1
Anatomy and Embryology of the Ear
A. Julianna Gulya
It is incumbent upon the otologic surgeon to possess a detailed familiarity with the structure of the temporal bone and its environs. Additionally, as a number of otologic disorders are based on, or rendered more complicated by, aberrant development of the ear and temporal bone, an understanding of the normal embryologic sequences and the more common anomalies is critical to skillful otologic diagnosis and management. This chapter, in its review of the critical concepts of temporal bone anatomy and embryology, provides an important basis for better understanding the subsequent chapters. It begins with the structure of the temporal bone and the ear, followed by their development, both normal and abnormal. The interested reader is referred to Anatomy of the Temporal Bone with Surgical Implications1 for details beyond the scope of this chapter.
 Anatomy
Anatomy
Pinna
The pinna is a bilaterally symmetric, cartilage-framed, cranial appendage that serves to focus and localize sound. The precise configuration of each individual pinna displays considerable variability, owing to its multicomponent embryologic origin, but there are also constant features.
The cartilaginous frame of the pinna determines its contour, and is composed of elastic cartilage. The lateral surface of the pinna is characterized by its convexities, the dominant one being the concha, which is bordered anteriorly by the tragus, superiorly and posteriorly by the anthelix and its anterior crus, and inferiorly by the antitragus. The helix, lacking in lop ears, extends superiorly and posteriorly from its crus and ends at the lobule; the Darwinian, or auricular, tubercle, is a projection occasionally seen at its posterosuperior aspect. Another convexity is the triangular fossa, cradled by the two crura of the anthelix. The scaphoid fossa is the groove separating the helix and anthelix. The tragus is a nearly independent island of cartilage, connected to the main flange of the pinna by a narrow, inferiorly located, isthmus. The lobule is the fibrofatty inferior appendage of the pinna.
The skin and subcutaneous tissue recapitulate the irregularities of the cartilaginous frame; both the medial and lateral surfaces display hair, and sebaceous and sudoriferous glands, but the skin attachment differs, being loosely tethered on the medial aspect and snugly attached on the lateral.
The pinna attaches to the cranium by skin, cartilage, three extrinsic muscles, and extrinsic ligaments. The six intrinsic auricular muscles of the pinna are generally poorly represented in the human.
External Auditory Canal
The external auditory canal extends for approximately 2.5 cm; its lateral third is elastic, oriented posterosuperiorly, and is perforated anteriorly by two to three variably present fissures, the fissures of Santorini. The medial two thirds is osseus, oriented inferiorly and anteriorly (Fig. 1–1). The isthmus, located just medial to the junction of the bony and fibrocartilaginous canals, is the narrowest portion of the external auditory canal. Owing to the different angulations of the canal segments in the adult, the auricle must be pulled superiorly and posteriorly to allow alignment for otoscopic examination.
The skin of the osseous canal is much thinner than that of the fibrocartilaginous canal, and is lacking the usual adnexal structures, for example, hair follicles, in the subcutaneous layer. The subcutaneous layer of the fibrocartilaginous canal skin bears, in addition to hair follicles and sebaceous glands, ceruminous (modified apocrine) glands.
The sensory innervation of the pinna and the external auditory canal derives from the auriculotemporal branch of the trigeminal nerve, the greater auricular nerve of C3 origin, the auricular branch of the vagus, and twigs from the facial nerve. The auriculotemporal nerve innervates the anterior canal wall and tympanic membrane, as well as the anterior aspect of the pinna. The greater auricular nerve supplies the mastoid process and both lateral and medial aspects of the posterior pinna and tympanic membrane. The auricular branch of the vagus innervates the inferior bony canal and tympanic membrane, the posterosuperior cartilaginous canal, and the cymba concha. Branches of the facial and chorda tympani nerves innervate the posterosuperior bony external auditory canal.
Number key for Figures 1-1 to 1-5 1, external auditory canal; 2, fossa mastoidea; 3, squama; 4, mastoid tip; 5, tympanomastoid suture; 6, zygoma; 7, glenoid fossa; 8, temporal line; 9, petrotympanic fissure; 10, styloid process; 11, middle meningeal artery sulcus; 12, petrous bone; 13, internal auditory canal; 14, sigmoid sulcus; 15, superior petrosal sulcus; 16, inferior petrosal sulcus; 17, petrous apex; 18, arcuate eminence; 19, internal carotid artery foramen (internal); 20, tegmen; 21, facial hiatus; 22, stylomastoid foramen; 23, jugular fossa; 24, internal carotid artery foramen (external); 25, cochlear aqueduct; 26, endolymphatic fossette.
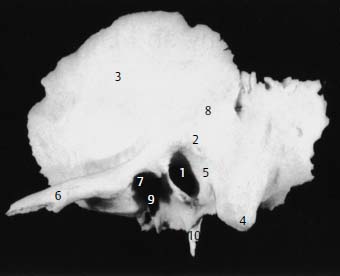
Figure 1–1 Left temporal bone, lateral view.
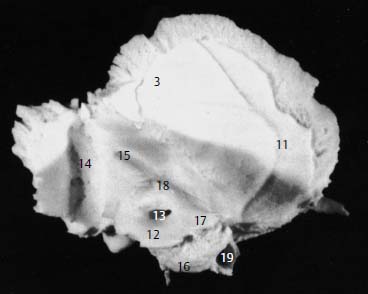
Figure 1–2 Left temporal bone, medial view.
Temporal Bone
The tympanic bone of the osseous external auditory canal constitutes one component of the temporal bone; the petrous, squamous, and mastoid bones constitute the remaining portions, whereas the styloid process represents a separate bone (Figs. 1–1 to 1–5). The temporal bone articulates with the zygomatic, sphenoid, parietal, and occipital bones, and forms part of the lateral and posterior cranial fossae as well as the lateral wall and base of the skull.
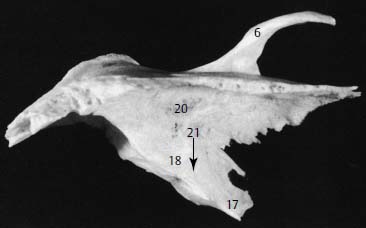
Figure 1–3 Left temporal bone, superior view.
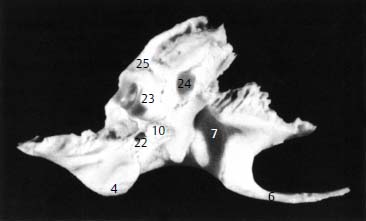
Figure 1–4 Left temporal bone, inferior view.
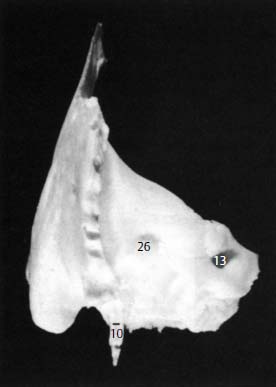
Figure 1–5 Posterior surface of temporal bone.
The petrous portion of the temporal bone is the pyramidal core of the temporal bone and houses the inner ear. Its superior surface (Fig. 1–3), marked by the arcuate eminence, the tegmen of the tympanomastoid compartment, and the trigeminal impression for the fifth cranial nerve, makes up part of the floor of the middle cranial fossa. The facial hiatus, located anterior to the arcuate eminence, marks the exit of the greater superficial petrosal nerve from the geniculate ganglion. The posterior face (Fig. 1–5) of the petrous bone lies vertically between the superior petrosal sinus and the inferior petrosal sinus as it forms the anterolateral wall of the posterior cranial fossa. The porus of the internal auditory canal, the subarcuate fossa, and the endolymphatic fossette for the endolymphatic sac are located on the posterior face of the petrous bone. At the apex of the petrous bone, which is oriented anteromedially, the internal carotid artery exits its intrapetrous course, closely approximated by the orifice of the eustachian tube and the lesser superficial petrosal nerve. The inferior aspect (Fig. 1–4) of the petrous bone is highly irregular, providing attachment for several deep neck muscles, and is punctuated by the foramina for the internal carotid artery and the jugular bulb, separated by the jugulocarotid crest, housing the inferior tympanic artery and Jacobson’s nerve (the tympanic branch of the ninth cranial nerve). The cranial orifice of the cochlear aqueduct opens at the medial aspect of the jugular fossa, whereas the styloid process arises posterolaterally. The stylomastoid foramen of the facial nerve arises posterior to the styloid process.
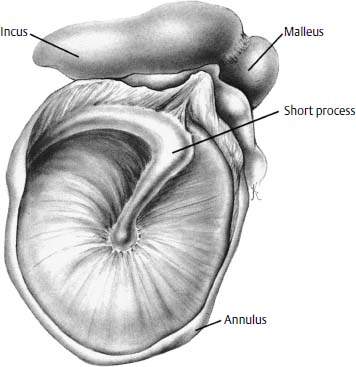
Figure 1–6 Lateral view of the right tympanic membrane.
The squamous portion of the temporal bone (Figs. 1–1 and 1–2) forms the lateral wall of the middle cranial fossa, and articulates with the parietal bone superiorly and anteriorly with both the zygoma (by means of the zygomatic process) and the sphenoid bone. Arterial sulci mark both its lateral (the middle temporal artery) and medial (the middle meningeal artery) surfaces.
The mastoid portion of the temporal bone (Figs. 1–1, 1–4, and 1–5) comprises inferiorly directed projections of both the petrous (medially) and squamous (laterally) portions, separated by Koerner’s (petrosquamous) septum. Posterosuperior to the external auditory canal opening lies the spine of Henle, posterosuperior to which is the fossa mastoidea, or Macewen’s triangle, which laterally overlies the mastoid antrum. The mastoid incisure accommodates the posterior belly of the digastric muscle; medial to the mastoid incisure is the temporal groove for the occipital artery. The mastoid foramen marks the passage of the mastoid emissary vein, located posteriorly on the lateral surface of the mastoid.

Figure 1–7 Normal right tympanic membrane.
The tympanic portion of the temporal bone (Fig. 1–1) joins the mastoid at the tympanosquamous suture, and constitutes the inferior, anterior, and part of the posterior external auditory canal. The petrotympanic fissure represents the interface of the tympanic bone with the petrous bone, and is traversed by the chorda tympani nerve, the anterior tympanic artery, and the anterior process of the malleus. An inferior projection of the tympanic bone, the vaginal process, forms a sheath for the styloid bone. At the medial aspect of the tympanic bone is a groove (the annular sulcus), deficient superiorly (the notch of Rivinus), which houses the tympanic membrane annulus.
Tympanic Membrane
The tympanic membrane (Fig. 1–6) is an irregular cone, the apex of which is located at the umbo, corresponding to the tip of the manubrium (Figs. 1–7 and 1–8). In the adult, the tympanic membrane measures about 9 mm in diameter, and rests at a 140-degree angle with the superior wall of the external auditory canal. The tympanic membrane is firmly attached to the malleus at the lateral process and at the umbo; in between these two points, the plica mallearis, a flimsy fold of mucosal tissue, tethers the tympanic membrane to the malleus. The anterior and posterior tympanic striae, running from the lateral malleal process to the anterior and posterior tympanic spines, respectively, separate the superiorly located pars flaccida (Shrapnell’s membrane) from the pars tensa. The pars tensa comprises three layers: a lateral epidermal layer, which is continuous with the skin of the external auditory canal; a medial mucosal layer, which is continuous with the mucosa of the middle ear; and an intermediate fibrous layer (the pars propria), consisting of outer radial and inner circular layers. The pars flaccida is also trilaminar and is thicker than the pars tensa, but contains an abundance of elastic fibers in its intermediate layer, which is irregularly organized.

Figure 1–8 Normal left tympanic membrane.
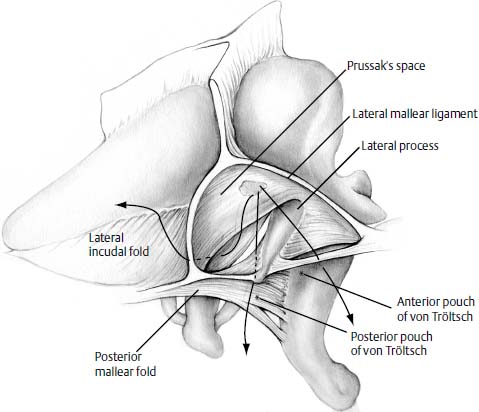
Figure 1–9 Prussak’s space and environs. (Adapted from Hughes G. Cholesteatoma and the middle ear cleft: review of pathogenesis. Am J Otol 1979;1:109–114. Reprinted by permission.)
Prussak’s space (Fig. 1–9), or the superior recess of the tympanic membrane, is bordered laterally by Shrapnell’s membrane, anterosuperiorly by the lateral malleal ligament, and inferiorly by the anterior and posterior malleal folds, and opens posteriorly into the epitympanum.
The fibrous annulus is the thickened periphery of the tympanic membrane and is lodged in the tympanic sulcus, both of which are deficient superiorly at the notch of Rivinus, where the tympanic membrane attaches directly to the squama.
Ossicles
The ossicular chain (Fig. 1–10) conveys sound from the tympanic membrane to the cochlea, and is made up of the malleus, incus, and stapes.
The malleus is the lateralmost ossicle, and consists of a manubrium (handle), head, neck, and lateral and anterior processes. The lateral process has a lateral, cartilaginous component that imperceptibly blends with, and thus is densely adherent to, the pars propria of the tympanic membrane. At the umbo, dense adherence is afforded by the splitting of the pars propria to encircle the tip of the manubrium. The anterior process to the petrotympanic fissure anchors the malleus, and, with the posterior incudal ligament, establishes the ossicular axis of rotation. The tendon of the tensor tympani muscle sweeps around the cochleariform process and attaches to the medial aspect of the neck and manubrium. Ordinarily, the medial pull of the tensor tympani muscle is opposed by the tympanic membrane; in cases of long-standing perforation, however, the tensor tympani acts unopposed, and can medially displace the manubrium, rendering myringoplasty and ossiculoplasty more difficult by contracting the middle ear space. Forcible lateralization of the malleus, or sectioning of the tendon, may be required to perform these procedures.
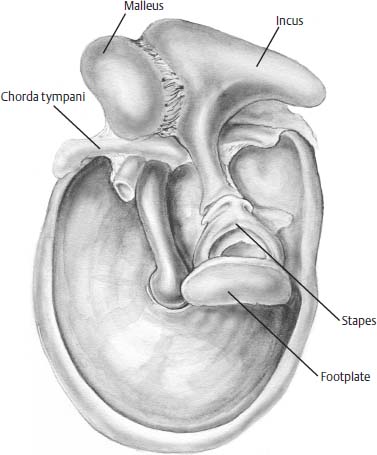
Figure 1–10 The ossicles, medial view in relation to the tympanic membrane.
The incus is the largest of the ossicles and comprises a body and a short, a long, and a lenticular process. The body rests in the epitympanum with the head of the malleus, with which it articulates in a cog-type fashion. The short process of the incus occupies the incudal fossa, anchored by the posterior incudal ligament. The long process stretches inferiorly, paralleling the manubrium, to which it lies posterior, and terminates in the lenticular process, which articulates with the stapes. The long process in particular is susceptible to osteitic resorption with chronic otitis media, possibly related to its tenuous blood supply.
The medially located stapes is the smallest of the ossicles and is made up of a head, footplate, and two crura. The footplate, rimmed by the annular ligament, seals the oval window. The stapedius tendon stretches anteriorly from the pyramidal process to attach to the superior aspect of the posterior crus and the head of the stapes. When dissecting disease from the stapes, for example, cholesteatoma, it is best to work parallel to the plane of the stapedius tendon, working from posterior to anterior, so that the tendon resists displacement of the stapes.
Muscles
The tensor tympani muscle, arising from the greater wing of the sphenoid, the eustachian tube cartilage, and the walls of its semicanal, has both striated and nonstriated fibers that converge into a tendon. Innervation is derived from the trigeminal nerve.
The stapedius muscle occupies a vertical sulcus adjacent to the facial nerve, from which it derives its innervation, in the posterior wall of the tympanic cavity. Its action tilts the stapes, stretching the annular ligament and diminishing response to sound stimulation.
Middle Ear Spaces
The tympanic cavity is a sagittally oriented slit that is pneumatized by the eustachian tube, traversed by the ossicular chain, lined by mucosa, and connected posteriorly to the mastoid air cells by the antrum and aditus ad antrum. Its tegmen, or roof, serves also as the floor of the middle cranial fossa, whereas its irregularly contoured floor is dominated by the jugular bulb; in the posterior part of the floor is the root of the styloid process, from which arises the styloid eminence. Anteriorly, progressing sequentially from inferiorly, are located the internal carotid artery, the eustachian tube orifice, and the tensor tympani muscle. The tympanic membrane forms the lateral wall.
The more anatomically interesting aspects of the tympanic cavity are its posterior and medial walls. The posterior wall features the pyramidal eminence associated with the stapedius tendon, and laterally, the chordal eminence, which is pierced by a foramen, the iter chorda posterius, traversed by the chorda tympani nerve as it enters the tympanic cavity. In between the pyramidal and chordal eminences is the facial recess, limited superiorly by the short process of the incus. Superior to the incus, the epitympanum opens into the mastoid antrum.
The medial wall (Fig. 1–11) is marked by three depressions of note: the sinus tympani and the oval and round window niches. The sinus tympani is delimited superiorly by the ponticulus, running between the pyramidal eminence and the promontory, inferiorly by the subiculum, which extends from the styloid eminence to the round window niche, laterally by the vertical segment of the facial nerve, and medially by the posterior semicircular canal. The sinus tympani variably extends posteriorly, but never communicates directly with the mastoid cavity, owing to different embryonic routes of pneumatization. The round window niche rests anteroinferior to the subiculum and posteroinferior to the promontory overlying the basal turn of the cochlea; the round window membrane lies in the depths of the niche; generally in the horizontal plane. The round window membrane, frequently obscured by a mucous membrane veil, has been implicated as a site of perilymph leakage; in making such as assessment, it is important to be sure that one is not being fooled by a leak through the veil. The oval window niche lies anterosuperior to the ponticulus. The cochleariform process is anterosuperior to the oval window, and is surmounted by the facial nerve in its tympanic segment.
The anterior epitympanic recess is anterior to the head of the malleus, which blocks the surgeon’s view of this space, and demonstrates considerable variability in size. Cholesteatoma may extend into this region from the epitympanum, and it is important to remember that the facial nerve and geniculate ganglion may lie dehiscent in the surgical floor (medial wall) of the epitympanum.
Eustachian Tube
The eustachian tube is the mucosally lined pathway that ventilates, clears, and protects the tympanic cavity as it extends from the nasopharynx. The fibrocartilaginous portion is located anteromedially and composes two thirds of the approximately 35-mm tube; its union with the posterolateral osseous segment is marked by the isthmus (Fig. 1–12). The bony eustachian tube lies lateral to the internal carotid artery and is perforated by the passage of the caroticotympanic arteries. The tympanic ostium of the tube is in the anterior wall of the tympanic cavity, a few millimeters above the floor.
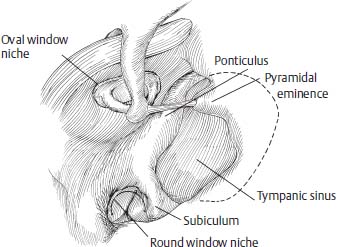
Figure 1–11 The medial wall of the left tympanic cavity, highlighting the sinus tympani, the round window niche, and the oval window niche. (Adapted from Schuknecht HF, Gulya AJ. Anatomy of the Temporal Bone with Surgical Implications. Philadelphia: Lea & Febiger, 1986:88. Reprinted by permission.)
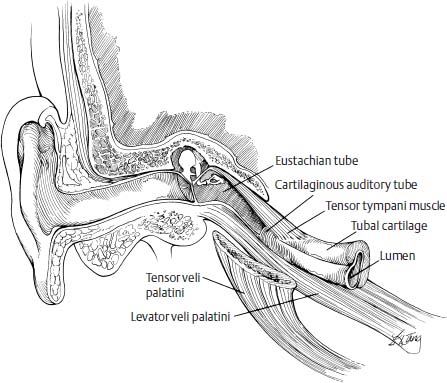
Figure 1–12 The eustachian tube and its associated muscles. (Adapted from Bluestone CD, Stool CE, eds. Pediatric Otolaryngology. Philadelphia: WB Saunders, 1990:320. Reprinted with permission.)
The fibrocartilaginous eustachian tube (Fig. 1–13) has a shepherd’s crook cross section, with a larger medial and a smaller lateral lamella; the inferior margin of the medial lamella has a groove for the levator palatini muscle, whereas the tensor veli palatini muscle attaches to the tip of the lateral lamella. Active opening of the upper half of the tube, which ventilates the tympanic cavity, is accomplished by contraction of the tensor veli palatini muscle.2 The mucociliary clearance function is located in the lower half of the tube, which has an abundance of mucociliary cells. The lateral fat pad (of Ostmann) contributes to the resting closure of the tube, which protects the tympanic cavity.2
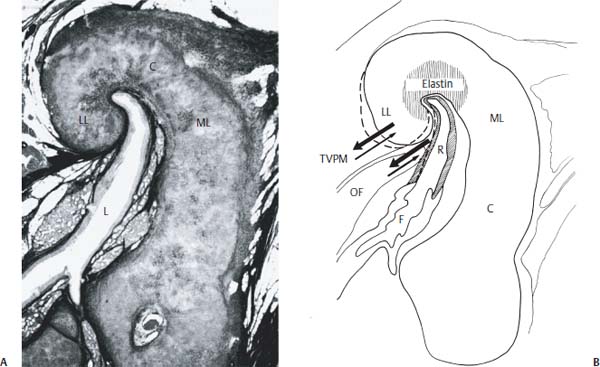
Figure 1–13 (A) Vertical section through the fibrocartilaginous (C) eustachian tube of an adult, illustrating the medial lamella (ML), the lateral lamella (LL), and their relation to the lumen (L). (B) Line drawing of fibrocartilaginous (C) eustachian tube, illustrating the hypothesized functional area. Tensor veli palatini muscle (TVPM) contraction causes lateral movement (heavy arrows) of the lateral lamella (LL) with respect to the medial lamella (ML) from its resting position (heavy outline) to its new position (dashed line). The elastin in the hinge portion mediates a return to resting position (thin arrows). (R, roof; F, floor; OF, lateral fat pad of Ostmann).
Middle Ear Mucosa
The tympanomastoid compartment has four types of lining cells: nonciliated with secretory granules, ciliated, intermediate, and basal.3 The distribution of cell types varies within the middle ear and mastoid, with ciliated cells found in conjunction with secretory cells,4,5 resulting in the formation of mucociliary tracts located on the promontory, the hypotympanum, and the epitympanum. These tracts work with the mucociliary clearance system of the eustachian tube.
Pneumatization
The degree of pneumatization of the temporal bone displays considerable variability, related to heredity, environment, nutrition, infection, and eustachian tube function. The pneumatized regions of the temporal bone are divided into five regions: the middle ear, the mastoid, the perilabyrinthine, the petrous apex, and the accessory (Fig. 1–14). Defined by the tympanic annulus, the tympanic region is divided into the mesotympanic, epitympanic, hypotympanic, protympanic, and posterior tympanic areas. The mastoid region can be divided into the mastoid antrum area, the central mastoid tract, and peripheral mastoid areas, for example, the tip cells. The perilabyrinthine region consists of a supra- and infralabyrinthine area, based on relation to the bony labyrinth. The petrous apex region is divided into an apical area and a peritubal area; the anterior petrous apex is pneumatized in 10 to 15% of specimens6; more often (80% of the time), the petrous apex is diploic, and in 7% of the cases it is sclerotic.7 The accessory region is made up of the zygomatic, squamous, occipital, and styloid areas. Five tracts of pneumatization are recognized: the posterosuperior, running at the juncture of the posterior and middle fossa plates of the temporal bone; the posteromedial, paralleling and running inferior to the posterosuperior tract; the subarcuate, running through the arch of the superior semicircular canal; the perilabyrinthine tracts, running superior and inferior to the bony labyrinth; and the peritubal, around the eustachian tube.
Inner Ear
The bony labyrinth shelters the sensorineural and membranous structures of the inner ear, and comprises the vestibule, the semicircular canals, and the cochlea. The bone is trilaminar, with an inner, or endosteal, layer, an outer, or periosteal layer, and in between, a mixed layer of intrachondrial and endochondral bone, characterized by globuli interossei or islands of cartilage. Both the middle and endosteal layers demonstrate poor reparative capacities, and thus fractures of the labyrinth tend to heal only by the formation of fibrous tissue, with some bony repair by the periosteal layer.
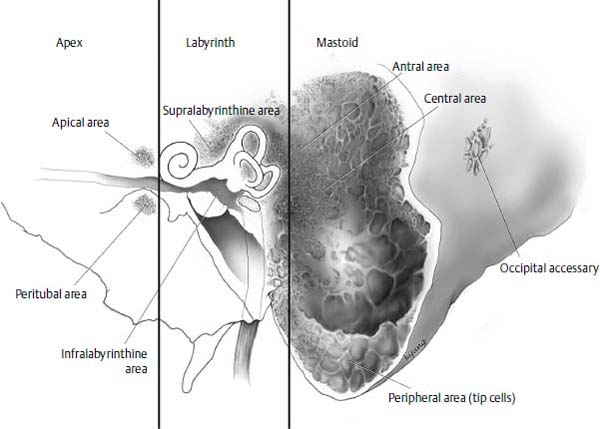
Figure 1–14 Pneumatization of the temporal bone. The mastoid, perilabyrinthine, and petrous apex regions are illustrated here. (From Nadol JB, Jr, Schuknecht HF, eds. Surgery of the Ear and Temporal Bone. New York: Raven Press, 1993. Reprinted by permission.)
The cochlea is a 32-mm bony spiral that winds 2½ turns about its central axis, the modiolus, to a total height of 5 mm. The base of the cochlea abuts the fundus of the internal auditory canal, and is perforated (the cribrose area) for the transmission of cochlear nerve fibers. The apex, pointing anteriorly, inferiorly, and laterally, lies medial to the tensor tympani muscle. The osseous spiral lamina also winds about the modiolus, partially subdividing the cochlear canal into the scala tympani and scala vestibuli. The interscalar septum separates cochlear turns.
There are three semicircular canals: the lateral (horizontal), posterior (posterior vertical), and superior (anterior vertical). The three canals are orthogonally related to one another, measure 1 mm in diameter (expanding to 2 mm at the ampullae), and describe a 240-degree arc. Each of the three ampullae opens into the vestibule, as does the nonampullated end of the lateral canal, but the nonampullated ends of the posterior and superior canals fuse to form the crus commune, and thus open into the vestibule.
Microfissures of the bony labyrinth, or breaks in the endosteal and endochondral layers filled with fibrous tissue and acellular matrix, are commonly encountered in two locations—between the round window niche and the posterior semicircular canal ampulla, and superior and inferior to the oval window. The round window niche microfissure is uniformly present after the age of 6 years, whereas the oval-window-related microfissures are seen in about 25% of specimens, especially after the age of 40 years.8 Their etiology remains unclear, but it is unlikely that they permit the flow of perilymph from the inner ear to the tympanic cavity.9
There are three fissures related to the bony labyrinth. The fistula ante fenestram is a constantly occurring evagination of the perilymphatic space that extends from the vestibule anterosuperiorly to the oval window, and in adulthood is filled with fibrous tissue and cartilage. The fossula post fenestram is a less consistently occurring evagination of the perilymphatic labyrinth that extends posterior to the oval window; it too is occupied by fibrous tissue. Hyrtl’s fissure (the tympanomeningeal hiatus) is a remnant of the embryologic development of the temporal bone and its course parallels that of the cochlear aqueduct from the medial aspect of the jugular fossa to inferior to the round window niche. It has been implicated as a site for cerebrospinal fluid leakage into the middle ear.10
The membranous labyrinth (Fig. 1–15), consisting of the cochlear duct, the three semicircular ducts and their ampullae, the otolithic organs (the utricle and the saccule), and the endolymphatic duct and sac, is housed within the bony labyrinth, with the connective tissue, blood vessels, and fluid of the perilymphatic space interposed. The membranous labyrinth is filled with endolymph, with the utricular duct, saccular duct, and ductus reuniens connecting the major structures.
The cochlear duct (Fig. 1–16), or scala media, is an epithelial duct that spirals from the vestibular cecum in the vestibule to the cupular cecum at the apex of the bony cochlea. The epithelium of the floor of the cochlear duct is dominated by the organ of Corti, which rests on the basilar membrane. The inner and outer hair cells are the primary auditory receptors; in the human, there is one row of inner hair cells and three rows of outer hair cells. The hair cells are partially enveloped by the synaptic terminations of cochlear nerve fibers and are associated with several types of supporting cells. The spiral ligament is a specialized layer of periosteum in the outer wall of the bony cochlea, upon which rests the stria vascularis, a band of specialized tissue that is composed of three layers of cells and a rich capillary network. Reissner’s membrane forms the anterior wall, or roof, of the cochlear duct, and extends from the spiral limbus to attach to the spiral ligament at the vestibular crest. The tectorial membrane is a gelatinous leaf that extends from the vestibular lip of the limbus to end in the border net, blanketing the organ of Corti.
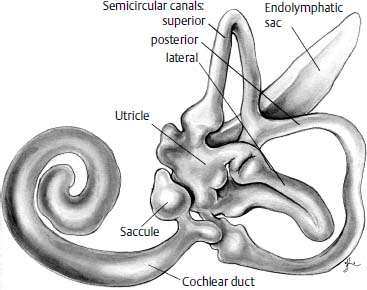
Figure 1–15 The adult membranous labyrinth as viewed from medially. (Adapted from Anson BJ, Donaldson JA. Surgical Anatomy of the Temporal Bone and Ear. Philadelphia: WB Saunders, 1983. Reprinted by permission.)
The utricle is an elliptical tube that sweeps inferiorly from the elliptical recess. Its macula, oriented in the horizontal plane, is the sense organ of the utricle, containing its hair cells, and is divided into two regions by the striola. The otolithic membrane is the otoconia-studded gelatinous blanket into which the cilia of the macular hair cells project.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


