Introduction
Rhinosinusitis is widely believed to comprise of a spectrum of inflammatory and infectious diseases concurrently affecting the mucous membranes of the nose and paranasal sinuses (PNS). It is one of the most common disorders and is a major health problem worldwide.1 The term “rhinosinusitis” is fast replacing “sinusitis”, because sinusitis is often preceded by rhinitis and rarely occurs without concurrent nasal airway inflammation.2,3 When rhinosinusitis is persistently present for 3 months of more, it is called chronic rhinosinusitis (CRS). This multifactorial disease has a complex nature, and the limited understanding of its relationship with associated factors makes it difficult to precisely define and classify the condition. Although the mortality of the disease is low, its morbidity is high, with CRS patients demonstrating worse quality-of-life scores for physical pain and social functioning than those suffering from chronic obstructive pulmonary disease, congestive heart failure, or angina.4
The ultimate end stage of CRS is inflammatory mucosal thickening and in a subset of patients, polypoid changes.5,6 Although its histologic hallmark is persistent underlying eosinophilic inflammation,6–8 the exact cause and pathophysiology have been the source of extensive controversy. Several competing hypotheses exist regarding the underlying cause, the mechanism leading to persistence of pathology, and the categorization of patients into subgroups.9 This chapter will attempt to bring to light some of the important as well as controversial factors in the pathophysiology of CRS.
Relevant Normal Physiology of Nose and Paranasal Sinuses
To understand the pathophysiology of the disease, it is first necessary to have a brief overview of the normal physiological mechanism of the nasal cavity and PNS. The main physiological protective mechanism of this system is a functional mucociliary transport system. The various components of the mucociliary transport system of the nose and the paranasal sinuses work together in synchrony to maintain the internal milieu of this compartment. Any derangement in one or more of these components can lead to a disruption of this ‘fine-tuned’ process, leading to stasis of mucus and infection or inflammation.
Drainage Pathways of Paranasal Sinuses
All the mucus from the nose and paranasal sinuses is transported to the nasopharynx, where it is eventually ingested and presented to the gastrointestinal tract. Understanding these pathways helps locate the obstruction to the normal outflow tracts and target the therapeutic measures to selectively correct it with minimal intervention to other areas both structurally or functionally.
The pioneering work by Messerklinger in the 20th century highlighted the importance of mucociliary transport pathways for the paranasal sinuses and the nose. His observations have stood the test of time and are till date considered relevant in the management of sino-nasal pathology. In fact, they have formed the basis of functional endoscopic sinus surgery (FESS), wherein unlike the earlier radical external approaches to the paranasal sinuses, the endoscopic approach addresses and attempts to correct the mucociliary transport mechanism defects that have been deranged due to sinusitis in a minimally invasive manner, so as to eventually restore ventilation and drainage of the nose and the paranasal sinuses.
Physiological Protective Nature of Mucus Layer
The sinonasal epithelium is covered by a mucus blanket with dynamic properties. When aerosolized pathogens and particles larger than 0.5–1μm pass through the nasal cavities, they become entrapped in this mucus layer. Through the beating action of the cilia, the debris laden mucus is propelled to the pharynx, where it is swallowed.11
The mucus blanket consists of two layers—an inner sol and an outer gel phase. The sol phase is continuous, has lower viscosity level, is comprised of water and electrolytes, and surrounds the shafts of the cilia. The gel phase is discontinuous, has higher viscosity, and rides along the tips of the extended cilia.
The mucus layer is mainly composed of water (95%), with other components such as peptides, salts and debris. It has a slightly acidic pH of 5.5–6.5 and is immunologically active.12 In addition to acting as a medium for trapping foreign inhaled material, the mucin of this layer binds to surface adhesions on microorganisms to contribute to the respiratory host defense. This specific adhesivity between the microorganisms and the mucus provides additional protection by optimizing the clearance.11 The mucus also has chemical and biologic enzymatic activity, which helps in maintaining the immune defense of the nose and paranasal sinuses.
Role of Pseudostratified Ciliated Columnar Epithelium and Ciliary Motility
The sinonasal mucosa is lined by pseudostratified ciliated columnar epithelium with goblet cells, akin to respiratory epithelium. The epithelium of each part of the nasal cavity is customized for the particular function of that region. In the anterior portion, the nasal vestibule, the epithelium is stratified squamous with sebaceous glands, sweat glands and vibrissae. This forms a barrier, like skin. At the nasal valves, a transition occurs to pseudostratified ciliated columnar epithelium. This epithelium is found throughout the sinonasal compartment, with the exception of the olfactory epithelium.13 Each ciliated epithelial cell of the sinonasal cavity has hundreds of motile cilia and even more number of immotile microvilli along its apical surface.
Cilia are cylindrical organelles protruding from the apical surface of epithelial cells. These are anchored to the cells by intracellular basal bodies derived from centrioles. Cilia are responsible for clearing the mucus belt with the entrapped debris from the nose and PNS. This mechanism is so powerful and efficient that it can clear the mucus blanket of the entire nose or sinus in 10 minutes14 The mechanism of ciliary motion depends on a series of ATP-dependent molecular motors that cause the outer doublets of the axoneme to slide relative to each other, producing a vector force.11 All the cilia beat together in a coordinated fashion to produce what is referred to as a metachronous wave.15 At the individual level, each cilium has a forward power stroke followed by a recovery stroke. During the power stroke, the cilium is fully extended and at the apogee of the arc with the distal tip making contact with the viscous outer mucus layer (gel phase), thereby transmitting directional force to the overlying mucus blanket. During the recovery stroke, the cilium bends 90˚ and sweeps back to its starting point within the thinner periciliary fluid layer (sol phase).
The microvilli are thin hair-like projections of actin filaments, about 1–2mm in length, covered by cell membrane. The main function of microvilli is most likely to increase the apical surface area of the cell, thereby increasing the exchange process across the epithelium and optimizing secretory functions. The microvilli also prevent drying of the surface by retaining moisture. The ciliated epithelial cells contain numerous mitochondria in the apical compartments generating the energy substrate necessary for the microvilli and cilia, as well as for its secretory and transport function. The goblet cells of the epithelium contribute to the respiratory secretions by virtue of mucus production.11
Anatomical Variations Influencing the Development of Rhinosinusitis
Along with an understanding of the normal physiology and protective mechanisms of the nose and PNS, it is important for the clinicians to be aware of the anatomical variations commonly encountered. Knowledge of the anatomical variations can help in determining the potential pathway of spread of disease from one “compartment” to another as well as serve as a road map for the endoscopic sinus surgeon so as to avoid a potentially hazardous surgical outcome. An anatomical variation may at times be the cause of the disease by blocking the normal drainage of the PNS. However, it must be kept in mind that sinusitis is not merely an anatomical problem, but an entity that occurs due to an infection, superimposed by mucosal and airflow changes within the nasal and paranasal sinus cavities, in individuals, who may be anatomically and genetically predisposed.
Detection and documentation of anatomical variations can be done effectively using CT scan. Some commonly seen anatomical variations are described in the following section.
Variations of Uncinate Process
The upper end of attachment of the uncinate process may give clue to the nature of spread of infection from the ethmoid to the maxillary and frontal sinuses. If the uncinate process is attached to the middle turbinate (Figure 1), then infection may spread from the frontal to the maxillary sinus. Conversely, if it is attached to the lamina papyracea, then the outflow track from the frontal recess would be isolated from the maxillary sinus, not allowing for spread of infection.
Also, an enlarged or even pneumatized uncinate process may normally lie in close proximity to the ethmoidal bulla. In such a case, minimal edema will allow for abutment of the two, causing a potentially lower threshold for the occurrence of maxillary sinusitis.
Variations in Bulla Ethmoidalis
Similar to an enlarged or pneumatized uncinate process, a well-pneumatized bulla ethmoidalis can also narrow the infundibulum, allowing for a lower threshold to the development of maxillary sinusitis.
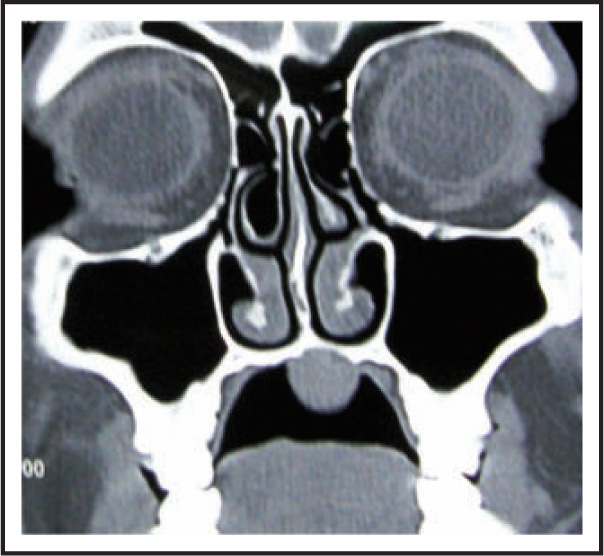
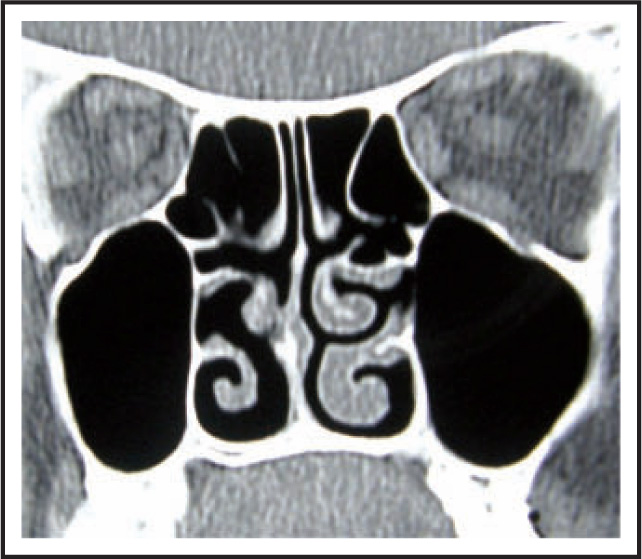
Variations of Middle Turbinate
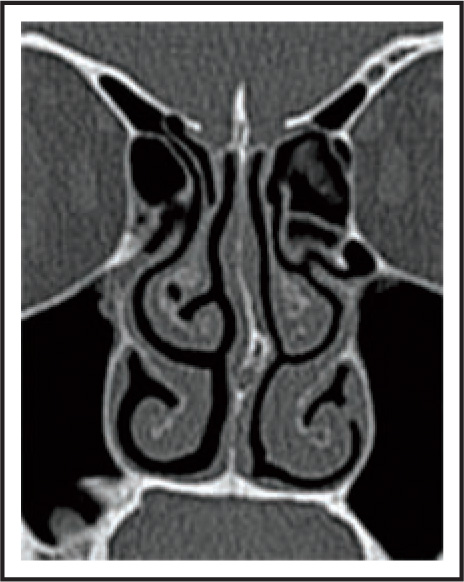
The middle turbinate may have a large concha bullosa (Figure 2), which may pneumatize from the frontal recess (Figure 3), and thus, disease from the frontal recess may affect and concurrently involve the concha.


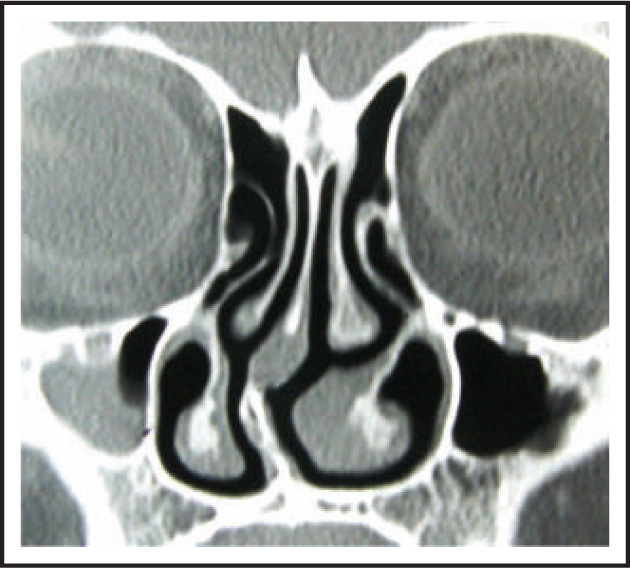
The middle turbinate may be paradoxically bent (Figure 4), with its convexity toward the middle meatus, causing severe narrowing of the same, and thus become a potential for the occurrence of sinusitis following mucosal pathologies.
Accessory Ostia
Accessory ostia may be seen commonly in the anterior and posterior fontanelles of the medial wall of the maxillary sinuses. Their presence may be the cause of formation of local eddy currents between the true and accessory ostium, leading to recirculation of mucus, which would normally follow its pathway toward the nasopharynx. This re-entry of the once exited mucus from the maxillary sinus could carry nasal passage infections into the sinuses, causing maxillary sinusitis, despite having an open/unobstructed maxillary sinus ostium. Accordingly, it must be kept in mind during endoscopic sinus surgery, to join the accessory to the true ostium, so as to prevent recurrence of the maxillary sinusitis. (Figure 5)

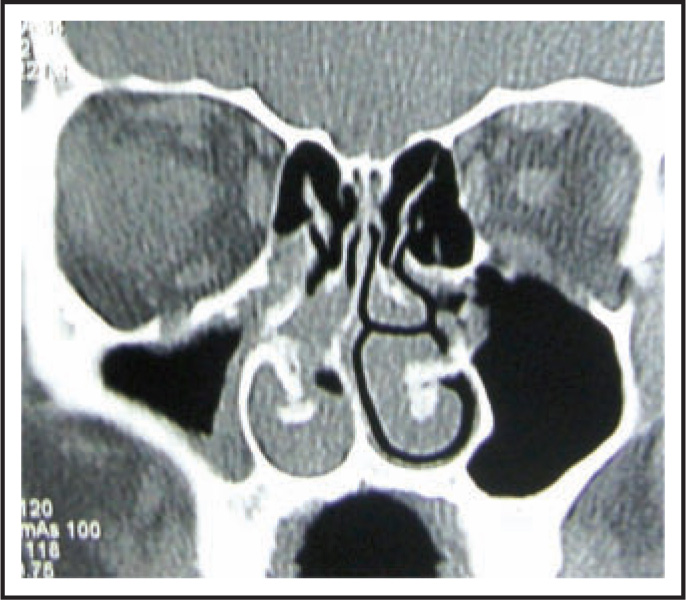
Deviated Nasal Septum
A deviated nasal septum may potentially cause narrowing of the meatii on the side of the convexity/angulation of the deviation (Figure 6). This may not, however, necessarily cause ipsilateral sinusitis. In fact, many a time, the sinusitis has been seen to occur on the opposite side (Figure 7).

Nasal Masses
Bulky nasal masses may sometimes cause “post-obstructive” changes within the sinuses, which may be reversible with the removal of the primary pathology. This may not be true sometimes in cases of very long-standing disease, wherein the sinus pathology may have to be addressed simultaneously with the nasal problem (Figure 8).
Haller Cell
An anterior ethmoid cell lying between the maxillary sinus and the orbit is known as a Haller cell, and its presence may cause obstruction of the maxillary sinus outflow (Figure 9).
Potential Causes of Chronic Rhinosinusitis
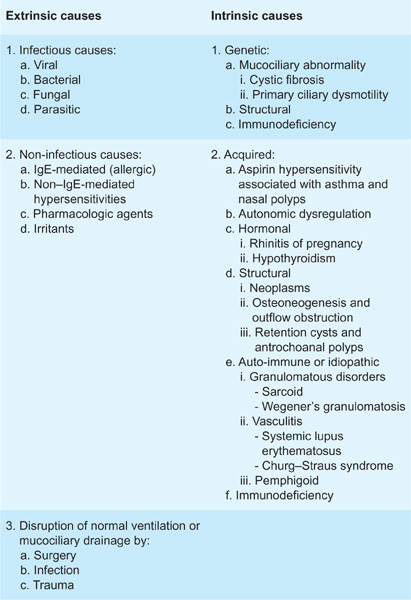
As stated before, CRS is a multifactorial disease and most of the time the long-standing duration of clinical features, the possible overlap between exposure to potential causative factors, and presence of intrinsic and extrinsic factors contributing to the condition make it difficult to classify or pinpoint the exact etiology. Benninger et al16 have proposed a system of classification for potential causes of CRS, which is exhaustive yet precise (Table 1). However, to prevent this section from becoming a didactic review, we have addressed a few of the salient and clinically relevant potential etiologies and pathogenesis mechanisms with special focus on recent views and future trends.
Table 1 Extrinsic and Intrinsic Potential Causes of Chronic Rhinosinusitis
Role of Infections in Chronic Rhinosinusitis
Sinusitis generally develops as a complication of viral or allergic inflammation of the upper respiratory tract.17 Although bacteria can be found in the sinuses of most patients who have CRS, the exact etiology of the inflammation associated with this condition is uncertain.18,19 The evolution of rhinosinusitis with infection as a possible causative factor occurs in a phase-wise manner, as described below.
Phases of Infective Chronic Rhinosinusitis
The phases of sinusitis depicted here were studied by performing serial cultures in patients with maxillary sinusitis20:
• The early phase: This is often a viral infection that lasts up to 10 days, with complete recovery occurring in most individuals.21
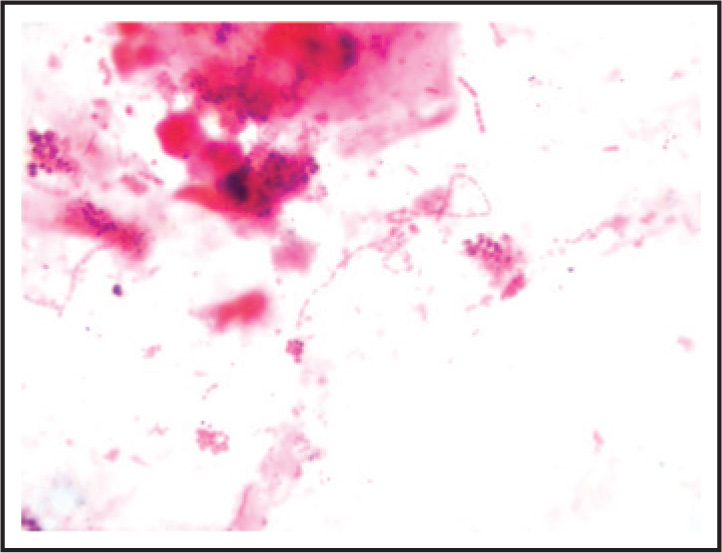
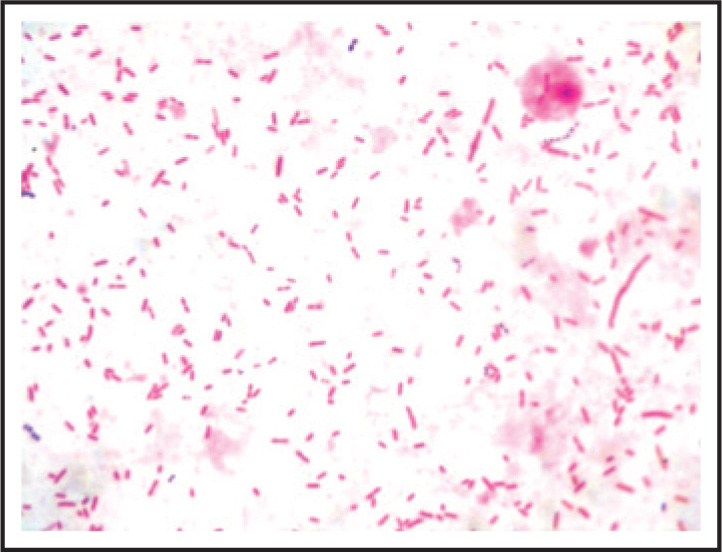
• Secondary acute bacterial infection: This usually develops in a small number of patients (about 0.5%) with viral sinusitis. It is generally caused by facultative aerobic bacteria such as Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis (Figures 10 and 11).
Bacterial Infection as Etiological Factor—Proof For and Against
Although bacteria have been isolated during the various phases of rhinosinusitis, there are quite a few findings that go against the belief that they may be the primary causative organisms, especially in cases of CRS with nasal polyposis. Some of the reasons why bacteria cannot conclusively be implicated even after being isolated from the diseased PNS include the following17:
From the points stated above, it is evident that noncontaminated collection of sample from the proper site plays an important role in narrowing down the cause of the disease. In an ideal scenario, this sample should be collected preferably from the infected sinus exclusively. A study by Brook22 demonstrated differences in the distribution of organisms in a single patient, who suffers from infections in multiple sinuses. He emphasized the importance of obtaining cultures from all infected sinuses. But then in such a scenario, culture of targeted sinus mucosal biopsies would be the only plausible option available for a near accurate diagnosis, which would then mean the requirement of surgical biopsies for all patients in the quest of diagnosis. As this is not practically acceptable, the clinicians usually opt for the most accessible areas to collect the sample. Due to the accessible location of the maxillary sinus, it is usually the sinus of choice for sampling to obtain specimens for culture.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


