Amblyopia
Evelyn A. Paysse
David K. Coats
Timothy P. Lindquist
THE TERM “AMBLYOPIA,” derived from Greek, literally means “dullness of vision.” Dr. Gunter von Noorden defined amblyopia as a “decrease of visual acuity in one eye when caused by abnormal binocular interaction or occurring in one or both eyes as a result of patterned vision deprivation during immaturity, for which no cause can be detected during the physical examination of the eye(s) and which in appropriate cases is reversible by therapeutic measures” (1).
Ophthalmologic examination of the eye typically reveals no anatomic abnormality. The exact mechanism of vision loss is not known, but it is thought to originate in the visual cortex. Amblyopia results in reduced visual acuity, fusion and stereopsis, and contrast sensitivity.
VISUAL DEVELOPMENT
At birth, the visual system is immature and visual acuity is estimated to be approximately 20/400 (2). Visual acuity improves and stereopsis develops during the first months of life. Myelination of the optic nerves, development of the visual cortex, and growth of the lateral geniculate body occur during the first two years (2). The fovea, the most visually sensitive part of the retina, reaches maturity at approximately 4 years of age. Visual stimuli are critical to the development of normal vision. Development of the visual pathways in the central nervous system requires that the brain receives a similarly clear, focused image from both eyes. Any process that significantly interferes with or inhibits development of the visual pathways in the brain may result in amblyopia.
The period of visual maturation is the critical period during which the visual system is affected by external influences. Most of the maturation of the visual system is thought to occur during the first 3 years of life, although some plasticity remains between 3 and 8 years of age, or even longer to some degree. One author describes three critical periods in the development of visual acuity and amblyopia (3):
The period of development of visual acuity (from birth to 3 to 5 years of age)
The period during which deprivation may cause amblyopia (from birth to 7 or 8 years of age)
The period during which recovery from amblyopia can be achieved (from the time of deprivation to adolescence or possibly young adulthood)
Epidemiologic, Social, and Psychosocial Factors
The prevalence of amblyopia in the United States is estimated between 1% and 3% (4). Using a conservative prevalence estimate of 2%, there are approximately 6 million people with amblyopia living in the United States. Prevalence rates for amblyopia are higher in developing countries. The National Eye Institute has reported that amblyopia is the most common cause of unilateral vision loss in patients under the age of 70 years. Estimates of prevalence, however, are affected by the definition of reduced visual acuity and by the process of early screening and treatment in the population being studied (4,5). Prevalence is not affected by gender. In some series, the left eye was more commonly affected than the right, particularly in cases of anisometropic amblyopia.
The mean age at presentation of amblyopia varies depending on its cause (6). In a series of 961 children with amblyopia, the mean ages at presentation for anisometropic, strabismic, and mixed amblyopia were 5.6, 3.3, and 4.4 years, respectively (6). The upper age limit for the development of amblyopia in children who are exposed to an amblyopia-inducing condition (e.g., traumatic cataract) has been reported to be between 6 to 10 years (7). Individuals with amblyopia are at increased risk for loss of vision and blindness in the nonamblyopic eye (8). In one population-based study of 370 individuals with unilateral amblyopia, the projected lifetime risk of vision loss in the fellow eye was 1.2% (95% CI 1.1 to 1.4) (8). In 16% of patients, vision loss in the nonamblyopic eye was due to orbital or ocular trauma.
Detection and treatment of amblyopia is important for a variety of reasons. Psychosocial effects of amblyopia have been reported by amblyopic children and their parents. Self-image, work, school, and friendships were negatively impacted. Somatization, obsessive-compulsive behavior, interpersonal sensitivity, depression, and anxiety were found
to be higher in individuals with amblyopia (9). Vocational opportunities for amblyopic individuals may be limited by requirements for good vision in both eyes.
to be higher in individuals with amblyopia (9). Vocational opportunities for amblyopic individuals may be limited by requirements for good vision in both eyes.
Amblyopia treatment has been proved to have a positive impact in multiple arenas. Both patching and penalization are well tolerated and well perceived by parents of children undergoing therapy (10). Psychosocial effects are minimized by therapy. Additionally, amblyopia treatment has been shown to be highly cost-effective when evaluating dollars expended to gain a valued commodity (visual acuity) and that impact over the life span of the individual (11).
CLASSIFICATION OF AMBLYOPIA
A distinction must be made between functional (potentially reversible) amblyopia and organic (irreversible) amblyopia. Organic amblyopia is a term used to describe visual impairment due to obvious or nonobvious ocular pathology, commonly involving the retina or optic nerve. Examples include optic nerve hypoplasia, optic atrophy, and foveal hypoplasia. Organic amblyopia is not the focus of this chapter. Functional amblyopia occurs in an eye that is anatomically normal. Functional amblyopia can occur concurrently with organic amblyopia and will be discussed later in this chapter.
Amblyopia is most commonly characterized by the clinical associations that initiate the problem. Amblyopia can likewise be classified based upon the causal mechanism. Familiarity with both methods of classification is important for clinicians and can be useful in designing and implementing appropriate treatment strategies.
Clinical Classification
Strabismic Amblyopia
Strabismic amblyopia is one of the most common forms of amblyopia. It results from abnormal binocular interaction that occurs when the visual axes of fellow eyes are misaligned. This abnormal interaction causes the foveae of the two eyes to be presented with different images. Diplopia and visual confusion result. Visual confusion (simultaneous perception of the two different images from the foveae) and diplopia (doubling of perception of the object of regard) stimulate active inhibition of the retinostriate pathways of visual input originating in the fovea and peripheral retina of the deviating eye. The visual cortex then suppresses the image from the deviating eye. Long-term suppression during the sensitive period of visual development results in amblyopia.
Any type of strabismus can be associated with amblyopia. As many as 17% to 40% of children with idiopathic infantile esotropia develop amblyopia. Intermittent exotropia is associated with amblyopia in up to 15% of patients. Paresis and palsy of cranial nerves 3, 4, or 6 may or may not be associated with amblyopia depending upon severity of the defect and the child’s ability to maintain fusion by adopting an anomalous head posture.
Strabismus surgery does not treat the associated strabismic amblyopia. Strabismus surgery is usually, though not always, deferred until the amblyopia has been maximally treated, though the success rate of surgery for esotropia is reportedly unaltered by the presence of mild amblyopia (12).
Anisometropic Amblyopia
Anisometropia is the other common cause of amblyopia. Anisometropic amblyopia occurs with hyperopia, myopia, or astigmatism. As a general rule, anisometropic amblyopia occurs more frequently with anisohyperopia (13). This occurs because when viewing binocularly, the fovea of the more ametropic eye in a child with anisohyperopia never receives a clearly focused image than the more hyperopic eye. In mild to moderate anisomyopia, the more myopic eye can be used for near work and the less myopic eye can be used for distance work, providing an important measure of protection against the development of amblyopia. Weakley (13) studied refractive errors likely to produce amblyopia. He noted that as little as one diopter of anisohyperopia and 1.5 diopters of anisoastigmatism were sufficient to produce amblyopia.
Anisometropic amblyopia is typically detected later as the affected child lacks obvious external abnormalities of the eyes (e.g., cataracts, strabismus), and visual function appears normal because the child sees well with the fellow eye.
In a manner thought to be similar to strabismic amblyopia, there is active cortical inhibition of input from the fovea of one eye in a child with anisometropia. This inhibition occurs in order to eliminate sensory misperceptions caused by monocular defocus and aniseikonia.
Visual-Deprivation Amblyopia
Deprivation amblyopia is the least common and most serious form of amblyopia. Visual deprivation is caused by obstruction of the visual axis or severe distortion of the foveal image of one or both eyes. Congenital cataracts, ptosis, congenital corneal opacities, and vitreous hemorrhage can cause deprivation amblyopia. Even transient obstruction of the visual axis, such as that caused by a hyphema or eyelid edema in a very young child can produce visual-deprivation amblyopia. Visual-deprivation amblyopia can be unilateral or bilateral. Sensory strabismus often occurs in children with unilateral vision deprivation. Deprivation amblyopia can result in permanent visual impairment if its cause is not treated urgently in infancy.
Special Forms of Amblyopia
Isoametropic amblyopia is the term used to characterize amblyopia in both eyes due to bilateral uncorrected or improperly corrected high refractive errors. It is most common in children with severe hyperopia, typically greater
than 5 or 6 diopters, but can also occur with high astigmatism and high myopia.
than 5 or 6 diopters, but can also occur with high astigmatism and high myopia.
Occlusion amblyopia is an iatrogenic amblyopia caused by obstruction of the visual axis of a sound eye in amblyopia treatment. It is more likely to occur when full-time patching is used. Rapid development of occlusion amblyopia is a sign of continued visual system plasticity and is believed by many ophthalmologists to portend a good visual outcome for both eyes of such patients if detected and corrected promptly.
Idiopathic amblyopia is a diagnosis of exclusion and is typically diagnosed in retrospect when a child with a monocular reduction of visual acuity and no detectable cause responds with improved vision during a trial of treatment for amblyopia. Because of this occasional good visual response, amblyopia treatment is often attempted when visual acuity is reduced in children with no obvious explanation. Presumably, an amblyogenic process was present earlier in the child’s life that has since resolved. Detailed history-taking will often identify a history of strabismus or previous occlusion of the visual axis (e.g., prolonged eyelid edema caused by an insect bite or infection of the lids as a young child). Equalization of a previous anisometropic refractive error is another possible explanation cause, although history is unlikely to be helpful in this situation.
Mechanistic Classification
From a mechanistic viewpoint, there are two causes of amblyopia. These include form-vision deprivation and abnormal binocular interaction. Each can occur in isolation or concurrently. Form-vision deprivation refers to amblyopia caused by poor image quality being projected onto the fovea. The visual cortex is thus never allowed to develop the capacity to process a sharply focused image. Form-vision deprivation occurs from conditions that obstruct the visual axis such as cataract, vitreous hemorrhage, corneal opacity, or severe ptosis, but it can also be produced by severe anisometropic hyperopia. For example, a child with an uncorrected refractive error of +10.00 diopters in his right eye and +1.00 diopter in the fellow eye can develop form-vision deprivation in the right eye due to persistent pronounced image blur in the right eye.
Abnormal binocular interaction refers to the condition in which the image projected onto the fovea of each eye is dissimilar enough to preclude fusion, thus prompting suppression and ultimately amblyopia of the suppressed eye. While strabismus may be the most obvious cause of abnormal binocular interaction, unilateral media opacities and severe anisometropia may participate in this mechanism as well. For example, in a child with uncorrected unilateral high myopia, in addition to a blurred image, the size of the image projected onto the fovea of the myopic eye is distinctly different than that projected to the fovea of the contralateral eye, resulting in abnormal binocular interaction in addition to form-vision deprivation.
PATHOPHYSIOLOGY
The mechanism and pathogenesis of amblyopia is an area of vast interest, with hundreds of publications produced on the topic in the last four decades. A common question that remains to be answered fully is the exact location of the disturbance within the visual system that is responsible for ultimately producing amblyopia. Changes have been found in the lateral geniculate nucleus (LGN) and visual cortex. It has been shown that the amblyopic eye functions at its best in mesopic and scotopic conditions and at its worst under photopic conditions. Retinal receptive fields in amblyopic eyes have also been shown to be larger than normal (14). Lastly, contrast-sensitivity function measured at the foveal region in strabismic amblyopes is reduced and similar to contrast-sensitivity function measured from the peripheral retina of a normal eye (15).
While amblyopia is most often detected during visual acuity testing, reduction in visual acuity is not the only visual abnormality that is present in the amblyopic eye. The full range of abnormalities present in the amblyopic eye has probably yet to be identified. Known visual abnormalities include reduced contrast sensitivity, dark adaptation abnormalities, and visual field abnormalities. Even the “sound” eye has been shown to have abnormalities in patients with anisometropic amblyopia. Leguire (16) reported reduced contrast-sensitivity function in both the amblyopic and “sound” eye of amblyopic patients. Kandel (17) reported dark adaptation to be better in the nonamblyopic eye.
Some authors have proposed that most eyes with amblyopia actually have subtle, undiagnosed ocular pathology involving the optic nerves, such as mild optic nerve hypoplasia (18). Certainly, it is true that some children initially diagnosed with amblyopia are later found to have subtle eye pathology when cooperative enough in later life to undergo a more detailed examination. The possibility of occult optic nerve and/or retinal pathology should always be kept in mind during the management of children with amblyopia who are not responding to treatment as anticipated.
Amblyopia is associated with histologic and electrophysiologic abnormalities in the visual cortex. Hubel and Wiesel (19) pioneered methods of studying the effects of changing visual experience in kittens by suturing an eyelid closed. Similar results have been found in a primate model (20). In these and other experiments, amblyopia was produced by suturing the lids closed in one eye and by inducing experimental anisometropia in susceptible animals.
The layers of the LGN corresponding to input from the amblyopic eye have also been shown to be attenuated in monkeys with strabismic, anisometropic, and visual-deprivation amblyopia (Fig. 6.1). Cells from the LGN travel through the parietal or temporal lobes to the visual
cortex, located in the occipital lobes. Ocular dominance columns representing alternating input from the right and left eyes are present in all portions of the visual cortex that receive binocular input. Notable exceptions are the temporal crescents of retina in each eye and retina corresponding to the position of the optic nerve in the fellow eye, which contribute monocular input. Amblyopia is associated with a decrease in the number of binocularly driven cells in the striate cortex (20,21). In a monkey model with deprivation amblyopia, the ocular dominance columns associated with the amblyopic eye were shown to be markedly attenuated (Fig. 6.2). These cortical changes presumably become irreversible over time. Recently Demer and coworkers (22) demonstrated significant reduction in relative cortical blood flow and glucose metabolism during visual stimulation of the amblyopic eye during a positron emission tomography scan.
cortex, located in the occipital lobes. Ocular dominance columns representing alternating input from the right and left eyes are present in all portions of the visual cortex that receive binocular input. Notable exceptions are the temporal crescents of retina in each eye and retina corresponding to the position of the optic nerve in the fellow eye, which contribute monocular input. Amblyopia is associated with a decrease in the number of binocularly driven cells in the striate cortex (20,21). In a monkey model with deprivation amblyopia, the ocular dominance columns associated with the amblyopic eye were shown to be markedly attenuated (Fig. 6.2). These cortical changes presumably become irreversible over time. Recently Demer and coworkers (22) demonstrated significant reduction in relative cortical blood flow and glucose metabolism during visual stimulation of the amblyopic eye during a positron emission tomography scan.
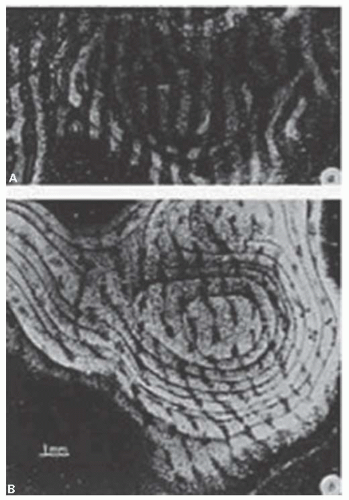 FIGURE 6.1. Autoradiographs of monkey visual cortex 2 weeks after injection of a radioactive tracer into the vitreous of one eye. Each figure represents a montage of tangential sections through the cortex. A: Normal monkey. The light stripes, representing labeled eye columns, are separated by gaps of the same width representing the other eye. B: Monocularly deprived monkey, who had the right eye closed at 2 weeks for 18 months. Input from the normal eye is in the form of expanded bands, which in places coalesce, obliterating the narrow gaps that represent the columns connected to the closed eye (21). (Reprinted with permission from Amblyopia, in Duane’s Ophthalmology.) |
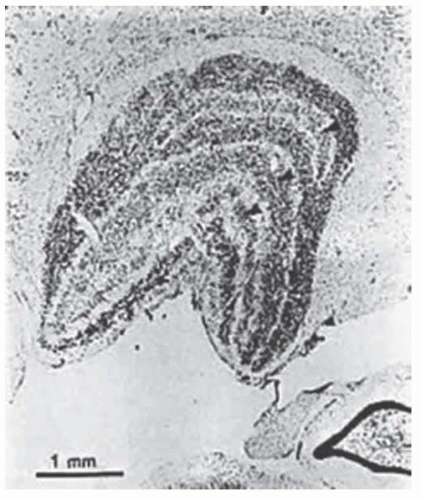 FIGURE 6.2. Coronal section through the right lateral geniculate nucleus of the same monkey. Atrophy in the layers receiving input from the deprived eye is indicated by arrows
Get Clinical Tree app for offline access
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|