31 Acoustic Neuromas and Neurofibromatosis Type 2
Acoustic neuromas also known as vestibular schwannomas are the most common tumors of the cerebellopontine angle (CPA) constituting 80% of the tumors of the CPA, followed by meningiomas and epidermoid cysts.1,2 Clinically diagnosed acoustic neuromas occur in 0.7 to 1.0 people per 100,000 population.3 There have been studies that suggested the prevalence of incidental acoustic neuromas to be 2 in 10,000 people.4
They are benign tumors that arise from the Schwann cells surrounding the nerve. The cranial nerve sheaths are formed by oligodendrocytes proximally as they exit the brain parenchyma and transition to myelin forming Schwann cells within a few millimeters. The transition zone for the vestibulocochlear nerve is at the Obersteiner-Redlich zone near the porus acousticus.5 As sensory nerve fibers are more heavily myelinated than motor fibers, the tumors tend to occur more frequently in sensory nerves, with the inferior vestibular nerve accounting for the origin of up to 91% of the schwannomas and the superior vestibular nerve the remaining number.5
The tumors tend to occur in two forms, the sporadic form which accounts for up to 95% of tumors occurring unilaterally and the remaining 5% associated with neurofibromatosis type 2.6 This small group has a predilection for occurrence in younger patients (second to third decades of life) and also bilateral tumors and as such present a unique set of challenges for successful management particularly in reducing postoperative morbidity and hearing rehabilitation. Grossly, they are usually yellow, white, or gray in appearance, usually solid but sometimes cystic with a smooth and regular surface. Although they are described as having a well-defined capsule, often during excision there is little evidence of a true capsule. Histologically, two patterns are described, Antoni A and Antoni B.6 The Antoni A pattern exhibits a densely packed pattern with small, spindle-shaped, deeply stained nuclei with whorled formations termed Verocay bodies. An Antoni B pattern shows a looser more cellular aggregation with pleomorphic, vacuolated cells. Both patterns show confirmatory S-100 immunocytochemical staining.5
Acoustic neuromas tend to exhibit slow growth with the mean tumor growth rate thought to be ranging from 0.5 to 2.0 mm per year.2 As the tumor approaches 2 cm in size, it abuts upon the brainstem and further growth causes the classic symptoms of brainstem compression. When the tumor reaches a size of approximately 4 cm it often extends far anteriorly and compresses the trigeminal and abducent nerves. Infrequently, it can also extend inferiorly to the jugular foramen compressing the lower cranial nerves and very rarely compression of vessels may occur with venous or arterial infarctions.6,7
Etiology
Exposure to high-dose ionizing radiation is the only definite environmental risk factor associated with an increased risk of developing an acoustic neuroma. Neurofibromatosis type II (NF2) occurs in individuals who have defective tumor suppressor gene located on chromosome 22q12.2. The defective protein produced by the gene is called merlin or schwannomin.8
Presentation
Hearing Loss
Progressive high-frequency unilateral or asymmetric sensorineural hearing loss is the most common presenting symptom in almost 90% of cases. In 10% of cases, sudden hearing loss occurs.9 Progressive injury to cochlear fibers probably accounts for slow progressive neurosensory hearing loss observed in a significant number of patients with acoustic neuromas. Sudden and fluctuating hearing losses are more easily explained on the basis of disruption of cochlear blood supply.10
Hearing levels are assessed using both pure tone thresholds and speech discrimination scores. The American Academy of Otolaryngology-Head and Neck Surgery Hearing Classification System (Table 31.1) or the modified Sanna classification11 (Fig. 31.1) can be used to quantify the extent of the hearing loss which is particularly important for selecting a surgical approach.
Tinnitus, Dysequilibrium, and Facial Weakness
Tinnitus can be a presenting symptom in up to 70% of acoustic neuromas.12
Vertigo is an uncommon presenting symptom in approximately 20% of patients. Dysequilibrium or the sensation of floating or unsteadiness is seen in up to 48% of patients with acoustic neuromas and the incidence is proportional to the size of the tumor.13
The incidence of facial nerve dysfunction associated with acoustic neuromas is approximately 10%. At the time of diagnosis more than 90% of patients have a normal House Brackmann grade I facial function.14,15
Table 31.1 American Academy of Otolaryngology-Head and Neck Surgery Hearing Classification System
Class | Pure Tone Threshold | Speech Discrimination (%) |
A | ≤ 30 dB | ≥ 70 |
B | > 30 dB, ≤ 50 dB | ≥ 50 |
C | > 50 dB | ≥ 50 |
D | Any level | < 50 |
Source: Committee on Hearing and Equilibrium guidelines for the evaluation of hearing preservation in acoustic neuroma (vestibular schwannoma). Otolaryngology-Head and Neck Surgery 113:179–180, 1995.
Cerebellar Dysfunction, Lower Cranial Nerve, and Brainstem Symptoms and Hydrocephalus
Cerebellar symptoms are usually due to direct compressive effects of the tumor and are usually later manifestations of disease with larger tumors. Lower cranial nerve manifestations are usually seen only with large tumors extending to the jugular foramen and hypoglossal canal. Large tumors that obstruct the fourth ventricle often lead to symptoms related to hydrocephalus such as headaches, nausea, vomiting, and diplopia. The incidence of hydrocephalus is low at 4% and is usually associated with rapid growth of the tumor.12
Investigations
Radiological investigations are the mainstay of diagnosis of acoustic neuromas with gadolinium (gadolinium diethylenetriamine penta-acetic acid)-enhanced magnetic resonance imaging (MRI); the current gold standard of diagnosis.16 Audiological tests such as the auditory brainstem response (ABR) were useful before the advent of MRI with the amplitude, latency, and interval difference between wave I and wave V being the most reliable indicators.11,17,18
Acoustic neuromas appear as iso- to hypointense on T1-weighted images and hyperintense on T2-weighted images with intense enhancement on gadolinium contrast administration. Fat suppression techniques are also a useful tool especially for detecting postoperative recurrence particularly if abdominal fat is uitilized to obliterate the cavity as routinely practiced at our center. Axial and coronal views are the best at displaying the tumor and its relationship with the surrounding anatomy. The following parameters can be easily assessed with MRI19,20:
• Tumor size.
• Intrameatal tumors are grade 0 tumors with grade 1 onward according to the largest extrameatal diameter.
• It is classified into:
 Intracanalicular.
Intracanalicular.
 Grade 1: less than 1 cm in greatest diameter.
Grade 1: less than 1 cm in greatest diameter.
 Grade 2: between 1 cm and less than 2 cm.
Grade 2: between 1 cm and less than 2 cm.
 Grade 3: between 2 cm and less than 3 cm.
Grade 3: between 2 cm and less than 3 cm.
 Grade 4: between 3 cm and less than 4 cm.
Grade 4: between 3 cm and less than 4 cm.
 Grade 5: more than 4 cm.
Grade 5: more than 4 cm.
• Internal auditory canal involvement.
• Intratumoral cysts.
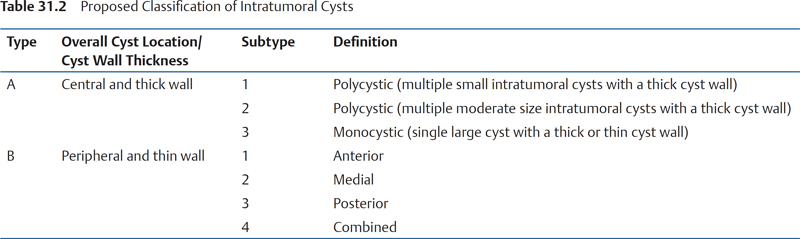
This may be particularly important when deciding upon total or subtotal tumor removal. A classification has been proposed (Table 31.2) according to the thickness of the cyst wall (thick or thin) and the location of the cyst within the tumor (central or peripheral). Subtype B1 and B3 pose the greatest danger to the facial nerve as the nerve is more stretched over the tumor (Fig. 31.2A, B):
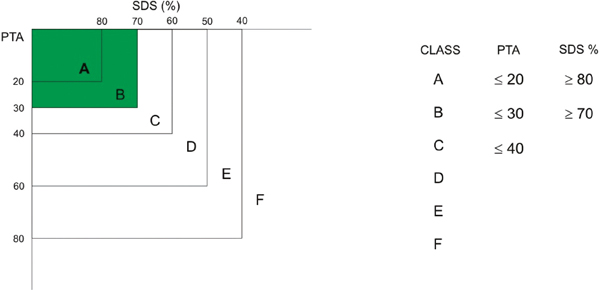
Figure 31.1 Modified Sanna classification. PTA, pure tone average; SDS, speech discrimination score.
Printed with permission from: Sanna M, Moffat DA, Kunihiro T, Inoue Y, eds. Acoustic Neuroma. Consensus on Systems for Reporting Results. Tokyo, Japan: Springer-Verlag; 2003:169–173.
• Extratumoral cysts.
• Intratumoral Hemorrhage.
• Brainstem indentation.
• Inner ear invasion.
While a translabyrinthine approach is well suited for invasion of the posterior labyrinth, the transotic approach offers better control of the cochlea turns. Neither the classic middle cranial fossa nor the retrosigmoid approach (RS) permits the removal of the infralabyrinthine portion of the tumor.3,21
• Brainstem compression.
• Cleavage plain between tumor and surrounding normal tissue.
• Jugular Bulb and sigmoid sinus, size, and dominance.
Computed Tomography Scan
Acoustic neuromas appear iso- to hypodense on nonenhanced computed tomography (CT) and enhance homogenously after an injection of contrast agent.1 In some occasions the tumor growth produces a progressive enlargement of the internal auditory canal, detected by the bone algorithm CT. However, CT is not ordered routinely because it is inferior to MRI in its resolution of soft tissue and can miss tumors till 1 cm into the CPA. Presently it is only indicated for patients that cannot undergo an MRI scan.
Decision-Making in Acoustic Neuroma Surgery
The factors influencing the decision-making process can be broadly classified as patient factors and surgeon factors.21–23
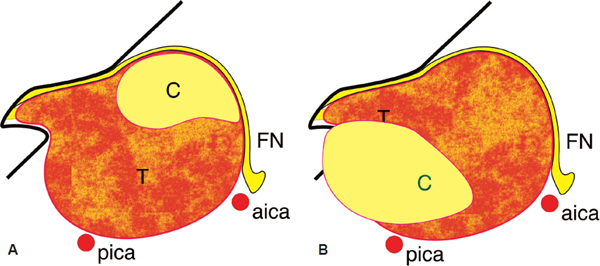
Figure 31.2 (A) Subtype B1. (B) Subtype B3. aica, anterior inferior cerebellar artery; c, cyst; FN, facial nerve; pica, posterior inferior cerebellar artery; T, tumor.
Patient Factors
• Tumor size.
• Extension.
• Age.
• Preoperative ipsilateral and contralateral hearing levels measured by pure tone audiogram, speech discrimination scores and occasionally ABR.
• Preoperative general condition and rehabilitation potential.
• Patient’s expectations.
Surgeon Factors
The surgeon should be familiar with all available approaches although the choice of approach is often dictated by the surgeon’s own experience and preference.
Residual Tumors
Residual tumors have the same features of the primary ones; depending on the experience of the surgeon and the difference encountered during surgery a different amount of tumor is left in place. While subtotal removal is adopted as a defined strategy in selected patients (usually elderly patients) sometime it results in an enlarged biopsy.
Wait and Scan
Some patients affected by small lesions are not candidate for surgery and may be initially followed with a “wait and scan” policy. However, not all these tumors do not grow and in such a case the policy may be switched for a surgery or a stereotactic radiotherapy.
Surgical and Nonsurgical Treatments
Surgical treatment is the treatment of choice in most cases of acoustic neuroma. Nonsurgical treatment is preferred in the following situations:
• Small tumors in elderly patients
• Tumor in the only hearing ear
• Poor general condition of the patient
Small Neuromas
In patients over the age of 65 years with small neuromas of 0.5 cm or less in the extrameatal diameter, without neurological symptoms, such as vertigo or unsteadiness, gadolinium-enhanced MRI is performed every 6 months for the first year then annually.24 The rate of growth of acoustic neuromas varies from 0.5 to 2.0 mm per year. In our experience, in approximately 70% of cases, tumors do not grow for the first 3 to 4 years.11 A longer period of follow-up is required to assess the rate of growth as rapid growth may still suddenly occur. Also, even an intracanalicular tumor may extend into the cochlea if it is localized at the fundus. Once it involves the cochlea, the chance of preserving hearing is lost. When a rapid growth rate is identified or if the patients present with sudden hearing loss on the tumor side, then surgery can be performed. In addition, tumor removal can be advised for patients with disturbing tinnitus even if they are over the age of 65 or older however, the tinnitus may or may not be resolved by the surgery. All patients should be made aware of the nature of their condition and all treatment options should be fully discussed.
Acoustic Neuroma in the Only Hearing Ear
The introduction of cochlear implants (CIs) and brainstem implants has greatly increased the treatment options available for patients with acoustic neuromas in the only hearing ear. However, we prefer to wait and scan, with a regular 6 monthly examination using gadolinium-enhanced MRI as well as hearing assessments.18 Hearing preservation surgery is always attempted if hearing becomes compromised or rapid tumor growth is noted, although the patient is made aware that the hearing may not be completely preserved. Furthermore, we would offer a CI on the contralateral deaf ear, if applicable, before making a decision on the acoustic neuroma.17 NF2 patients with bilateral vestibular schwannomas likely have a similar situation to the patient with vestibular schwannoma in the only hearing ear. Depending on tumor size, rate of growth, and the patient’s choice, radiosurgery with low-dose irradiation may be an option.
Acoustic Neuroma in Patients with Poor General Condition
In a patient with high anesthetic risk for the operation or in a patient with very poor rehabilitation potential, two options can be proposed:
1. Radiosurgery
2. Close observation with 6-monthly MRI scan
Radiosurgery
Radiosurgery is an option in recent times; however, it is not without complications such as hearing loss, facial and trigeminal nerve deficits, hydrocephalus, and malignant transformation. Moreover, 15 to 20% of the tumors continue to grow after radiosurgery.9
Tumor removal in patients who had previous radiotherapy is particularly difficult and more hazardous to the facial nerve and other cranial nerves.
Management of Elderly Patients
In elderly patients, surgery is not contraindicated as long as any existing comorbidities are well controlled. However, we must select them carefully based on strict guidelines, for example, rapidly expanding tumor, massive tumor or tumor causing cerebellar signs. Surgically, the dura, sigmoid sinus and jugular bulb are very fragile and utmost care must be applied during dissection.
Selecting the Surgical Approach
Translabyrinthine versus Hearing Preservation Surgeries
The main approaches for selecting the surgical method for acoustic neuroma includes (Fig. 31.3):
• Enlarged translabyrinthine approach (ETLA)
• Retrosigmoid-retrolabyrinthine (RS-RL) approach
• Enlarged middle cranial fossa approach (MCF)
The ETLA needs the most bone removal but obtains the best access to the CPA compared with the MCF and the RS. All these approaches have inherent advantages and disadvantages. The surgeon should know these and apply the best approach to the individual patient.
Indication of Enlarged Translabyrinthine Approach
Of the three approaches, the ETLA has the best outcome with regard to facial nerve function. This approach can be used to remove tumor of any size. There is no brain retraction required for this operation, thus providing the lowest frequency of postoperative neurological sequelae. It is therefore the approach of choice whenever hearing preservation is not being attempted.
Tumors exceeding 1.5 cm in extrameatal diameter in our practice were all removed using this approach regardless of preoperative hearing.1,21 The only exception to this protocol are two situations where we need to attempt hearing preservation–acoustic neuroma in the only hearing ear and some NF2 patients.17 Generally, it is almost always impossible to preserve useful hearing when the tumor is large.
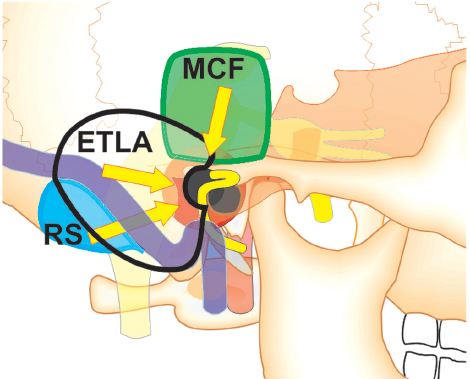
Figure 31.3 Three approaches are shown in the illustration. The enlarged translabyrinthine approach (ETLA) needs the most bone work but obtains the best access to the cerebellopontine angle than the other the middle cranial fossa approach (MCF) and the retrosigmoid approach (RS).
In tumors less than 1.5 cm but with hearing worse than modified Sanna classification B (i.e., pure tone average over 30 dB and speech discrimination score worse than 70%), we use the ETLA (Fig. 31.4). Furthermore, this approach is used when there is extension of the tumor into the fundus of the internal auditory canal. In our experience, lateral extension of the tumor into the fundus usually precludes any serviceable hearing even if hearing preservation technique is applied.
Since diminished preoperative hearing level usually implies that the cochlear nerve has already been compromised by the tumor, the possibility of preserving the preoperative hearing level is very low even in small tumors (less than 10%).10 In addition, the small percentage of cases in which the already poor preoperative hearing can be preserved should not be regarded as a success. Such a low hearing level and poor discrimination are practically useless to the patient, because the distorted signals received through those ears can be quite disturbing.
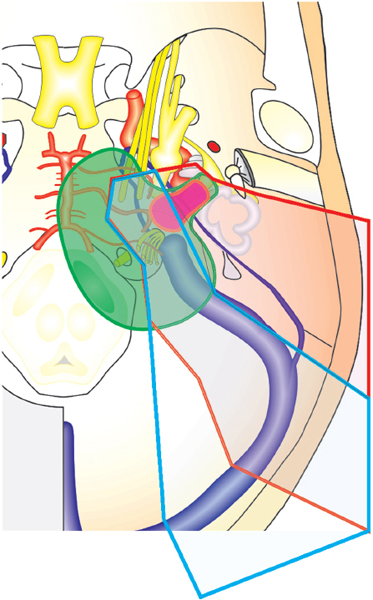
Figure 31.4 For removal of a small tumor (orange color), the retrosigmoid approach can be applied, but has a limit for a large tumor (green color) because of the necessity of excessive retraction of the cerebellum. The enlarged translabyrinthine approach can overcome these difficulties.
Special Consideration
In tumors larger than 1.5 cm in diameter and in tumors causing unserviceable preoperative hearing, hearing preservation at this time is not a parameter that should be considered in selecting the surgical approach. The parameters of importance in these cases are:
• Total tumor removal with the minimum neurological sequelae
• Uncomplicated and smooth postoperative course
• Good facial nerve results
Indications of Hearing Preservation Surgeries
Tumors smaller than 0.5 cm in the CPA in patients with good preoperative hearing (modified Sanna classification A and B) and in patients under 60 years of age, the enlarged middle fossa approach is used for preservation of hearing.11 In older patients with no disturbing symptoms, “wait and scan” and regular follow-up examinations are performed.
Tumors smaller than 1.5 cm in diameter in patients with good preoperative hearing (modified Sanna classification A and B) and with no extension into the fundus, a RS-RL approach is used.11
Borderline Cases
These are the nonstraightforward cases in which other parameters should be taken into consideration before selection of approach.
Regarding tumors larger than 0.5 cm and less than 1.5 cm in diameter with extension into the fundus in patients with good preoperative hearing, the decision depends on the patient’s age, his or her expectations, and a greater potential to preserve hearing.
Young patients with these parameters and a favorable axis of intraoperative vision, allowing better control of the lateral end of the internal auditory canal, can be managed using the RS-RL approach. This can go with the understanding that, if there is any doubt concerning residual tumor, the labyrinth should be sacrificed.
Older patients with tumors larger than 1 cm and with unfavorable parameters for hearing preservation can be managed by the ETLA (Figs. 31.5 and 31.6). It should be noted that there are no rigid rules, and each case should be dealt with individually after further discussion with the patient.
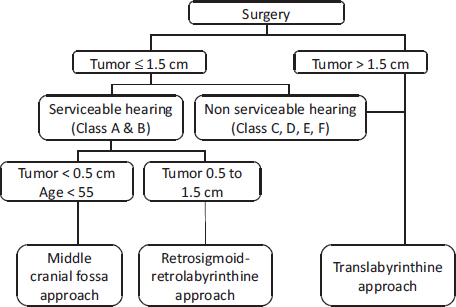
Figure 31.5 Algorithm for the selection of surgical approach.
In patients over 65 years of age with borderline hearing and tumors of approximately 1.5 cm in extrameatal diameter, the small likelihood of preserving serviceable hearing should be balanced against a safer approach with no cerebellar retraction and an increase of chances to preserve the facial nerve but with total hearing loss. Our preference is to offer the patient an ETLA.
In very rare cases with temporal bone or cochlear invasion, a transotic approach is used.20 In very large recurrent tumors in patients with long-standing preoperative facial nerve paralysis, a modified transcochlear approach is used.
Total versus Subtotal Removal
As a general rule, total removal has to be attempted in all cases of acoustic neuroma; however, subtotal removal can be preplanned or unplanned. It must be kept in mind that subtotal removal will lead to eventual recurrence, and revision surgery is more difficult and has a worse outcome when compared with primary surgery.
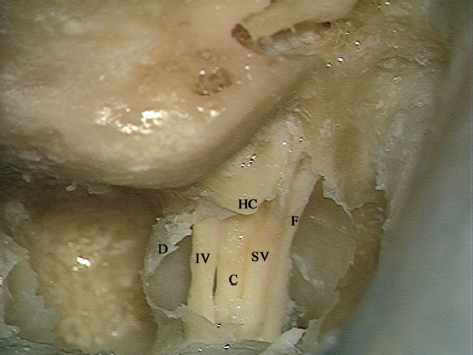
Figure 31.6 The contents of the internal auditory canal can be seen after opening the dura. C, cochlear nerve; D, dura of the canal; F, facial nerve; HC, horizontal crest; IV, inferior vestibular nerve; SV, superior vestibular nerve.
Preplanned Subtotal Removal
In patients over 70 years of age, a small part of the tumor may be left over the facial nerve at the level of the meatus. This reduces the injury to the nerve, and therefore more likely results in better facial nerve function postoperatively.
Cystic changes of acoustic neuroma usually result from degeneration because of relative ischemia following rapid growth. Cystic tumors frequently involve the arachnoid and thereby it may sometimes be impossible to identify the plane between the tumor and the surrounding brain tissue and nerves. In such cases, it is also prudent to leave the capsule of tumor attached to the brainstem and/or to the facial nerve.
Some surgeons advocate leaving a thin layer of tumor over the brain stem in all cases with adhesions because total removal is believed to cause major risks. In our experience, we have been able to establish a plane of cleavage between the tumor and the brain stem in all, but two cases, allowing safe total tumor removal from the brainstem.
Unplanned Subtotal Removal
In case of intraoperative complications, for example, bradycardia during surgery at the brainstem, or other anesthesia-related complications, it is prudent to stop the operation for a few minutes and then restart the dissection. However, if these complications are repeated, the operation should be terminated.
Occasionally, we are forced to leave some tumor behind because of the difficulty caused by certain anatomical variations (e.g., extremely low lying middle cranial fossa dura, remarkably protruding sigmoid sinus and jugular bulb). In such a case, another approach is applied later on.
Surgery in Cerebellopontine Angle: General Concepts
Internal Auditory Canal
Internal auditory canal is a meatus of almost 1 cm of length running in a lateral direction from the CPA through the petrous bone. Its orifice, called as porus, is observed in the posterior surface of the petrous bone. Its posterior border is formed by an acute angle while the anterior border is more flat. The dura of the posterior cranial fossa continues into the internal auditory canal lining the whole length and ends by merging with the contained nerves as they enter their corresponding foramina (Fig. 31.7). The long axis of the internal auditory canal lies in line with the long axis of the external auditory canal.2
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


