22 Acute and Chronic Nasal Disorders For acute and chronic disease also involving sinuses—see related chapters 24–26 • Invasion of pilosebaceous follicle by Staphylococcus aureus • Risk of cavernous sinus thrombosis—mortality of 10 to 27% • Acute β-haemolytic streptococcal infection • Follows a cut or incision • Butterfly pattern on face • Responds well to penicillin/erythromycin • Large deforming masses distending the nasal cavity • Klebsiella rhinoscleromatis • Disease found in developing countries • Three phases: rhinitic, infiltrative, and nodular • Finally resulting in adhesions, stenosis, and atresia • Large red tumour-like masses of the nodular phase are characterized by: • Large doses of streptomycin and tetracycline over 4 to 6 weeks are needed until two consecutive biopsies are negative • Topical acriflavine solution has also been used • Fingernail transmission into nose • Incubation can take 10 years • Tuberculous or lepromatous forms • Small anesthetic patches (tuberculoid) or nodular thickening around ant IT (lepromatous) • Perforation and nasal deformity follow • Dapsone ± rifampicin/clofazimine to treat • Nasal involvement secondary to chest • Nodular/ulcerative lesions on ant septum or ITs or choanae • Caseating epithelioid granulomas with acid-fast bacilli • Responds to standard Rx with saline douching • Lupus vulgaris = variant—nodules at vestibule • Congenital/primary/secondary/tertiary • Primary chancre on external nose or vestibule at 3–4 weeks after contact; disappears spontaneously after 6 to 10 weeks • Serology may be negative in early stages, 90% +ve in tertiary stage • Secondary stage may appear as simple rhinitis • Tertiary gummas produce tenderness over bridge of nose, posterior septal perforations, and nasal collapse • Congenital form may present at puberty: • Penicillin Rx required • An inflammatory disorder of the nasal mucosa characterized by 2 or more of the following symptoms: • Commonest immunological disorder in humans: 10 to 25% of individuals globally • Significant effects on quality of life for sufferers—may account for 30 to 40% of reduced productivity in the workplace • Most asthmatics also suffer from rhinitis • Allergic rhinitis and asthma share many common inflammatory processes • Both allergic and non-allergic rhinitis are risk factors for asthma • Most exacerbations of asthma are commenced by upper respiratory tract infection (URTI) • Rhinitis causes bronchial hyperreactivity • Allergic rhinitis increases the risk of asthma about threefold • Intermittent—<4 days/week or <4 weeks/year • Persistent—opposite of intermittent • Mild—normal sleep, daily activities, work/school; no troublesome symptoms • Moderate/severe—one or more of items not found in mild rhinitis • Allergen contact with IgE on mast cell surface • Mast cell degranulation releasing mediators and cytokines leads to initial symptoms of: • Leukotrienes, cytokines, and chemokines cause influx of inflammatory cells (eosinophils) • Cells secrete further mediators and cytokines • Inflammatory response perpetuated for days/weeks • Distinguish from other types of rhinitis or rhinosinusitis • Allergen contact—pets, damp home, etc. • Seasonal vs. perennial • Concurrent asthma • Paternal atopy (higher if both parents affected) • Drug history—e.g., use of nasal sprays, β-blockers • Endoscopic examination of nose • Skin prick allergy tests or radioallergosorbent test (RAST) • Other rhinological assessment: • Allergen avoidance • Topical steroids • Topical decongestants • Oral/(topical) antihistamines • Systemic steroids • Cromolyn sodium • Leukotriene receptor antagonists • Ipratropium bromide • Immunotherapy • Surgical turbinate options • Rhinitis is a common problem with significant socio-economic effects • A careful history and examination with skin prick test (SPT) can determine the appropriate level of medical management • Remember to manage the combined airway Also known as idiopathic or vasomotor rhinitis • Diagnosis of exclusion • Non-specific triggers: temperature, humidity, irritants (e.g., cigarette smoke)
22.1 Bacterial Infections
22.1.1 Folliculitis and Vestibulitis
22.1.2 Erysipelas
22.1.3 Rhinoscleroma
 Mikulicz cells (large cells with clear cytoplasm containing the bacilli)
Mikulicz cells (large cells with clear cytoplasm containing the bacilli)
 Russell bodies (which are plasma cells with eosinophilic-staining cytoplasm and prominent nuclei)
Russell bodies (which are plasma cells with eosinophilic-staining cytoplasm and prominent nuclei)
22.1.4 Leprosy
22.1.5 Tuberculosis
22.1.6 Syphilis
 Nasal saddling
Nasal saddling
 Dental abnormalities
Dental abnormalities
 SNHL
SNHL
22.2 Allergic Rhinitis
22.2.1 Definition of Rhinitis
 Rhinorrhea (anterior and/or posterior)
Rhinorrhea (anterior and/or posterior)
 Blockage
Blockage
 Itching/sneezing
Itching/sneezing
22.2.2 Facts about Rhinitis
22.2.3 Rhinitis and Asthma
22.2.4 Allergic Rhinitis Classification (ARIA)
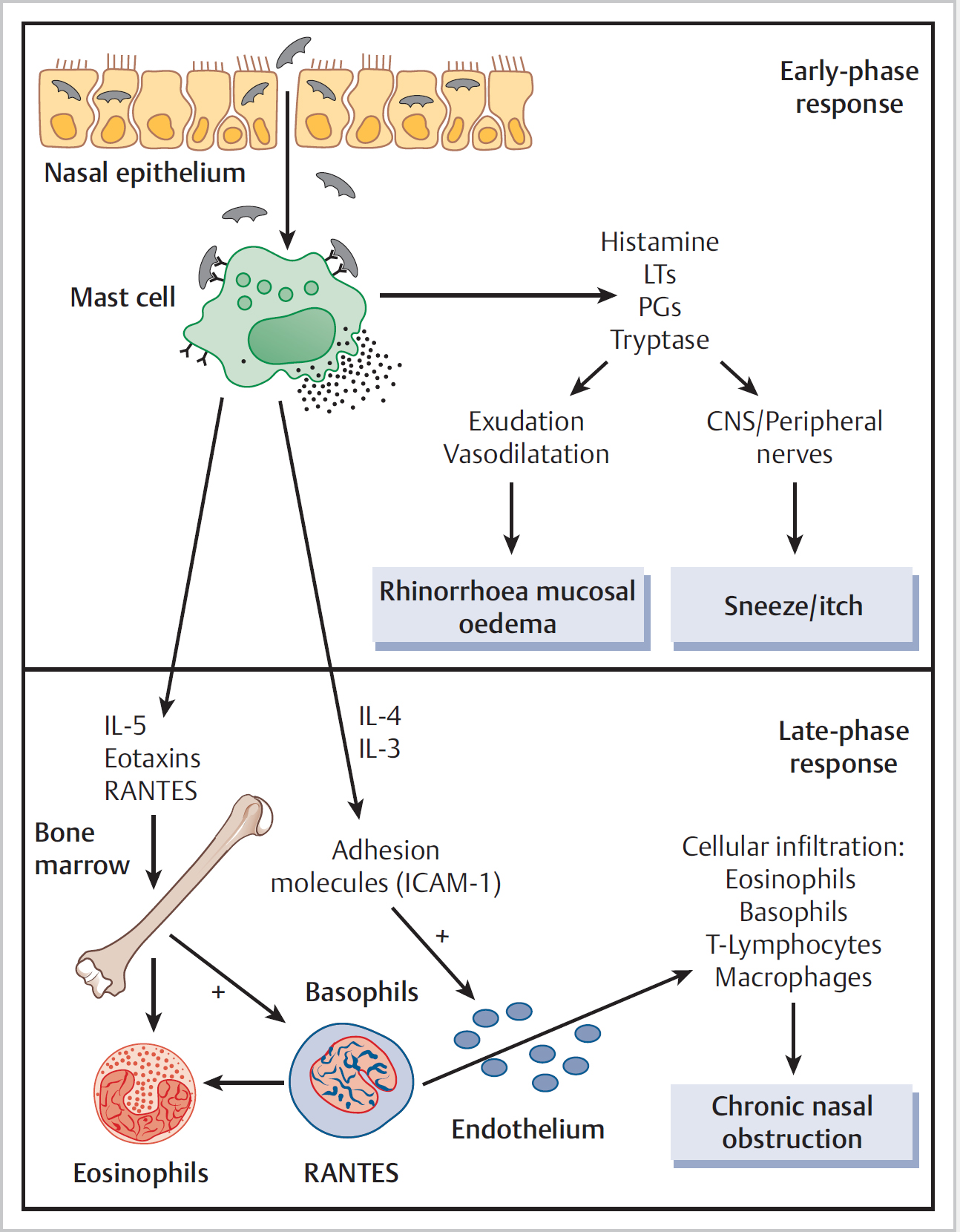
22.3 Pathophysiology of Rhinitis (Fig. 22.1)
22.3.1 Early Stage
 Sneezing
Sneezing
 Running
Running
 Itching
Itching
 Blockage after 15 to 20 min
Blockage after 15 to 20 min
22.3.2 Late Phase
22.3.3 History
22.3.4 Assessment of the Rhinitic Patient—Examination and Investigations
 Spatula misting
Spatula misting
 Peak inspiratory nasal flow rate
Peak inspiratory nasal flow rate
 Acoustic rhinometry
Acoustic rhinometry
 Rhinomanometry
Rhinomanometry
 Mucociliary clearance
Mucociliary clearance
22.3.5 Management Options (Fig. 22.2)
22.3.6 Summary
22.4 Non-allergic, Non-infectious Rhinitis
22.4.1 Non-allergic, Non-eosinophilic Rhinitis (NENAR)
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


