Alignment
Marshall M. Parks
Christopher J. Kelly
Paul R. Mitchell
Ophthalmologists must have a thorough understanding of eye alignment, not only for the management of eye conditions, but also for the overall health of a patient, which may depend on an accurate assessment. Diagnosing a small-angle esotropia in a child is essential in treating the amblyopia often associated with that condition. The appreciation of lateral incomitance in a small-angle esotropia, an association that can mark a subtle sixth nerve palsy, may be the earliest sign of an intracranial mass. Excellent patient care requires that an ophthalmologist be familiar with the concepts of ocular alignment and possess the ability to accurately quantify eye deviations.
PRIMARY POSITION
Classification
Orthophoria: The eyes are perfectly aligned, and no deviation occurs, even when the fusion reflex is disrupted.
Heterophoria and Heterotropia: Misalignment compensated for by the fusion reflex keeps the deviation in heterophoria latent. Manifest misalignment is heterotropia.
Horizontal
Esophoria or esotropia: convergent deviation of the visual axes
Exophoria or exotropia: divergent deviation of the visual axes
Vertical
Right hyperphoria or hypertropia: right visual axis is deviated upward compared to the left
Left hyperphoria or hypertropia: left visual axis is deviated upward compared to the right
Torsional
Incyclophoria or incyclotropia: superior poles of the corneas are tipped medially
Excyclophoria or excyclotropia: superior poles of the corneas are tipped temporally
Determination
The methods used to determine the eye alignment in the primary position are varied and multiple. No single test invariably assesses the alignment accurately in all patients.
There are four basic types of alignment tests: the various cover tests, which depend on the fixation reflex; the corneal reflex tests, which are based on the ability of the curved corneal surface to reflect an examining light; the dissimilar image tests, which are based on the patient’s response to diplopia produced by converting an isolated object of regard into different images on each retina; and the dissimilar target tests, which are based on the patient’s response to the dissimilar images created by each eye viewing a different target.
COVER TESTS
Because the cover tests are based on the fixation ability of the eye, fixation ability must first be assessed. Patients without fixation ability in each eye (eccentric fixation) are unable to have eye alignment checked by cover tests. Also, the patient’s accommodation must be controlled with an appropriate target. An accommodative target is a small target designed to control the patient’s accommodation if the patient’s response supplies clear vision; this target is required during the cover test. Advantages of cover testing include a high degree of interobserver repeatability, easy quantification using prisms, and the ability to accurately measure the angle of deviation in all fields of gaze.
Cover–Uncover.
The patient’s right eye is covered while fixating a series of distant accommodative targets. After 2 to 3seconds, the right eye is uncovered and the left eye covered. When covering one eye, the examiner’s attention is directed to the opposite, uncovered eye, looking for movement of this eye. An absence of movement of an eye when the other eye is covered (Fig. 1), occurring in both eyes, means that the patient does not have a heterotropia, but it does not differentiate between orthophoria and heterophoria. The alternate cover test is required to make this differentiation.
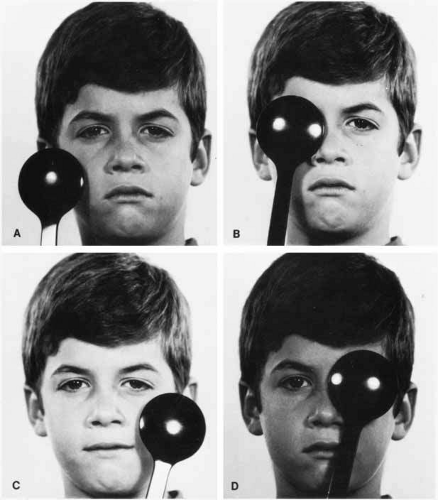 Fig. 1 Cover–uncover test. A. Examiner observes left eye while preparing to cover right eye. B. Right eye is covered. C. Right eye is uncovered. Right eye is observed as preparation is made to cover left eye. D. Left eye is covered. |
Alternate Cover.
The basic principle of this test is to prevent fusion for the duration of the test. This is accomplished by constantly maintaining a cover over one or the other eye, shifting it swiftly from eye to eye while the examiner looks for movement of the uncovered eye as it assumes fixation (Fig. 2). The rapid shift applies only to the speed of movement of the cover and not to the duration it is held before the eye; in fact, the exam-iner should maintain the cover over each eye for 2 or 3 seconds before rapidly shifting it. No movement of either eye indicates orthophoria. The patient whose eye moves on alternate cover has either a heterophoria or heterotropia. Differentiation between the two requires the cover–uncover test because there is not movement for either cover–uncover or alternate cover testing in orthophoria. The direction of the shift identifies the type of heterophoria or heterotropia. A temporal horizontal shift is esophoria or esotropia, a nasal shift is exophoria or exotropia, and right or left hyperphoria or hypertropia is the movement of the right or the left eye downward. If both eyes make movements downward, it is called dissociated vertical deviation or hypertropia (see Index).
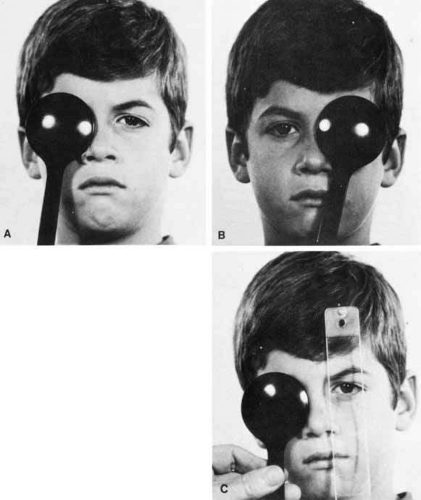 Fig. 2 Alternate cover test. Cover before right eye (A) is rapidly transferred to left eye (B) as examiner observes right eye for any shift it may make to establish fixation. Alternately transferring the cover from eye to eye while observing the uncovered eye discloses any heterodeviation that may be present, provided each eye can centrally fixate. C. Introducing a prism before one eye allows measurement of the heterodeviation (prism and alternate cover test). |
Having identified a heterodeviation, the next step is to measure the quantity of misalignment by neutralizing the shift with prism power. The prism is held in the examiner’s left hand in front of the patient’s right eye. The examiner’s right hand handles the alternate cover. The prism or prism powers are adjusted until the motion of the eyes on alternate cover is eliminated (Fig. 2C). Base-out prisms are used to compensate for an esodeviation, base-in for an exodeviation, base-down before the right eye for a right hyperdeviation, and base-up for a left hyperdeviation. Horizontal and vertical prism powers can be combined if loose prisms are used. A prism bar is handy, but it does not lend itself to neutralizing combined horizontal and vertical deviations nor is it sufficient to compensate for horizontal deviations greater than 45Δ or vertical deviations greater than 25Δ. The loose prisms must be combined for larger deviations. Vertical deviations seldom exceed 25Δ, but horizontal tropias greater than 40Δ are very common. The most convenient way for the examiner to hold combined horizontal prisms is not to superimpose them before one eye but instead to grasp the horizontal prisms either apex-to-apex (esotropia) or base-to-base (exotropia) between the thumb and index finger of the left hand, allowing the finger and thumb to cup around the patient’s right eye, with one prism being positioned before each eye. The area of contact between the apexes or bases then is in the midline in front of the patient’s nose. Prisms cannot neutralize cyclodeviations.
Prism measurement of the strabismic angle is the most accurate technique for measurement. However, prism measurements are subject to error. Thompson and Guyton1 describe several potential sources of error. The angle at which the prism is held in front of the patient can influence the quantification of a deviation, especially with large angles. Two commonly used positions are the Prentice, in which the prism is held perpendicular to the line of sight of the nonfixating eye, and the frontal plane position, in which the prism is held parallel to the plane of the patient’s face. In addition, the position of minimum deviation is reached when the angle of light incident to a prism is the same as that exiting. Glass prisms, although less common in clinical practice, are calibrated for the Prentice position, as are some prism bars2, whereas plastic prisms are calibrated for the angle of minimum deviation. It can be difficult to measure the angle of incident and exiting light from a prism, but in practice, the frontal plane position differs little from the angle of minimum deviation. However, holding a prism calibrated for the Prentice position in the position of minimum deviation can result in a significant overestimation of the deviation, especially for larger angles.
Strabismic angles larger than 50 prism diopters present another problem. It may be tempting to stack two prisms on top of one another and use their combined total to quantify the angle. However, this can seriously bias the result because the stacked prisms will not be held in the angle to which they are calibrated.1 Also, placing prisms in front of each other will not be correct, because angles measured in prism diopters are not additive. Fortunately, it is possible to stack horizontal and vertical prisms for complex strabismus, as the vectors are perpendicular to one another. Measurements at near are similarly subject to error.3 Because prism diopters are calculated as the distance light is bent over a distance of 1 meter, shortening the distance to a target by holding it too far from the eye can result in an overestimation of the true angle of deviation. More prism power is required to neutralize a near deviation if the prism is held several centimeters from the cornea.
Simultaneous Prism and Cover.
This test is useful in a patient having a small-angle heterotropia, commonly encountered in esotropes. The simultaneous prism and cover test is an attempt to measure the actual heterotropia angle present under normal seeing conditions while both eyes are uncovered. As the fixating eye is covered, a prism of known power is slipped simultaneously before the opposite eye with its base in the appropriate direction to compensate for the heterotropia. No movement occurs as the eye behind the prism takes up fixation when the prism power selected equals the heterotropia angle. This measurement is important because of a prevalent condition known as the monofixation syndrome.4 Some patients who have this syndrome are small-angle heterotropes; among these are some who reduce their larger fusion-free angle (as determined by alternate cover) to a smaller angle during normal seeing conditions. For example, the esotropia may measure 14Δ by alternate cover, but the simultaneous prism and cover may reveal 4Δ esotropia that the patient maintains with both eyes open.
CORNEAL REFLEX TESTS.
Studying the reflection of an examining light provides information regarding the alignment of the eyes in patients who cannot cooperate sufficiently to perform the alternate cover test or who lack fixation ability due to amblyopia. Four techniques may be employed using this principle. The Hirschberg test grossly estimates the angle of strabismus according to the degree of displacement away from the pupillary center at which the examiner views the corneal reflection in the deviated eye. Initially described by Hirschberg in the 19th century using a candle flame,5,6 currently a bright fixation light is placed before the eyes of the patient. The examiner observes the position of the light reflex in the nonfixating eye, as compared with the fixating eye. A second method was introduced by Krimsky7 as a more rigorous method of quantifying a deviated corneal light reflex. The Krimsky test entails introducing prisms before either one or both eyes to center the corneal reflections in the pupil of each eye. The third is a perimeter method, and the fourth is a major amblyoscope method. In the latter two methods, the alignment is read on the machine at the point the corneal reflections are centered in the pupils. The unit of strabismic deviation according to the Hirschberg and perimeter tests is degrees; for the Krimsky and major amblyoscope tests it is prism diopters.
Hirschberg Method.
A light reflected in the deviated eye nearer the pupillary center than the margin is estimated to be a 5° to 6° deviation, at the pupillary margin it is 12° to 15°, midway between pupillary margin and limbus it is 25°, at the limbus it is 45° to 60°, and beyond the limbus it is 60° to 80° (Fig. 3). Traditionally, each 1-mm deviation of light reflex displacement away from the proper position was considered to represent 7° or 15 prism diopters, without empirical validation.8 However, using flash photographs with millimeter rulers included for standardization, Brodie6 estimated a Hirschberg ratio of 21 prism diopters/mm, then supported this number theoretically. This angle correlates highly with that derived from alternate prism and cover testing.9
 Fig. 3 Hirschberg corneal reflex test.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|