Acute facial palsy is a common diagnostic problem encountered by the otolaryngologist, but its presentation often provokes consternation on the physician’s part. This reaction stems from our limited knowledge of facial nerve pathology, from the shortcomings of currently popular electrophysiologic tests in defining nerve injury, and from the controversy surrounding the management of facial palsy. This chapter presents contemporary opinions on management of acute facial palsy.
ANATOMY AND PHYSIOLOGY OF THE FACIAL NERVE
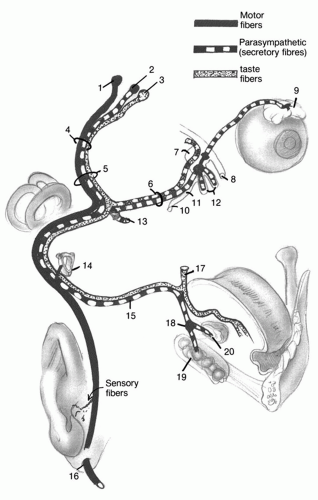
The cranial nerve VII is a complex motor/sensory nerve consisting of special visceral afferent, general visceral efferent, and special visceral efferent fibers (
Fig. 155.1) (
1). The special visceral afferent fibers convey the sense of taste from the sensory receptors on the anterior two-thirds of the tongue and project via the lingual and chorda tympani nerves to the geniculate ganglion and, hence, via the nervus intermedius to the tractus solitarius.
The general visceral efferent fibers constitute a parasympathetic system with three subsets of postsynaptic fibers. The preganglionic fibers arise in the superior salivatory nucleus. One subset of fibers exits the facial hiatus within the greater superficial petrosal nerve, joins the deep petrosal nerve in the vidian canal, and synapses at the sphenopalatine ganglion. Postsynaptic fibers then innervate the lacrimal and palatine glands. Another subset of preganglionic fibers within the lesser petrosal nerve synapses at the otic ganglion; the postsynaptic fibers provide secretory supply, in part, to the parotid gland. The third subset of this parasympathetic system exits the temporal bone along the chorda tympani nerve and passes along the lingual nerve to synapse at the submandibular ganglion. The postsynaptic fibers then provide the secretory supply to the submandibular and sublingual glands.
The special visceral efferent fibers arise within the facial motor nucleus and pass through the temporal bone, except for the fibers to the stapedius muscle, to exit the stylomastoid foramen and innervate the auricular, posterior belly of the digastric, stylohyoid, and platysma muscles and the superficial facial musculature.
Evidence that the sensory afferent fibers provide sensation from the external auditory canal and proprioception from the face is contradictory. These fibers are thought to account for the otalgia experienced in Bell palsy and the vesicular eruption in herpes zoster infection.
The intracranial segment of the facial nerve and the nervus intermedius exit the brainstem in a recess adjacent to the pons, cross the cerebellopontine angle ventral to the vestibuloacoustic nerve, and enter the internal auditory canal. The meatal segment of the facial nerve and the intermedius nerve occupy the anterior-superior quadrant within the canal and enter the fallopian canal at the meatal foramen superior to the crista transversa and anterior to the crista verticalis (Bill’s bar). The labyrinthine segment of the nerve courses 2 to 4 mm within the narrowest part of the fallopian canal to the geniculate ganglion, where the nerve makes an acute turn of 40 to 80 degrees (external or first genu) to enter the middle ear. Coursing posteriorly and slightly inferiorly above the cochleariform process and the oval window, the tympanic segment (11 mm) curves into the second (pyramidal) turn inferior to the horizontal semicircular canal. This turn has a more obtuse angle of 110 to 120 degrees. The mastoid segment then descends 13 mm vertically to the stylomastoid foramen. There are several branches of the nerve in its intratemporal course. At the geniculate ganglion, the greater superficial petrosal nerve courses anterior and medially. The branch to the stapedius muscle arises from the proximal mastoid segment while the chorda tympani exits the distal mastoid segment. The nerve to the posterior belly of the digastric is the first branch distal to the stylomastoid foramen. The
special visceral efferent fibers constituting the extracranial segment enter the posterior parotid gland and undergo secondary and tertiary branching. These fibers ultimately innervate the five regions of mimetic musculature: temporal, zygomatic, buccal, mandibular, and cervical. The peripheral branches of the nerve are the most variable in location.
Crossing nerve fibers at the level of the motor nucleus of the facial nerve in the brainstem leads to bihemispheric control of function in the upper half of the face and contralateral hemispheric control of function in the lower half of the face. Thus, forehead sparing can suggest a central versus a peripheral lesion of the facial motor pathway.
SURGICAL ANATOMY
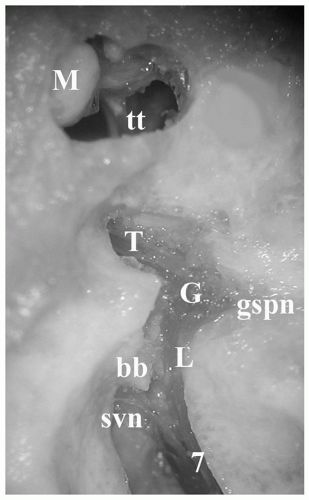
Knowledge of the intratemporal anatomy of the facial nerve and the associated landmarks is critical to safe otologic surgery. The surgical approach to different segments of the nerve varies if middle and inner ear structures are to be preserved. When hearing is good, the meatal and labyrinthine segments of the nerve are approached via the middle cranial fossa (
Fig. 155.2). This allows access to the internal auditory canal and/or geniculate ganglion. Important landmarks include the arcuate eminence, meatal plane, facial hiatus, and greater superficial petrosal nerve. The location of the internal auditory canal and meatal segment is approximated by bisection of the angle formed between the plane of the superior semicircular canal (arcuate eminence) and the greater superficial petrosal nerve. The nerve occupies the anterior quadrant of the internal auditory canal.
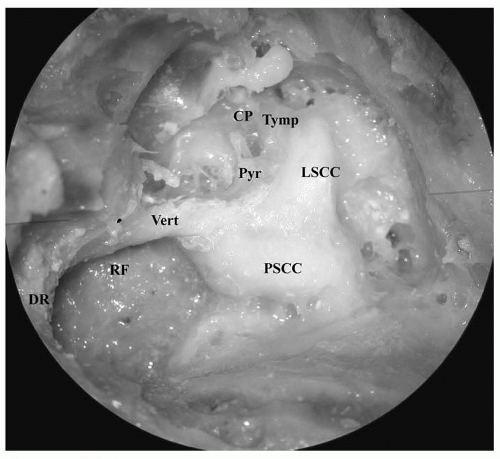
Important landmarks for identification of the tympanic segment in the middle ear are the cochleariform process and the oval window. The nerve is located superior to these structures and inferior to the horizontal semicircular canal. The upper mastoid segment lies posterior and medial to the chorda tympani and medial to the facial recess air cell tract. The stapedius muscle and posterior semicirular canal are medial to the facial nerve. The lower mastoid segment is at the same level as the digastric ridge (
Fig. 155.3), lateral to the retrofacial air cell tract. The mastoid segment of the nerve can be identified by removing the bone from the posterior aspect of the external auditory canal, thereby exposing the nerve on its lateral aspect. The surgeon should expect the nerve along a line drawn between the horizontal semicircular canal and digastric ridge.
When hearing preservation is not an issue, the entire intratemporal course of the nerve can be exposed via the translabyrinthine approach. The mastoid segment is defined as above. Removal of the labyrinth allows skeletonization of the tympanic segment along its superior aspect. The labyrinthine segment is located just anterior and superior to the ampulla of the superior canal. The internal auditory canal is identified medial to the vestibule. In the lateral end of the canal, the facial nerve is separated from the superior vestibular nerve by the vertical crest (Bill’s bar).
Anomalies of the Facial Nerve
Anomalies of the facial nerve are rare, but their existence makes even the most experienced otologic surgeon wary. The most common “anomaly” is a dehiscence in the facial canal, which exposes the nerve to injury during temporal bone surgery. The most common location is the tympanic segment over the oval window, followed by the geniculate ganglion and the mastoid segment adjacent to the retrofacial air cells (
2). The intratemporal course of the nerve is usually constant, but variations do occur. Deviations in the labyrinthine segment are exceedingly uncommon; usually the finding in this area is a difference in the angulation of the nerve between the meatal foramen and the geniculate ganglion, which relates to the depth of the internal auditory canal below the floor of the middle fossa. In the tympanic segment, the nerve may prolapse against the arch of the stapes, bifurcate around the stapes, or course below the oval window. Below the horizontal semicircular canal, the nerve may curve more acutely, making the prominent turn more susceptible to injury during an antrotomy. In the mastoid segment, bifurcations and trifurcations are exceedingly rare, but when duplication exists, the nerves occupy separate bony canals and exit individual foramina. Anomalies of the fallopian canal are suspect in congenital atresia of the middle ear and anomalies of the otic capsule (
3). Thin-section high-resolution computed tomography (CT) of the facial canal is recommended to provide as much preoperative information as possible about the course of the facial nerve.
Topographic Organization of the Facial Nerve
Topographic organization of the intracranial or intratemporal efferent and afferent fibers is not likely based on animal studies (
4,
5). Thus, suggestions that the site of lesion within the temporal bone can be determined according to the degree of muscle weakness in different regions of the face are inaccurate. This lack of intratemporal organization makes interfascicular repair of the nerve proximal to the stylomastoid foramen impractical and unnecessary. Synkinesis is inevitable with any reanastomosis or nerve grafting procedure.
Arterial Supply to the Facial Nerve
Both the carotid and vertebrobasilar arterial systems vascularize the intratemporal facial nerve. The labyrinthine artery, a branch of the anterior inferior cerebellar artery, provides the blood supply to the nerve within the internal auditory canal. The petrosal artery, a branch of the middle meningeal, supplies the nerve in the perigeniculate region and anastomoses with the stylomastoid artery, which feeds the mastoid and tympanic segments. The intratemporal facial nerve has a rich extrinsic anastomotic network to prevent ischemia, except in the labyrinthine segment at the junction between the carotid and vertebrobasilar systems.
EVALUATION
History
A careful history narrows the scope of the differential diagnosis and reduces the number of laboratory studies necessary to establish the cause. First, the onset of the paralysis
is defined as sudden, delayed, or gradual. Sudden refers to acute deterioration of facial function over a few days, either with or without an antecedent event. Delayed refers to acute deterioration in close temporal relationship with an antecedent event, though facial function is normal immediately following the event. Gradual refers to progressive loss over a period of weeks or longer. These definitions assume normal function prior to onset. When rapid deterioration occurs in a nerve exhibiting abnormal function, the onset is considered gradual or progressive unless there has been a lengthy period of stable facial function. Recurrent refers to facial palsy that occurs after a long period of stable recovery from a previous facial palsy.
Next, the degree of paralysis is designated as complete or incomplete. This is often of great prognostic importance. Incomplete paralysis or paresis is usually associated with good prognosis for recovery, unless a neoplasm is diagnosed. Complete paralysis typically carries a guarded prognosis for return of normal facial movement, especially when accompanied by electrical evidence of complete degeneration.
Associated symptoms provide additional diagnostic clues. Numbness in the middle and lower face, otalgia, hyperacusis, diminished tearing, and an alteration in taste are common in Bell palsy and Ramsay Hunt syndrome. Intense ear pain and a vesicular eruption are the hallmarks of herpes zoster oticus. Sensorineural hearing loss and vertigo are symptoms of advanced disease involving the labyrinth, the internal auditory canal, or brainstem.
Recurrent facial palsy also may indicate a tumor, although some persistent dysfunction is likely in between episodes of worsening function. More common causes of recurrent palsy include Bell palsy and Melkersson-Rosenthal syndrome. About 7% of patients with Bell palsy develop recurrent palsy, with half of the recurrences on the ipsilateral side (
6). Melkersson-Rosenthal syndrome is often familial, and the first episode of facial palsy usually occurs before 20 years (
7). Associated findings include facial edema, particularly of the upper lip; fissured tongue; and migraine headaches.
Any thorough history encompasses other medical conditions that may be incriminated in the differential diagnosis of the palsy: cancer, sarcoidosis, autoimmune disorders, and previous surgeries in the posterior fossa, temporal bone, or parotid.
Laboratory Studies
Several studies may be indicated in the evaluation of acute facial paralysis (
Table 155.1), depending on the findings in the history and physical examination. Because of numerous problems arising within the temporal bone and the proximity of the cranial nerves VII and VIII in the posterior fossa, pure tone and speech audiometry is recommended.
The once-popular topognostic testing (Schirmer test, stapedial reflex assessment, electrogustometry, and salivary flow) for determining the site of the lesion and for prognostication is obsolete. Imaging is more efficient for diagnosis and is essential in any case when the etiology is uncertain or the paralysis is recurrent or atypical. High-resolution CT of the temporal bone is the study of choice for assessment of the fallopian canal. Any potential cause of facial paralysis associated with bone destruction (mastoiditis, cholesteatoma, tumors, temporal bone trauma) is seen best on CT. MRI is most useful when infectious or neoplastic involvement of the nerve (idiopathic facial palsy, herpes zoster oticus, facial schwannoma) is suspected.
When paralysis is complete, electrophysiologic studies are done to establish the degree of degeneration and prognosis for recovery. The Schirmer test remains useful to quantitate the amount of tearing in the involved eye. Reduced tear secretion suggests the need for aggressive treatment to protect the cornea. When the diagnosis is uncertain, other laboratory studies can be considered to
exclude blood dyscrasias, autoimmune disorders, Lyme disease, sarcoidosis, and central nervous system diseases.
 DIFFERENTIAL DIAGNOSIS FACIAL PALSIES
DIFFERENTIAL DIAGNOSIS FACIAL PALSIES


