Anesthesia for the Pediatric Ophthalmology Patient
Susan K. Woelfel
Barbara W. Brandom
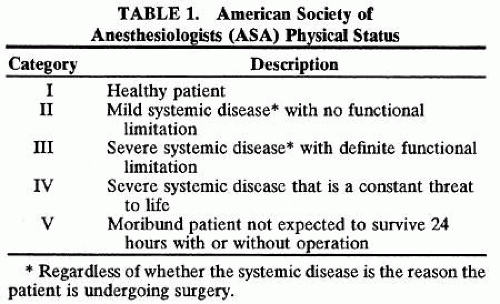
Unlike adult ophthalmic procedures, most procedures in children are performed using general anesthesia. Because most such procedures are elective, the patient should be in an optimal state of health at the time of surgery. Clear communication among the surgeon, patient and patient’s family, and anesthesiologist is essential. Parents of children with any medical problems are encouraged to talk to an anesthesiologist before the day of surgery. A review article1 documented perioperative morbidity rates and mortality in pediatric patients during a 6-year study period that involved 29,220 uses of anesthesia. Two findings of this review are particularly noteworthy. First, infants younger than 1 month of age have the greatest risk of perioperative adverse events, the most significant of which is cardiovascular or respiratory depression. Cardiac arrest occurred nine times as often in this age group compared with children over 1 year of age. Events such as hypotension, laryngospasm, or apnea occurred intraoperatively, in the recovery room, and within the first 72 hours postoperatively. Most of these infants were American Society of Anesthesiologist (ASA) physical status (PS) III–V (Table 1) having major abdominal surgery. Second, the study found little difference in the incidence of intraoperative complications between the pediatric group older than 1 month of age and adults (9 versus 10.6, respectively, per 10,000 cases) with the exception that children do experience twice as many adverse events in the recovery room (13 for children versus 5.9 for adults per 10,000 cases); airway obstruction is the most frequent event. Another frequent postoperative problem is the combination of nausea and vomiting (30% in children versus 5% in adults). Possible explanations for this last finding include less use of retrobulbar blocks in younger patients, undertreatment of pain in children, or type of surgical procedure. For example, after repair of strabismus, incidence of postoperative nausea and vomiting may be as high as 80%.
 |
A more recent collection of cardiac arrest data reveals that anesthesia is a major cause of cardiac arrest in ASA PS III–IV patients who have a cardiac arrest in the operating room. In addition, outcome is much better in healthy PS I–II patients, with 6% mortality compared with 55% mortality in PS III–IV patients when a cardiac arrest does occur.2 The anesthetic problems in this review were attributed to drug administration, including relative anesthetic overdose, wrong drug or dose, and allergic reaction.
Additional reviews3,4 found that the incidence of cardiac arrest in children less than 1 year of age was 0 (zero) when a trained pediatric anesthesiologist was present versus 19.7 per 10,000 anesthetics when a nonpediatric anesthesiologist was supervising. Similarly, incidence of bradycardia was half as likely in the presence of a trained pediatric anesthesiologist.
The goal of this chapter is to review the measures taken to provide safe anesthesia and recovery for a child undergoing ocular surgery. The details of anesthetic management are influenced by the individual patient and type of surgery. On any given day, the variety of ocular surgeries performed may include a healthy 5-year-old who has been treated with echothiophate iodide and is undergoing an extraocular muscle resection of 10 minutes’ duration, a 6-week-old (born prematurely at 28 weeks’ gestation) undergoing scleral buckling of 2 hours duration, and a frightened 3-year-old with a penetrating eye injury. The factors common to all these patients include the need for preoperative evaluation, including preoperative fasting, airway management with specialized endotracheal tubes or a laryngeal mask airway (LMA), intraoperative monitoring, administration of analgesics and antiemetics, andintraoperative and postoperative administrationof intravenous fluid, the potential occurrence of oculocardiac reflex (OCR), postoperative croup, pain, nausea, and vomiting; and the determination of discharge criteria.
PREOPERATIVE EVALUATION ASA CLASSIFICATION
All patients must be evaluated by an anesthesiologist before surgery. This is often done on the day of surgery for healthy children. The physical status (PS I to V) is a method to evaluate and communicate the condition of the child (see Table 1). If the child has systemic disease, the primary care physician should perform a preoperative evaluation to determine whether the child’s disease has been optimally treated. A letter reviewing the child’s medical problems and treatment is a useful source of information for the anesthesiologist preoperatively.
INFECTIOUS DISEASES
Upper Respiratory Tract Infection Versus Allergic Rhinitis
Young children, especially those in day care or school settings, experience frequent upper respiratory tract infections. The child with a runny nose (clear rhinorrhea) and no other symptoms of illness may have allergic rhinitis or vasomotor rhinitis rather than viral infection. If the clinical state of a child with allergic rhinitis is stable, then that child is a candidate for elective surgery. Clear rhinorrhea can complicate general anesthesia by increasing the likelihood of laryngospasm and oxygen desaturation resulting from secretions in the pharynx and larynx. If an antihistamine is being given preoperatively to a child with allergic rhinitis, this medication should be continued up until surgery because it may decrease the likelihood of airway problems intraoperatively. Conversely, if symptoms of bacterial infection such as lethargy, high fever (temperature over 39°C), decreased appetite, purulent drainage, and productive cough are present, there is an unacceptable risk because of the possibility of progression to serious diseases such as pneumonia or sepsis. A child with an upper respiratory tract infection may transmit the infection to health care workers and other patients. With such potential complications, elective surgery should be rescheduled for a time when the symptoms have resolved (about 2 to 4 weeks). The child may be evaluated by the attending pediatrician to ensure that the problem has resolved satisfactorily.
Other Infectious Diseases
Preoperative evaluation of all potentially infectious conditions is especially important in children. The child with fever, vomiting, or diarrhea who is scheduled for an elective procedure should have the surgery rescheduled when symptoms have resolved. These symptoms may be exacerbated by anesthesia and this may complicate intraoperative and postoperative management. For example, a rapid increase in temperature may suggest the presence of malignant hyperthermia, and vomiting may increase the risk of aspiration during the procedure and produce significant postoperative pulmonary complications.
A child with chickenpox is infectious for several days before the appearance of the pustules until scabs form over the skin lesions. The expected time from exposure to development of this disease is 11 to 21 days. Those children who are capable of transmitting the disease to other patients should not come to the hospital, and their surgery should be delayed for 21 days. If a child has any other acute infectious disease, elective ocular surgery should be postponed until that disease is resolved.
Another example of a common disease process in infants and children is otitis media. Acute otitis media should be resolved as determined by a pediatrician before elective ocular surgery. A child on prophylactic medication for chronic otitis media is a candidate for elective surgery.
PEDIATRIC DISEASES AND CONDITIONS
Asthma
Asthma is a common pediatric disease that requires careful documentation of the preoperative status. The goal is to have the patient in optimal condition preoperatively, to have a deep plane of anesthesia, and to avoid any stimulus that may precipitate bronchospasm. An LMA may be used instead of an endotracheal tube because it provides a less noxious stimulus. Halothane and sevoflurane are often used because they promote bronchodilatation. If the asthmatic child is taking oral steroids, a steroid boost is not necessarily required preoperatively for a brief ocular procedure. However, the anesthesiologist must be aware of the possible need for supplemental doses of steroid intraoperatively or post-operatively. In addition, inhaled bronchodilators should be available in the operating room.
Diabetes Mellitus
Diabetes mellitus is a serious illness in pediatric patients that requires careful planning to avoid perioperative complications. The unstable juvenile diabetic patient may be admitted to the hospital the night before an operation to receive intravenous maintenance fluids containing glucose and insulin to prevent dehydration and to allow blood glucose to be monitored. The stable diabetic patient may be admitted the morning of surgery. The preoperative dose of insulin should be less than the usual morning’s dose, and surgery should be scheduled early in the day, as the first procedure whenever possible. When insulin is given, glucose-containing solutions should be administered at maintenance rates and blood glucose levels should be monitored with a glucometer intraoperatively and postoperatively. After minor procedures and as soon as well-controlled patients are able to take fluid by mouth postoperatively, they may be discharged home if a responsible adult is present. Patients with brittle diabetes should be monitored for a longer period before discharge; sometimes it is necessary to keep them overnight.
Prematurity
Children born prematurely often have complex medical problems and significant disease that involves several systems. The premature infant with periodic breathing is at increased risk for apneic and bradycardic episodes in the perioperative period.5 Postoperative instability of the ventilatory drive and pulmonary complications, such as atelectasis or bronchospasm, are common in patients with residual bronchopulmonary dysplasia. A pediatrician should thoroughly evaluate these children and document their baseline pulmonary status. A notation such as “OK for anesthesia” is not useful, whereas specific suggestions for management such as “this child requires 2 L oxygen by nasal cannula at home; the chest x-ray shows no new changes; lungs on auscultation reveal coarse bilateral breath sounds that clear after treatment with inhaled bronchodilators” are useful. With a statement such as this, an established baseline status and recommended therapeutic management are clarified, and a reasonable plan for the management of potential complications is identified. See the later section on Inpatient Versus Outpatient for postoperative care of these children. These infants may not tolerate IV fluid replacement over 2 to 3 hours as term infants will be able to do, because it may increase the work of breathing. They may have poor IV access as well. A baseline oxygen saturation should be measured before induction of anesthesia. Bronchodilators should be available. Normal temperature should be maintained.
Down Syndrome
Ophthalmic problems and several systemic illnesses or malformations are commonly associated with trisomy 21 or Down syndrome. Children with Down syndrome have mental retardation ranging from severe to very mild and also have a high incidence (20%) of atlantoaxial instability. Neurologic and radiologic evaluations should be performed on any patient with symptoms of sensory or motor dysfunction in the limbs or with neck pain. If a child has an unstable neck, then extension of the neck (i.e., as is usual for intubation) may injure the spinal cord. In addition, extra care should be taken in positioning this child’s head and neck while the muscles are relaxed under anesthesia.
Children with Down syndrome also have macroglossia and subglottic stenosis (25% of patients), which frequently complicates airway management. The use of an oral airway or the jaw thrust maneuver may prevent airway obstruction on induction of anesthesia. For the same reason, such a child ordinarily should be extubated when fully awake and muscle function of the airway has returned to normal.
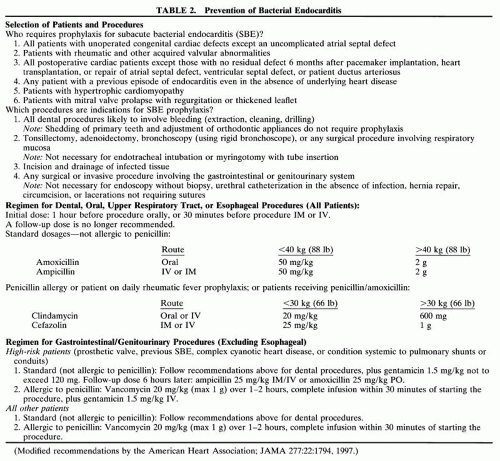
These patients usually require atropine on induction if halothane is administered. Patients with Down syndrome also have a high incidence (50%)of associated cardiovascular disease, with a ventricular septal defect or an atrioventricular canal the most common malformations. If a murmur is present, a full evaluation by the pediatric cardiologist is indicated using available electrocardiographic, radiographic, echocardiographic, and cardiac catheterization data. The most recent (1997) recommendations for subacute bacterial endocarditis (SBE) prophylaxis are presented in Table 2.
 |
Congenital Heart Disease
Any child with congenital heart disease should be evaluated by a cardiologist so that the cardiovascular state is optimized and medication levels are therapeutic. Cardiovascular shunts (i.e., Blalock-Taussig shunts) should be evaluated for proper functioning. Baseline pulse oximetric values should be available. Cyanotic children should not be polycythemic, and the hematocrit value should be decreased to less than 60% before elective surgery. The cardiologist should note whether SBE prophylaxis is warranted and if so which antibiotics are most appropriate. Most ophthalmic operations do not produce bacteremia. SBE prophylaxis is not required for endotracheal intubation alone or forprobe and irrigation of the nasolacrimal duct. WhenSBE prophylaxis is required, ampicillin 50 mg/kgmay be administered intravenously after induction of anesthesia instead of administering oral drug preoperatively. (See Table 2 for the current guidelines.)
Sickle Cell Anemia
Sickle cell anemia occurs in black and Mediterranean populations. Preoperative evaluation of the hemoglobin (Hgb) S level and transfusion of blood to reduce the Hgb S level to less than 40% has been recommended in the past. More recently, data show that if Hgb is 10, no adverse effects are likely during minor surgical procedures provided all other factors are treated (i.e., avoid hypothermia, dehydration, hypoxia, acidosis). Thus, children with sickle cell anemia require oxygen in the recovery room until fully awake. Outpatient surgery is acceptable for minor procedures, but any surgery or drugs that depress respiration could precipitate a sickling crisis. The narcotic requirement may be greater than expected because tolerance may develop during treatment of the painful crises characteristic of this disease. These data may be obtained during the preoperative evaluation.
Congenital Syndromes and Craniofacial Abnormalities
Some congenital syndromes have systemic as well as ocular manifestations. For example, patients with Kearns-Sayre syndrome have heart block, and those with Wagner-Stickler syndrome have mitral valve prolapse and micrognathia.
A list of congenital syndromes with a description of the disease state and anesthetic implications is given in the appendix of Anesthesia for Infants and Children, edited by Motoyama and Davis.6
Patients with craniofacial syndromes may pre-sent for surgical treatment of strabismus or eyelidabnormalities. Some of these syndromes, espe-cially Treacher Collins, Apert, and Goldenhar syndromes, also involve abnormal airway anatomy that makes tracheal intubation difficult or impossible. Appropriate preoperative evaluation of the child’s airway by the anesthesiologist and discussion of airway management (i.e., of the possible need for a tracheostomy or postoperative care in the inten-sive care unit) with the family should occur beforethe day of surgery. Appropriate caregivers (e.g., the pediatric laryngologist) and equipment (e.g., fiberoptic bronchoscope, Bullard laryngoscope, light-wand, intubating LMA) should be available at thetime of surgery. It is more common to see children with a cleft lip or palate who present for eye surgery. They usually have no special preoperative needs, except if they have had prior surgery, they may strongly dislike the mask induction, either an intravenous induction or preoperative medication to decrease anxiety is recommended.
Common Neurologic Diseases
Cerebral palsy is a static neurologic condition that occurs in 2 to 4 of 10,000 live births. The most common etiologic factor is prematurity. Cerebral palsy patients often include those who cannot communicate, cannot move or straighten their limbs, and those who have frequent seizures and gastroesophageal reflux. Preoperatively, seizures should be controlled and appropriate medication (ranitid-ine hydrochloride, metoclopramide hydrochloride, or cisapride) given for gastroesophageal reflux. On induction, these children may be at risk for aspiration. Seizure medication should be resumed as soon as possible postoperatively. Care should be taken to comfortably support the patient’s arms and legs intraoperatively. All prophylactic antibiotics (e.g., against urinary infection) should be continued during the perioperative period.
INPATIENT VERSUS OUTPATIENT
It is very unusual for patients to be admitted the day before surgery. An exception might be a child with brittle diabetes mellitus. Most children go home after the procedure the same day unless their underlying disease requires monitoring or if there have been significant anesthetic complications such as post obstructive pulmonary edema.
Any infant younger than 44 weeks’ postconceptional age or one who has a history of apnea and bradycardia should be admitted postoperatively for at least 12 hours of respiratory monitoring.6 Caffeine is sometimes used to treat expremature infants with postoperative apnea. Full-term infants should be at least 1 month of age before elective surgery. Infants and children should have their elective surgery scheduled early in the day so their fasting time is not prolonged by delays in the operating schedule. Arbitrary limits on the minimum age to be accommodated at an ambulatory center may be imposed because of limited staff experience or training, or a lack of availability of equipment or consultants for small infants. Patients who are likely to have complications due to preexisting medical conditions such as diabetes, latex allergy, or malignant hyperthermia susceptibility should have surgery scheduled where these problems are most easily managed. This may mean surgery occurs in a hospital rather than an ambulatory center.
PREOPERATIVE PREPARATION LABORATORY STUDIES
The need for preoperative laboratory evaluation, if any, should be determined on an individual basis. Most pediatric anesthesiologists do not require healthy infants or children to undergo any routine laboratory studies.7 If the child has a systemic illness (e.g., diabetes mellitus) or if the procedure has the potential for a large amount of blood loss (e.g., excision of a vascular tumor), then appropriate preoperative laboratory studies (blood glucose, Hgb, or hematocrit and a type and cross for blood) should be obtained. Children taking anticonvulsants should be observed during follow-up by their pediatrician or neurologist and have therapeutic blood levels.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


