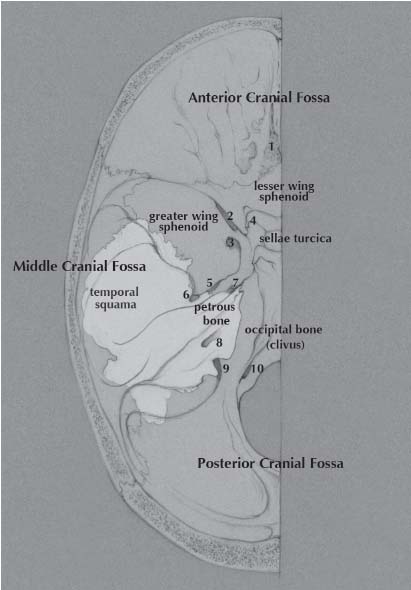
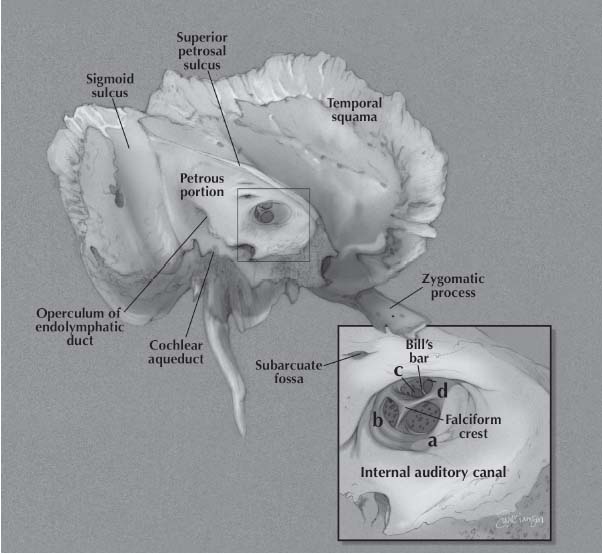
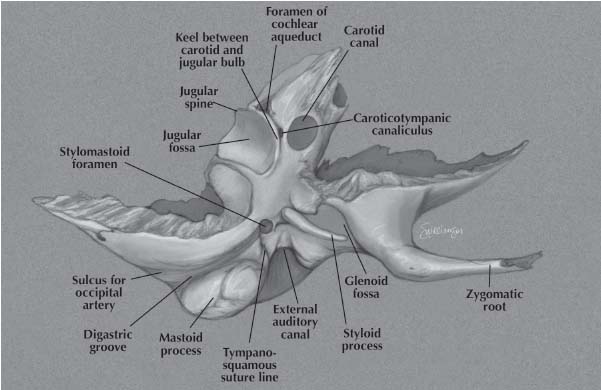
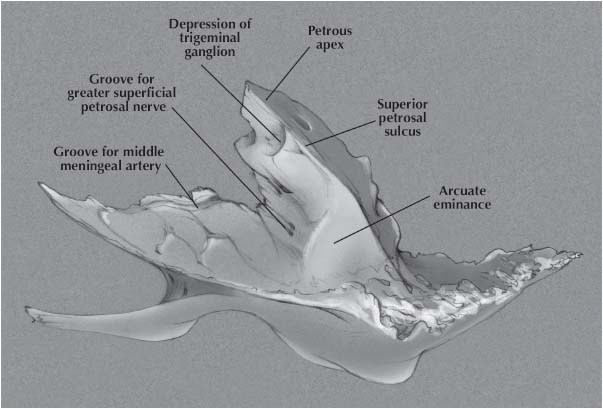
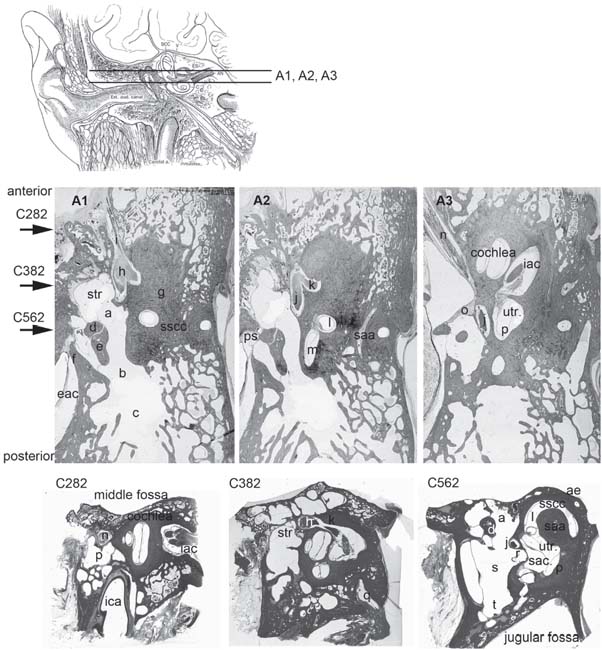
2 Multiple intra- and extra-cranial regions interface with the temporal bone (Fig. 2.1). This anatomy reflects its unique role in the embryology of the head and neck. The temporal bone articulates with the sphenoid, parietal, occipital and zygomatic bones, therefore contributing to the cranial, skull base and facial structure. The temporal bone has a pyramidal shape, the sides of which form the middle fossa floor (superior face), the anterior limit of the posterior fossa (posterior face), muscle attachments of neck and infratemporal fossa (anterior-inferior face) and the muscular-cutaneous-covered side of the head (lateral) which forms the base of the pyramid. The temporal bone consists of four embryologically distinct components: the squamous, mastoid, petrous and tympanic parts.1 The squamous part (temporal squama) forms the lateral wall of the middle fossa (Figs. 2.1, 2.2, 2.3). It consists of inner and outer cortical plates with intervening diploe and an anterior extension known as the zygomatic process, which forms the bony roof of the glenoid fossa. A horizontal ridge, the temporal line is formed along the most inferior insertion by the temporalis muscle and is aligned with the zygomatic process. The temporal line provides a first approximation for the location of the middle fossa floor,2 which on average is positioned ~4.7 mm inferiorly. Fig. 2.2 Lateral view of the temporal bone. Fig. 2.3 Medial view of the temporal bone. The mastoid part is a bulbous bony structure shaped by the expansion of air-filled spaces within (Fig. 2.2). The constant pull by the sternocleidomastoid muscle (SCM) and posterior belly of the digastric muscle elongates the mastoid inferiorly to form the mastoid tip or process. The mastoid cortex is perforated by multiple small emissary vessels that drain from the central air cell or antrum, forming a triangular (Macewan’s triangle) and depressed cribriform area at the anterior junction of the mastoid process with the tympanic bone. The foramen of a single emissary vein is evident near the posterior limit of the outer mastoid cortex and communicates with the sulcus of the sigmoid sinus, which is evident on the posterior medial aspect of the temporal bone. The site of SCM insertion is indicated by a rough and irregular surface at the mastoid tip. Medial to the mastoid tip, the posterior belly of the diagastric muscle is inserted in a sulcus that terminates anteriorly at the stylomastoid foramen (Fig. 2.4). Medial and almost parallel to the digastric sulcus is the sulcus for the occipital artery. The tympanic part of the temporal bone forms the anterior wall, floor and part of the posterior wall and roof of the bony external auditory canal (EAC), and the anterior wall and floor of the middle ear (Fig. 2.2). The anterior edge of this open ring forms the tympanosquamous suture line within the EAC, and the petrotympanic suture line within the middle ear, through which the chorda tympani exits the ear. The posterior edge of the tympanic ring forms the tympanomastoid suture line which curves from the posterior EAC in feriorly to within millimeters of the stylomastoid foramen, serving as a landmark for the main trunk of the facial nerve as it exits the temporal bone (Fig. 2.4). The petrous part has the shape of a pyramid whose base is united with the mastoid laterally; the apex is oriented antero-medially between occipital and sphenoid bones (Fig. 2.1). The jugular foramen is formed at the junction between the petrous and occipital bones (at the clivus) and is partitioned into the pars nervosa (posterior) and pars venosa (anterior) by the jugular spine.3 The posterior surface of the petrous part of the temporal bone is oriented in the vertical plane forming the anterior bony limit of the posterior fossa (Fig. 2.3). This surface is framed by sulci for the sigmoid, superior petrosal and inferior petrosal sinuses (along the petro-clival junction). At the center of the posterior face is the porous acusticus or internal auditory meatus at the fundus of which can be seen the falciform (horizontal) crest, Bill’s bar (vertical crest), and foraminae of the cochlear nerve fibers (a), the inferior vestibular nerve (b), the superior vestibular nerve (c) and the facial nerve (d). The subarcuate artery emerges from a fossa of the same name located superior and lateral to the acoustic meatus, whereas the endolymphatic sac and duct occupy the depression and opening located infero-laterally, known as the operculum. Fig. 2.4 Inferior view of the temporal bone. Fig. 2.5 Superior view of the temporal bone. The inferior surface of the temporal bone is irregular due to the presence of multiple muscle attachments (Fig. 2.4). The styloid process is located anterior to the stylomastoid foramen, and both are located at the anterior limit in-line with the digastric groove. The jugular bulb occupies a dome shaped compartment located lateral to the the jugular foramen directly under the middle ear space. The inferior foramen of the carotid canal is located directly anterior to the jugular bulb depression, from which it is separated by a wedge shaped bone called the keel. The tympanic canaliculus penetrates the keel to transmit sensory and pre-ganglionic parasympathetic fibers from the inferior ganglion of the glossopharyngeal nerve into the middle ear as Jacobson’s nerve.1,4 The external aperture to the cochlear aqueduct is located just medial and anterior to the jugular spine within the pars nervosa and marks the most superior limit of the jugular foramen. The cochlear aqueduct eventually opens into the scala tympani at the cochlear base.4–6 In the translabyrinthine approach to the internal auditory canal, the cochlear aqueduct is an important inferior limit of dissection used to protect the lower cranial nerves.7 The anterior surface forms the postero-medial margin of the middle fossa floor (Fig. 2.5). Prominent surface features include: 1) medially, the arcuate eminence formed by the prominence of the superior SCC, and the sulcus of the superior petrosal sinus; 2) anteriorly at the junction with the greater sphenoid wing, the musculotubal canal containing the more superficial semicanal of the tensor tympani and a deeper semicanal of the Eustachian tube; and 3) at the apex a smooth depression occupied by the trigeminal ganglion, just posterior to which is located foramina and sulci of the greater and lesser superficial petrosal nerves, running parallel to the sphenoid suture line. The roof of the middle ear and mastoid extends lateral to the arcuate eminence. Review of temporal bone sections promotes better understanding of the complex anatomic relationships within the ear. Nine horizontal (axial) sections from the same ear are presented in Figs. 2.6, 2.7, and 2.8. Although not perfectly orthogonal to the horizontal series, three vertical sections from a different donor provide additional perspectives to these three-dimensional relationships. For additional details on these anatomic relationships as demonstrated in temporal bone sections publications by Nager,5 Schuknecht,4,6 and Saumil and Nadol8 are recommended. Fig. 2.6 Temporal bone histological sections. Superior axial sections (A1–3) reveal the relationship between contents of the attic, antrum, labyrinth, internal auditory canal, and first genu of the facial nerve. Coronal sections (C282, C382, and C562) from another temporal bone reveal approximate orthogonal relationships along planes indicated by the labeled arrows. a attic/epitympanum, b aditus ad antrum, c mastoid antrum, d head of malleus, e incus body and short process, f scutum, g otic capsule, h geniulate ganglion and first genu facial nerve, i
Anatomy of the Temporal Bone
 Surface Anatomy
Surface Anatomy

 Internal Anatomy
Internal Anatomy
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


