer, because “rhexis” means to tear rather than to cut. The original name, “mechanized anterior capsulectomy,” emphasized the mechanized nature of the vitrector handpiece and the fact that a portion of the capsule was removed (capsulectomy) rather than merely opened (capsulotomy).3,19
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


