4 Amplification A comprehensive audiometric evaluation is required prior to determining hearing aid candidacy. It is vital that, at a minimum, air- and bone-conduction audiometry, speech recognition thresholds (SRTs), and word recognition scores (WRSs) be obtained. In addition, tympanometry, acoustic reflex threshold testing, and/or acoustic reflex decay testing should be performed in patients with asymmetries in audiometric configuration and/or WRSs, conductive hearing loss components, or in patients with subjective reports of unilateral tinnitus, pain and/or pressure, and dizziness. It is important that the referring physician, or preferably an otologist, provide medical clearance for amplification prior to a trial period with hearing aids. The U.S. Food and Drug Administration (FDA; U.S. Food and Drug Administration, 2007) requires that medical clearance for amplification be obtained for all individuals under the age of 18. In addition, individuals over the age of 18 should either obtain medical clearance or sign a waiver acknowledging that they were informed of the recommendation for medical clearance, but elected to proceed with amplification without consulting a physician. It is especially important that patients with asymmetries in audiometric configuration and/or WRSs, conductive hearing loss components, complaints of unilateral symptoms of tinnitus, complaints of pain and/or pressure, and dizziness be evaluated by an otologist to determine whether further testing or some form of medical treatment is recommended. Once medical clearance has been obtained by the physician, it is safe to proceed with a hearing aid fitting (HAF). In addition, it is required that an audiometric evaluation be completed no more than 6 months before hearing aids can be dispensed. The hearing aid evaluation (HAE) is an appointment that occurs following the comprehensive evaluation and preferably after medical clearance for amplification has been received. The HAE is typically a 60-minute appointment that consists of reviewing the patient’s hearing test, determining patient motivation, and making recommendations for amplification based on a combination of the patient’s hearing loss characteristics, lifestyle, and financial resources. The HAE begins with a thorough description of the patient’s audiogram to determine hearing aid candidacy and to establish realistic expectations with hearing aids depending upon the patient’s hearing loss and ability to recognize speech. For example, a patient with mild to moderate sensorineural hearing loss from 2000 to 8000 Hz with excellent word recognition abilities is likely to have a better outcome with hearing aids than a patient with severe sensorineural hearing loss and a very poor ability to recognize speech. The use of a subjective questionnaire regarding a patient’s communication abilities without hearing aids is also recommended during the HAE. Such subjective questionnaires provide the audiologist and patient with a realistic picture of the patient’s functional communication abilities in everyday life with an unaided hearing loss and are also used after an HAF to confirm hearing aid benefit and/or satisfaction. Examples of commonly used patient questionnaires include the Abbreviated Profile of Hearing Aid Benefit (APHAB; Cox & Alexander, 1995), the Client Oriented Scale of Improvement (COSI; Dillon, James, & Ginis, 1997), and the Characteristics of Amplification Tool (COAT; Sandridge & Newman, 2006). Once hearing aid candidacy has been determined and the patient feels ready to proceed with hearing aids, hearing aid style (or size) and hearing aid technology are discussed at length. Depending on the style of hearing aid that the patient selects, an earmold impression is made of each ear canal to order a custom earmold (impression sent to earmold laboratory) for a behind-the-ear fitting or a custom in-the-ear hearing aid (impression sent to hearing aid manufacturer). Finally, the patient’s subjective loudness discomfort levels (LDLs) are often measured in the sound booth at the HAE, which is information that will be important at the HAF. LDLs, hearing aid style, technology options, and earmolds are discussed in detail in the following sections. A major complaint of hearing aid users is that their hearing aids are too loud. The measurement of a patient’s loudness discomfort levels (LDLS) provides audiologists with an output target in decibels in sound pressure level (dB SPL) for programming hearing aids to ensure the amplification to loud input levels is never judged to be uncomfortably loud. An LDL is defined as the level (decibels in hearing level [dB HL] and/or dB SPL) at which a patient reports that a signal (pure tone and/or speech) is “loud, but OK.” The measurement of LDLs is typically performed at the HAE appointment, but may also be performed immediately prior to the HAF. Figure 4.1 illustrates the configuration for measuring LDLs using an insert earphone. LDLs are measured from 500 to 4000 Hz in dB HL and SPL using a real ear approach, or one that involves the use of a probe microphone placed ~4 to 6 mm from the tympanic membrane. During LDL testing, the audiologist presents pure tones, beginning at ~20 dB SL (in reference to pure tone threshold at the test frequency), and uses an ascending procedure until the patient judges the pure tone signal to be “uncomfortably loud.” The audiologist then decreases the signal 10 dB, followed by incremental increases of 5 dB, and this bracketing technique is repeated until the level at which the patient judges the pure tone signal as “loud, but OK” is reliably determined. These levels are recorded as the measured LDLs both in dB HL, the level on the audiometer dial, and dB SPL, the level recorded at the probe microphone. Table 4.1 provides the categorical loudness scaling anchors that are provided to the patient during LDL testing. Fig. 4.1 Real ear configuration for measurement of loudness discomfort levels (LDLs) in dB HL and dB SPL using an insert earphone. The patient’s LDLs are used at the HAF to verify that the output of the hearing aid does not exceed the measured LDLs. This is confirmed by comparing the output of the hearing aid with a 90 dB SPL pure tone sweep, referred to as the real ear saturation response (RESR90), to the patient’s measured LDLs. This measurement will be discussed in further detail in the real ear measurements (REMs) section. Unfortunately, most audiologists too often use average transformations to predict LDL data to program hearing aids. The concern with using predicted LDLs is that intersubject variability of LDLs is as wide as 35 to 40 dB (Elberling, 1999), and as a result, the maximum output of the hearing aids may exceed a patient’s LDLs and the hearing aids are more likely to be rejected by the patient. Conversely, the maximum output (or ceiling) of a hearing aid may also be too far below the patient’s LDLs, which may result in increased distortion. For these reasons, it is important to not only measure individual LDLs, but to verify that the real ear maximum output of the hearing aids approximates the patient’s LDLs.
 What Type of Evaluation Is Required for Determining Hearing Aid Candidacy?
What Type of Evaluation Is Required for Determining Hearing Aid Candidacy?
 What Is the Role of the Otologist or Physician in Determining Hearing Aid Candidacy?
What Is the Role of the Otologist or Physician in Determining Hearing Aid Candidacy?
 What Is the Hearing Aid Evaluation?
What Is the Hearing Aid Evaluation?
 What Are Loudness Discomfort Levels and Why Are They Measured?
What Are Loudness Discomfort Levels and Why Are They Measured?

| 7. Uncomfortably loud |
| 6. Loud, but OK |
| 5. Comfortable, but slightly loud |
| 4. Comfortable |
| 3. Comfortable, but slightly soft |
| 2. Soft |
| 1. Very soft |
| 0. Cannot hear at all |
 What Are the Available Styles of Hearing Aids?
What Are the Available Styles of Hearing Aids?
Hearing aid style refers to the size or the physical appearance of a hearing aid, and can be divided into two basic categories: in-the-ear and behind-the-ear (Fig. 4.2). In-the-ear (ITE) hearing aids are custom made to each patient’s ear(s) and vary in size (largest to smallest) from traditional ITE, to in-the-canal (ITC) and completely-in-the-canal (CIC) instruments. With custom hearing aids, all of the electronic parts are housed in the custom hearing aid shell that sits in the ear canal and/or part of the concha bowl. Custom aids are typically easier to insert and remove and may have manual controls, such as a program button and volume control. However, because the electronic components of custom aids are located in a shell that is deeply inserted in the ear canal, these aids are subject to repair due to issues related to cerumen and moisture infiltration into the hearing aid. In addition, the amount of gain available in custom hearing aids is limited due to problems with feedback.
Behind-the-ear (BTE) hearing aids are non-custom and vary in the way that they are coupled to the ear and in the location of the receiver or loudspeaker. Conventional BTE aids are coupled to the ear via a custom earmold or a thin tube with a stock, one-size-fits-most dome. In addition, the loudspeaker (i.e., receiver) may be located in the hearing aid itself or it may be attached to a thin wire that is seated deeply in the ear canal. Generally, BTE aids are less likely than ITEs to need repairs that are the result of moisture and/or cerumen issues. In addition, BTE aids are usually able to accommodate a wider range of hearing losses (from slight loss to profound loss), are less prone to feedback-related problems, and have a longer battery life than ITE aids.
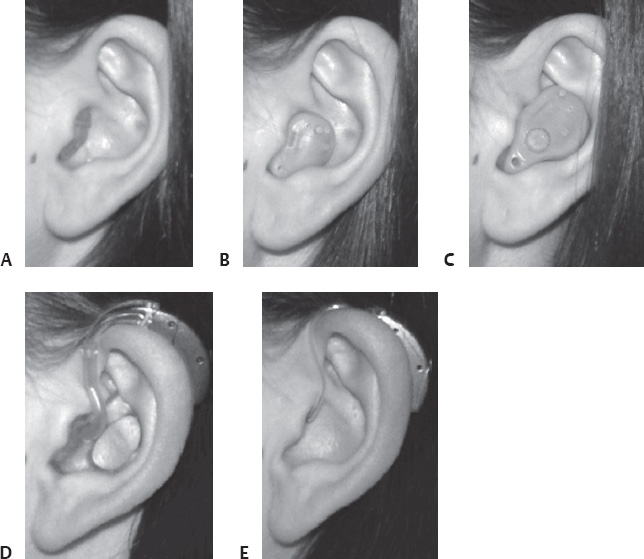
Fig. 4.2 Various styles of hearing aids: (A) completely in-the-canal (CIC), (B) in-the-canal (ITC)/half shell, (C) in-the-ear (ITE)/full shell, (D) behind-the-ear (BTE), and (E) open-fit BTE.
Open-fit hearing aids are BTE hearing aids that are coupled to the ear with a thin tube or wire and a non-occluding, or open, standard dome or custom earmold. This fitting option is most appropriate for patients with relatively normal hearing in the low frequencies (250–1000 Hz) and primarily high-frequency (> 1000 Hz) hearing loss; thus, low-frequency sounds enter and exit the open ear canal naturally, and amplification is provided only in the middle and/or high frequencies where it is required. When the open ear canal is completely blocked by an earmold or custom hearing aid, bone-conducted sound is amplified in the space occupying the ear canal from the tip of the earmold/hearing aid to the tympanic membrane by as much as 30 dB in the low frequencies (Revit, 1992). This phenomenon is known as the occlusion effect (OE), and results in the patient perceiving that they are talking into a barrel. Open-fit hearing aids help to minimize and oftentimes eliminate the OE. In general, two types of open-fit BTEs exist, receiver-in-the-aid (RITA) and receiver-in-the-ear (RITE). A RITA open-fit BTE (Fig. 4.3A) has all of the electrical components housed in the case behind the ear, and is coupled to the ear via an open tube and dome. A RITE open-fit BTE (Fig. 4.3B) has the microphones and processor located in the case behind the ear, but the receiver is located in the ear canal and is coupled to the ear via a thin receiver wire that is housed in a thin plastic tube. Much like custom hearing instruments, the RITE open-fit BTE is much more likely to require repair due to cerumen and/or moisture infiltration into the receiver than the RITA open-fit BTE.

Fig. 4.3 (A) Receiver-in-the-aid (RITA) versus (B) receiver-in-the-ear (RITE) open-fit BTE aids. (Photos courtesy of Phonak. From: Phonak Hearing Systems (2009). Image resources. Retrieved April 20, 2009 from http://www.phonakpro.com/_marketingservices/mktserv_imageresources_digitalbionics.html)
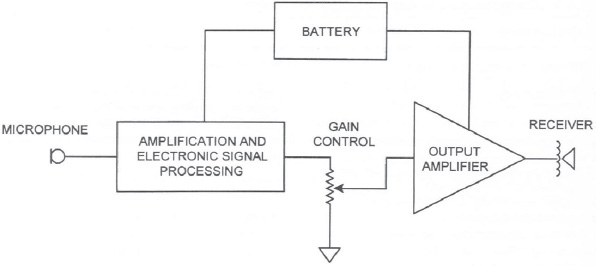
Fig. 4.4 Block diagram depicting the basic sound processing in a hearing aid. (From: Agnew, J. (2002). Amplifiers and circuit algorithms for contemporary hearing aids. In M. Valente (Ed.). Hearing aids: Standards, options, and limitations. 2nd ed. (pp. 101-142). New York: Thieme Medical Publishers, Inc.)
 What Is the Basic Sound Processing of a Hearing Aid?
What Is the Basic Sound Processing of a Hearing Aid?
Modern hearing aids consist of some of the most advanced digital signal processing available; however, the basic sound processing of a hearing aid remains the same today as it did in the past. All hearing aids, analog or digital, consist of a few basic parts that allow for sound processing to occur: a microphone (or microphones), an amplifier, and a receiver (or loudspeaker). The microphone converts acoustic energy to electric energy, the amplifier amplifies the electronic signal, and the receiver converts the electric signal back to an acoustic signal. In a digital hearing aid, sound is picked up by one or more microphones and the sound signal is filtered through an analog-to-digital (A/D) converter. From there, the binary code is sent through an amplifier, where multiple stages of sound processing occur, and through a digital-to-analog (D/A) converter. Finally, the amplified sound is delivered to the patient’s ear canal via the receiver or speaker. Figure 4.4 depicts the basic sound processing discussed above. The advanced sound processing that occurs in the amplification stage, including noise reduction and feedback management, is discussed in the sections below.
 What Are Directional Microphones and How Do They Work?
What Are Directional Microphones and How Do They Work?
The greatest complaint of patients with hearing loss is an increased difficulty understanding speech in the presence of background noise. Oftentimes, patients report they do well in quiet listening situations, but cannot understand speech when noise is present. Also, in the past, and to some degree at present, patients with hearing aids report they do well with their hearing aids in quiet, but not nearly as well in noise. Hearing aids with two or more microphones help to address patient complaints of difficulty in background noise by reducing the level of noise behind and/or to the sides of the listener, thereby providing the greatest amplification for sounds in front of the speaker. In this way, the hearing aid attempts to make speech more audible in the presence of background noise. Such a system, referred to as a directional microphone, enhances the signal-to-noise ratio (SNR). When a hearing aid is only equipped with one microphone or when only the front microphone of a directional microphone system is activated (referred to as omnidirectional) then the microphone is equally sensitive to sounds all around the listener.
Directional microphones have different polar patterns that determine the degree of azimuth at which the hearing aid provides the greatest (node) and least (null) amount of amplification. Figure 4.5 illustrates a variety of polar patterns, including cardioid, bidirectional, hypercardioid, and supercardioid. For example, a directional microphone system with a bidirectional polar pattern (Fig. 4.5B) would provide greatest amplification to the front and back of the listener, with very little amplification provided for sounds directly to the sides of the listener (at 90° and 270° azimuth).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


