Introduction
Chronic rhinosinusitis (CRS) is characterized by a number of debilitating features such as mucopurulent drainage, nasal obstruction, facial pain/pressure/fullness and decreased sense of smell persisting for 12 or more weeks.1,2 It may also be associated with purulent mucus or edema in the middle meatus or ethmoidal region, polyps in nasal cavity or the middle meatus and/or radiographic evidence of paranasal sinus inflammation. Despite the fact that maximal medical therapy is indicated in all cases and many cases do respond to it, there still exists a group of patients who improve only after surgical treatment.3–5
Sinus surgery has come a long way from the conventional open surgery to the presently practiced endoscopic surgery. This chapter will briefly describe the history of sinus surgery from the global as well as Indian perspective, outline the various aspects of endoscopic sinus surgery (ESS) and touch upon the future trends.
Evolution of Sinus Surgery
Global Update
Rhinosinusitis is a highly prevalent disease worldwide6,7 that results in a huge financial and disease burden globally.6,8 All over the world approximately 500000 surgical procedures are being performed annually on CRS patients.5
In the pre-antibiotic era, the main aim of sinus surgery was removal of pus from sinuses as a life-saving measure. As a result, decompression of maxillary sinus either by dental or inferior meatal root and “frontal sinus trephine” were the most common surgeries performed on the sinuses. In 18th and 19th century treatment of chronic sinus disease was approached by external route with the aim of removing all the diseased mucosa from the sinuses. Caldwell-Luc and external frontoethmoidectomies were the most common surgeries performed then. This was followed by the advent of endoscopic sinus surgery. Based on the work by Messerklinger,9 Stammberger10,11 described the basis of endoscopic surgery, emphasizing the role of removal of disease from ostiomeatal complex. This was later popularized by Kennedy12 who introduced the term “functional” for this kind of surgery. Other authors like Wigand13 supported a more radical posterior to anterior approach to deal with extensive polyposis as opposed to Messerklinger’s anterior to posterior approach.
Subsequent advancement in instrumentation including the recently added 3-chip digital high-definition (HD) camera with HD monitor made the quality of endoscopic images unbelievably clear resulting in more advanced and complicated work. The introduction of powered instruments such as microdebrider and high speed drills in mid-1990s was another big step in advancement of ESS especially for extensive polyposis and fungal diseases.14 In expert hands a microdebrider can reduce the duration of surgery, work in bloody field, cut more precisely and avoid undue stripping of the mucosa though the potential to cause devastating orbital and intracranial complications has to be guarded against.15 Other advances include the “image guidance system,” which was initially introduced in neurosurgery in early 80s16 and later used for ESS in late 90s.17 It has revolutionized extensive sinus diseases, revision surgeries and resection of anterior and middle skull base lesions.18 Endoscopic balloon dilatation sinuplasty is the latest addition in this armamentarium and has shown promising results in terms of safety, patient comfort and success for both adult and pediatric patients.19–22
Indian Perspective
A major portion of surgical workload of an ENT surgeon these days in India is related to sinus diseases. The evolution of sinus surgery in India has been following the global pattern, though there is a paucity of data to support the same. When the senior author was doing his postgraduation in 1989–92, the most commonly performed surgeries for chronic sinusitis were antral washout, Caldwell-Luc and Lynch-Howarth frontoethmoidectomy. Occasionally intranasal ethmoidectomies using microscope and osteoplastic flap for frontal sinus were performed. When the second author was doing his post-graduation in the same department in 1993–96, ESS without camera and monitor were started though most of the extensive cases of fungal sinusitis were still being dealt with external approaches. Nowadays conventional surgery is rarely being performed in the same department. This series of changes reflect a parallel for Indian pattern.
Some credit for this change is due for the Indian-born foreign faculties such as Dr. D.S. Sethi (Singapore), Dr. Kalusker (Ireland), Dr. Dinesh Mehta (USA), and Dr. Nikhil Bhatt (USA) who in the late 80s and early 90s started conducting ESS courses in India, creating awareness and teaching this new technique to many ENT surgeons. The contribution of Dr. V.P. Sood, the editor of this book, also cannot be ignored who along with Dr. Dinesh Mehta conducted an ESS course for the first time in India in 1989. Unfortunately an adverse effect of this phenomenon is that the new generation of surgeons are unlikely to have the required skill to perform conventional sinus surgeries which are sometimes necessary to revise failed ESS cases, deal with complications of sinus surgery or manage sinonasal tumors.
Another distinct feature of practice in India is that a large number of patients have allergic fungal sinusitis (AFS) and present with extensive disease with massive polyposis and altered anatomy. In senior author’s practice, about 40% of sinus surgeries are related to AFS. There is literature from other major institutes of India which indirectly indicate similar numbers.23,24
Indian surgeons are now using most of the advanced equipment for ESS. Good quality camera and monitor as well as microdebrider are being used routinely by most surgeons though the use of navigation system and “balloon-dilatation” is still very limited. With more and more corporate hospitals coming up in India, it is likely that these latest gadgets too will be used by more number by surgeons in future.
Surgical Management: Indications, Contraindications and Goals
Other than CRS not responding to optimum medical management, the other cases of rhinosinusitis for which sinus surgery is indicated include recurrent acute rhinosinusitis, allergic fungal sinusitis, sinonasal polyposis, acute rhinosinusitis with complications, sinus mucoceles and antrochoanal polyps.
The contraindications for surgical treatment include:
• Patient having extensive polyposis or AFS who is not likely to adhere to post-op prolonged medical treatment.
• Patient having chief complaints of “headache” or midfacial pain which is unlikely to be of sinus origin even though CT scan might show sinus opacity.
• Frail patient or other medical condition making surgery a highly risky proposition.
• Grossly hypoplastic sinuses and/or thick bones (this is a relative contraindication).
Endoscopic sinus surgery aims to reduce the disease in patients with rhinosinusitis by:
• Removal of pathological tissue from ostiomeatal complex area, which helps in restoration of mucociliary function of sinus mucosa.
• Ventilation of sinuses that helps in reduction of number of mucosal glands and goblet cells population leading to decreased nasal secretions.
• Clearing the pathway for better delivery and distribution of topical nasal medication in the nose and sinus mucosa.
• Reduction of diseased sinus mucosa surface area by removal of polypoidal disease.
• Improvement of ‘olfaction’ by opening superior meatus and sphenoethmoid recess.
• Relief from the nasal obstruction in cases with gross surgical anatomic variations such as concha bullosa or big spur.
Pre-Operative Considerations
Pre-operative Evaluation
Pre-operative evaluation consists of selection of a patient who is likely to be benefited by surgical intervention. Usually this consists of making a correct diagnosis and adequate pre-operative counseling of the patient.
A correct diagnosis can be arrived at by a thorough history taking, nasal examination and radiological investigations. Details about the diagnostic modalities are mentioned in chapter “Diagnosis of Chronic Rhinosinusitis”. The history taking should identify the chief symptoms, associated contributory conditions, any immuncompromised status, comorbidities and details of medical treatment received till that point. Nasal examination, usually by an endoscope should try to identify the structural abnormalities in the nose and carry out a thorough inspection of middle meatus and sphenoethmoid recess. The radiological examination in the form of CT scan is required for all the CRS patients who have not improved despite optimal medical therapy. Besides this a pre-operative CT scan checklist (detailed later in this chapter) is mandatory before initiation of the surgery in all cases.
Once a correct diagnosis is reached, adequate counseling of the patient regarding nature of the disease, available treatment options, benefit and limitations of the surgery, postoperative care, postoperative medical treatment, chances of success/failure and potential complications should be discussed. An informed consent is a must to avoid medicolegal implications later.
Pre-operative Medical Treatment
Although the candidate for surgery of CRS is one who has not responded to medical treatment, a course of medical treatment is still indicated pre-operatively to optimize the nasal mucosa at the time of surgery. Preoperative medical treatment is individualized based on patient symptoms and nasal endoscopic findings. Usually it includes 2–3 weeks of culture-directed antibiotic in patients with CRS without polyps. Antihistamines and intranasal steroid spray are added in patients who give history of nasal allergy. Oral itraconazole is added in patients of fungal sinusitis. In patients of extensive polyposis, oral steroids along with steroid spray are prescribed. Also any antiplatelet agent that the patient may be taking should be stopped a week before surgery.
Anesthesia for Endoscopic Sinus Surgery
Most of our patients are now being operated under general anesthesia. Although it is possible to do ESS using local anesthetics with i.v. sedation, we offer this technique to the patient only if there is limited disease or patient’s condition does not permit general anesthesia without significant risk. During surgery, the anesthetist is requested to maintain mean arterial pressure between 60mmHg and 80mmHg and pulse rate below 70/minute.
Preparation of Nasal Cavity before Surgery
We usually pack the nasal cavity with two cottonoid packs each side, soaked and squeezed with 4% xylocaine with 1:1000 adrenaline solution approximately 15 minutes before shifting the patient into the theater. Once the patient is anesthetized and intubated, these packs are removed and 2 fresh packs soaked in same solution are kept under endoscopic guidance in middle meatus and nasal cavity for 10 minutes more. After removing these packs, local infiltration with 2% xylocaine and 1:200000 adrenaline is done using 24-guage spinal needle. The usual sites of infiltration are areas just above the anterior end of middle turbinate, just below and lateral to the posterior end of middle turbinate (sphenopalatine area), middle part of uncinate, and anterior surface of concha bullosa if present. After infiltration, nose is again packed with same cottonoids soaked in 4% xylocaine with adrenaline for another 15 minutes.
Pre-operative CT Scan Checklist
Before performing the surgery and while waiting for decongestion of the nasal cavity, it is advisable that the surgeon should go over the CT scan findings once again. The important CT findings to be looked are described with each step of surgical technique later in this chapter, the main points of which are summarized below. The surgeon should:
• Look for any dehiscence in lamina papyracea.
• Make a note of type of skull base (e.g. Kero’s I, II or III and variation in height on either sides) and look for any dehiscence in the skull base.
• Note the position of anterior ethmoidal artery and the mesentery.
• Look for the presence or absence of any “Onodi direct positive or indirect positive” situation.
• Look at bone covering the optic nerve, the lateral wall of sphenoid and presence of Haller cells.
Surgical Technique
The patient is positioned supine on the OT table with head end elevated by 30°. The head is kept in the neutral position (neither extended nor flexed) and turned slightly towards the surgeon. Both eyes are taped and the patient is draped in such a manner that both eyes are left uncovered.
The surgeon usually operates from the right side, the nurse and instrument trolley are stationed at the head end, monitor is kept on the left side near the head end and anesthetist along with the anesthesia monitor and machine are positioned at the foot end on the left side. The method described below follows the usual anterior to posterior approach of Messerklinger practiced by most surgeons.
Uncinectomy
Uncinectomy is usually the first step of the surgery and one of the causes of failure of ESS is poorly performed uncinectomy.25 Radiology check points before starting this step include looking for any dehiscence in the lamina papyracea, define the posterior free edge of uncinate (seen in posterior cuts only) and noting the distance between uncinate process and lamina papyracea. The surgeon should also trace the upper part of uncinate in anterior cut and look for its attachment to lamina papyracea directly or through Agger nasi cell, skull base or middle turbinate. The position of medial wall of maxilla with respect to the vertical plane of lamina papyracea should also be noted as a lateral placement may make it difficult to locate the maxillary ostia. The presence of maxillary sinus hypoplasia should also be looked for as it is commonly associated with the alternate positioning stated above.
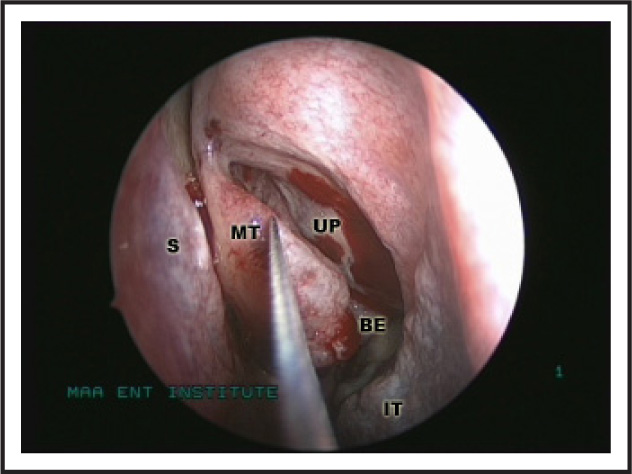
Before starting the surgery, it is also prudent to do a thorough nasal endoscopy again to understand the particular nose. In case middle turbinate is obstructing the instrumentation, it can be medialized gently with Freer’s elevator (Figure 1). Any pus or fungal mucin can be collected for further microbiological studies.
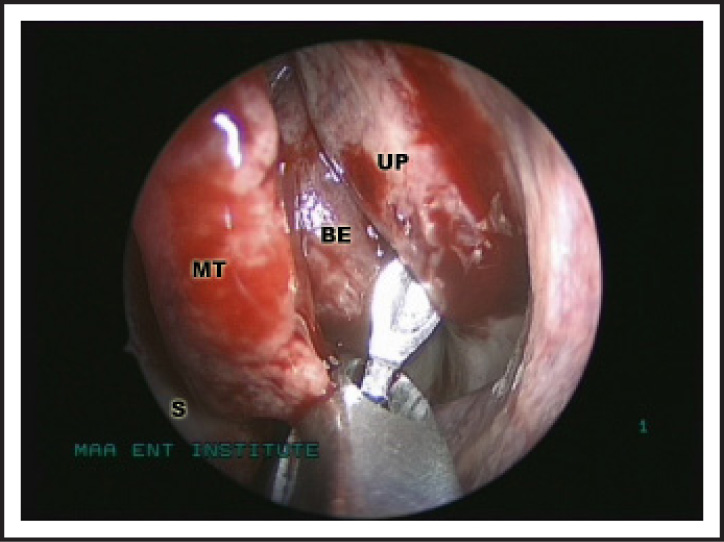
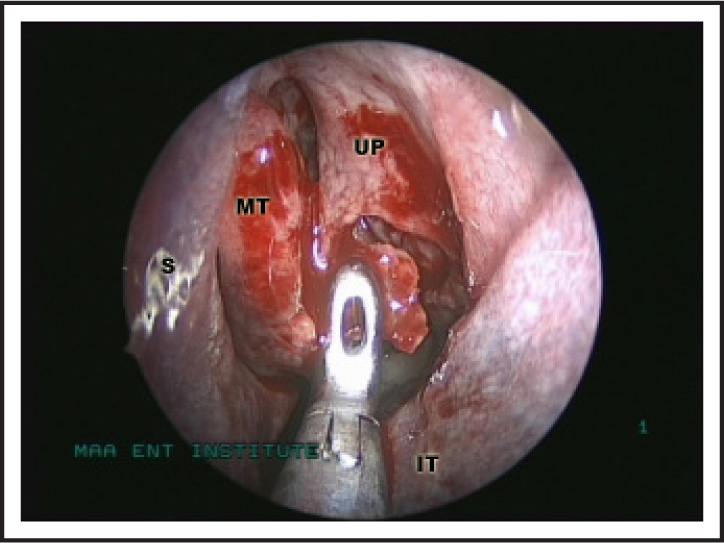
The surgeon should first identify the middle ⅓rd of free border of the uncinate by using a ball-tipped right angle probe. The distance between free border of uncinate and medial wall of orbit should then be estimated by putting the probe through hiatus semilunaris into the infundibulum (Figure 2). A back biting forceps is opened facing the anterior wall of the bulla and by rotating it to 90°, the free border of uncinate is engaged in it at the junction of vertical and horizontal part of uncinate. At this stage the surgeon should close the jaw of the back biting forceps gently and move it medially. The movement of the jaw should be visible through the intact uncinate. If not, then the surgeon should withdraw the backbiter and reposition it. By taking this precaution one can avoid injury to the lacrimal duct. If the positioning is correct then the jaws of the backbiting forceps should be closed to cut the uncinate process (Figure 3) until the vertical and horizontal parts of uncinate are completely divided. The vertical part of uncinate should be slightly medialized using ball-tipped probe and removed using either microdebrider or 90° upturned Blakesly forcep. One should change to 30° endoscope at this stage. Horizontal part of uncinate is then dissected out between the two layers of mucosa with the help of ball-tipped probe taking care to cut all pseudopodia-like processes that attach the horizontal part of uncinate to the upper surface of inferior turbinate.
Alternate Techniques of Uncinectomy
Another conventional technique used by surgeons11 has described the removal of uncinate process by making an incision near its anterior attachment to lateral wall of nose using either sickle knife or sharp edge of Freer’s elevator. This method requires that the line of attachment of uncinate with lateral wall of the nose should be palpated first before making the incision. A microscissor can then be used to cut the upper and lower end of remaining attachment of uncinate and horizontal part is removed in the usual manner as described earlier.
The technique described by Wormold26 is named as “swing door technique”. This is similar to the technique described above except that the superior horizontal cut by sickle knife is made near the axilla of middle turbinate in vertical part of uncinate. Then the uncinate is swung medially like a “door” and subsequently removed.
Middle Meatal Antrostomy
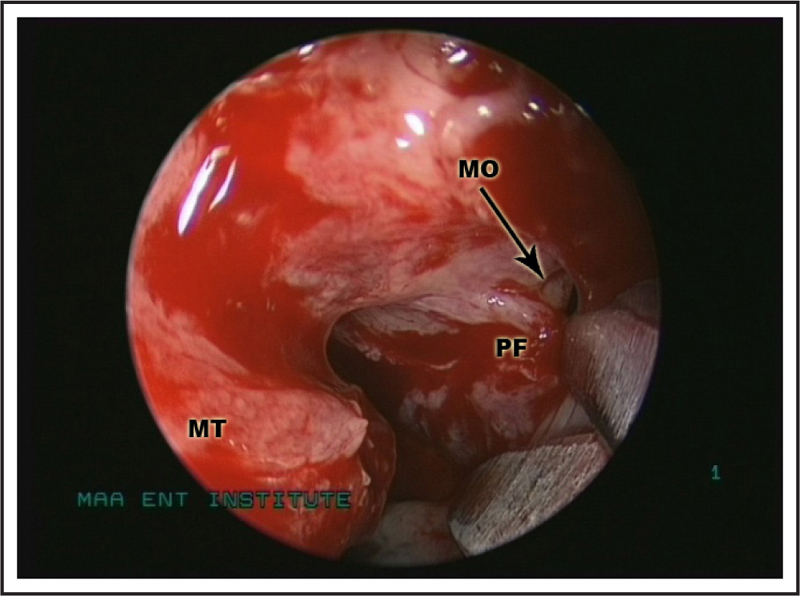
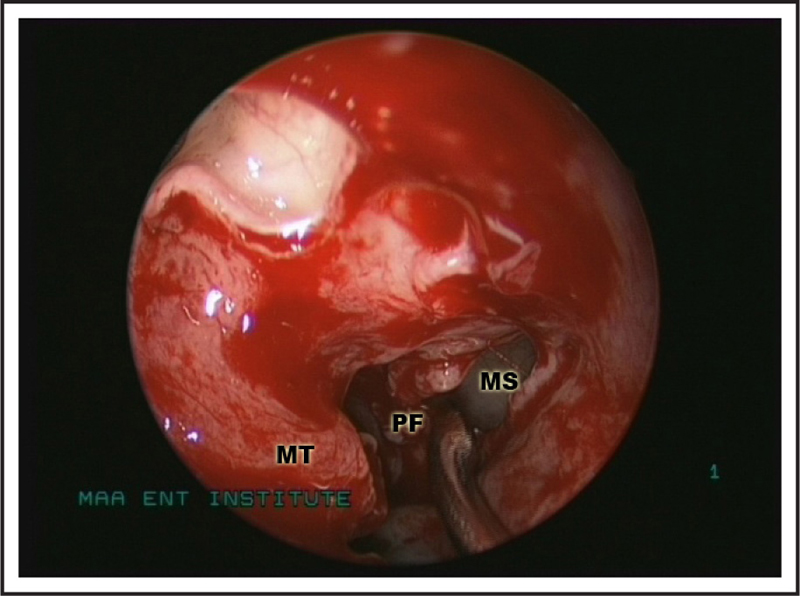
Uncinectomy is followed by middle meatal antrostomy (MMA). Removal of uncinate process opens the infundibulum. The antero-inferior corner of infundibulum contains the natural opening of the maxillary sinus, which is a short, oval, three-dimensional tract. The maxillary sinus opening is easily identifiable with a 30° nasal endoscope (Figure 4). If it is not visualized clearly, gentle pressure on the posterior fontanelle by a ball-tipped probe or curved suction cannula will displace the air in the maxillary sinus through the ostium resulting in an air bubble that indicates the location of the ostium. Once the ostium is identified, it is widened (Figure 5). There is lot of controversy on how much widening of maxillary sinus is ideal. The authors feel that it should be guided by the extent of pathology in the maxillary sinus. If maxillary sinus opening is wide and patent and there is not much disease in the maxillary sinus, one need not further widen the maxillary sinus. If there is an accessory ostium, it needs to be joined with natural opening.
The ostium is enlarged by introducing one blade of a curved cutting scissors into the maxillary sinus through the natural opening and making a cut flush with the roof of the sinus. The inferior part of posterior fontanelle is then everted using a curved curette. It can be trimmed further using shavers or sharp straight scissors. A further widening, if needed, can be done using Stammberger’s ostium back-biting punch. However it is advisable to preserve the mucosa in this region to avoid postoperative lymphedema of maxillary sinus mucosa. One should not go too anterior as it may damage nasolacrimal duct. Once antrostomy is done whole of interior of maxillary sinus should be inspected using all angled telescopes including 90° one. All pus, mucin, fungal elements, foreign body, polyps, cyst or pyocele should be removed from the sinus. Sometimes removal of the polyp or cyst from anterior wall needs introduction of microdebrider blade through inferior meatus or canine fossa.



