Abnormalities of the Anterior Segment
Pamela Hooker
In this chapter the most prevalent pathologies of the anterior segment encountered in the infant and pediatric population are discussed. Sight- or life-threatening disease processes are rare in this age group, but many less serious entities are commonly encountered. Etiology, prevalence, diagnosis, and treatment are all addressed.
Adnexa and Lids
Capillary Hemangioma
Capillary hemangiomas are the most common benign orbital tumor in children. They can occur anywhere within the orbit or more superficially, and present with red, flat lesions that grow quickly, proptosis, or both (1). Children with capillary hemangiomas require referral to an oculoplastic surgeon if removal is to be attempted, and they should be closely monitored for the development of amblyopia if the lesion obstructs the visual axis. Occasionally, biopsy is indicated if malignancy is suspected. These lesions can spontaneously resolve, but corticosteroids are often used to speed resolution, either by local injection or systemic administration.
Dermoid
Dermoids are formed by ectodermal tissue being trapped in bony sutures during development (1). They can occur superficially, or more deeply, on the conjunctiva or cornea, and can result in proptosis or optic neuropathy (1,2) (Fig. 12.1). The most common site for a dermoid cyst to appear is at the lateral eyebrow and the superionasal notch, and excision is usually recommended after 6 months of age. Although dermoid cysts are not themselves malignant, the potential exists for rupture of the cyst, which can lead to orbital cellulitis.
Congenital Arteriovenous Malformation
Congenital arteriovenous (AV) malformations appear in children as relatively low-flow, slow-growing lesions. Unlike capillary hemangiomas, growth of AV malformations tends to continue past the age of 1 year. If retinal involvement can be ruled out, the lesions can often be left untreated. Patients should be monitored for amblyopia development, however, if the visual axis is blocked.
Occasionally, AV malformations are found associated with Osler-Weber-Rendu or Wyburn-Mason syndromes, and patients should be referred for examination to rule out these entities.
Cellulitis
Although not as common as conjunctivitis, cellulitis is occasionally seen in the pediatric population, and can be quite serious (Fig. 12.2). Orbital cellulitis, the most common cause of proptosis in children (1), typically originates from infections in the paranasal sinuses. The most common bacterial causes include staphylococcus and streptococcus, as well as Haemophilus influenzae
if the child is not well immunized. Visual acuity is affected, and there is usually considerable swelling with closure of the lids and deficient extraocular motilities. Ultrasonography is a helpful diagnostic tool when the lids are too swollen to allow sufficient examination.
if the child is not well immunized. Visual acuity is affected, and there is usually considerable swelling with closure of the lids and deficient extraocular motilities. Ultrasonography is a helpful diagnostic tool when the lids are too swollen to allow sufficient examination.
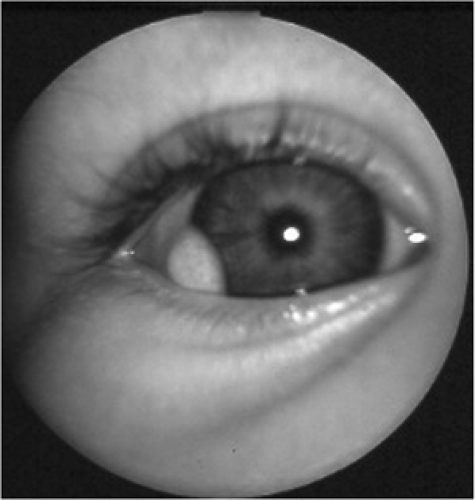 Figure 12.1. Dermoid cyst at corneal limbus. (Photo courtesy of Dr. Scott Richter). (See color well.) |
Treatment for cellulitis ranges from oral antibiotics on an outpatient basis (for preseptal cases) to hospitalization for intravenous administration. Occasionally, surgical draining of the sinuses is required.
Eyelid Laceration
A direct result of trauma, eyelid lacerations (Fig. 12.3) must be treated promptly to avoid intraocular infection. All patients with eyelid lacerations, regardless of age, need to have a comprehensive evaluation with dilation prior to treatment or surgical repair of the laceration to rule out any penetrating trauma to the globe. Orbital computed tomography (CT) scanning is useful for severe trauma, suspected orbital foreign body, or globe rupture.
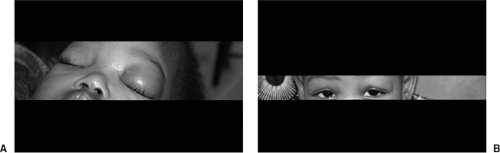 Figure 12.2. Preseptal cellulites. A: Active inflammation accompanied by high fever. B: Resolved condition. (Photos courtesy of Dr. Jeffrey Roth). (See color well.) |
In addition to in-office cleaning of the wound, surgical repair is often necessary, particularly if the laceration is large. Tetanus prophylaxis may also be indicated. If the laceration occurred at the lid margin, sutures are often left in place for 10 to 14 days. In other locations, sutures may be needed for only 4 to 6 days (3).
Blepharitis
Many children present with blepharitis of varying degrees. It can present with or without an accompanying conjunctivitis or meibomian gland dysfunction. A common cause of childhood blepharitis is staphylococcus infection, which usually manifests as chronic irritation of the lid, typically bilateral (4). Generally, also seen are ocular burning, conjunctival injection regardless of the presence or absence of frank conjunctivitis, and scales and collarettes around the lashes (3). Severe cases may also show neovascularization of the lid margin and possible madarosis.
Lid hygiene is the most important treatment that must be initiated in cases of active blepharitis. This typically involves lid scrubs two to three times per day with mild baby shampoo and water, as well as warm compresses to loosen
debris and help express capped meibomian glands. Proper lid hygiene is instrumental in preventing recurrence of the condition. If necessary, topical antibiotics can also be prescribed. Ointments work well, as the medication will stay in direct contact with the affected area for extended periods. Topical steroids can be added if the case is particularly severe.
debris and help express capped meibomian glands. Proper lid hygiene is instrumental in preventing recurrence of the condition. If necessary, topical antibiotics can also be prescribed. Ointments work well, as the medication will stay in direct contact with the affected area for extended periods. Topical steroids can be added if the case is particularly severe.
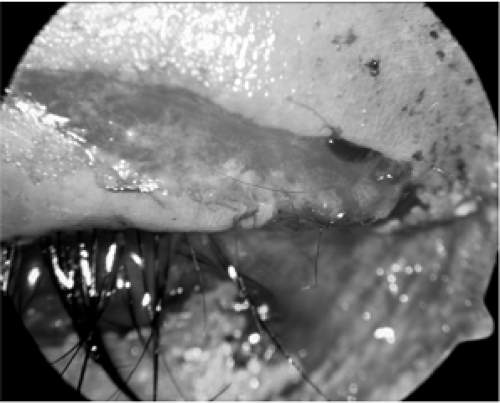 Figure 12.3. Eyelid laceration. (Photo courtesy of Dr. Jeffrey Roth). (See color well.) |
Dacryoadenitis
Dacryoadenitis is an orbital inflammation involving the lacrimal gland. The most common form of nonspecific orbital inflammation (1), it presents with pain and swelling along the upper lid in the region of the gland. Patients typically have a characteristic S-shape to the upper lid, and ptosis can be present if the swelling is significant. Diagnosis is aided with an orbital CT scan; treatment is usually with oral corticosteroids, with rapid resolution of inflammation.
Congenital Ptosis
Although ptosis can be caused by a number of entities, including birth trauma and myasthenia gravis, some children present with ptosis that is truly congenital. When faced with congenital ptosis as a possible diagnosis, it is important to rule out other conditions with careful history, paying special attention to parents’ reports and earlier photographs. Intermittent conditions (e.g., nocturnal lagophthalmos) must also be considered and investigated (5).
Amblyopia is a concern in patients in whom there is visual axis obstruction. Careful visual acuity and cycloplegic refraction should be performed to maximize the child’s vision. If the visual axis is obscured, or if cosmesis is a significant issue, surgical correction of the eyelid is indicated. In general, the more severe the ptosis, the earlier the condition should be corrected to reduce the risk of severe deprivational amblyopia.
Congenital Nasolacrimal Duct Obstruction
Two to four percent of full-term newborns will show a congenital blockage of their nasolacrimal duct, a condition referred to as “nasolacrimal duct obstruction” (NLDO). One study reported an incidence of 20%, which may be more inclusive of those instances in which the condition spontaneously resolves (6). The condition, which typically manifests when the infant is between 1 and 2 weeks of age, includes a history of excessive tearing when the child is not crying. NLDO occurs when the valve of Hasner does not fully open, and most obstructions spontaneously open within 4 to 6 weeks after birth. Approximately 80% of all patients with NLDO have spontaneous resolution by the age of 1 year (5,6,7).
Epiphora in infants can be a sign of congenital glaucoma, a condition which must be ruled out by careful slit lamp evaluation, intraocular pressure measurement, and dilated fundus examination, as well as measurement of the corneal diameters, which are typically enlarged in congenital glaucoma. Ocular infections of various types can also cause tearing or watery discharge, and should also be ruled out before making a diagnosis of NLDO.
Duct obstruction is fairly easy to treat due to its tendency to spontaneously resolve. Parents should be instructed to perform massage over the nasolacrimal duct, rubbing downward and using petroleum jelly or other lubricant safe for the eyes to protect the sensitive skin in that area. Follow-up care should be scheduled frequently to monitor for progress and possible acute dacryocystitis, which can occur within a blocked duct. If this occurs, systemic antibiotics are indicated, with surgical drainage as needed. If the NLDO does not resolve by the time the child reaches approximately 1 year of age, probing and irrigation of the duct are
indicated. Success rates above 95% have been reported if the probing is performed before 13 months of age, but the procedure is also helpful in patients older than 1 year. Occasionally, dacryocystorhinostomy is necessary for surgical bypass of the blockage in recalcitrant cases (5,8,9).
indicated. Success rates above 95% have been reported if the probing is performed before 13 months of age, but the procedure is also helpful in patients older than 1 year. Occasionally, dacryocystorhinostomy is necessary for surgical bypass of the blockage in recalcitrant cases (5,8,9).
Conjunctiva
Foreign Body
Children can acquire foreign bodies in as many ways as can be imagined. For most, treatment is the same as for adult patients. Symptoms can include irritation, pain, foreign body sensation, tearing, redness, a subjective history of getting something in the eye, or any combination of these. Clinical signs include injection, vertical corneal abrasions, which may stain with sodium fluorescein, and conjunctival or subconjunctival hemorrhage.
Foreign bodies should be differentiated from a number of other entities, including dry eye, blepharitis, conjunctivitis, trichiasis, recurrent corneal erosion, superficial punctate keratitis, contact lens-related problems, episcleritis, pterygium, or pinguecula. Most of these are easily discernable by outward appearance and subjective symptoms.
Clinical workup for foreign bodies includes a thorough history, slit lamp examination with measurement of intraocular pressure unless there is a known globe rupture, double lid eversion, and dilated fundus examination. Handheld slit lamps and non-contact tonometers (NCT) instruments are helpful for younger patients. In addition, B-scan ultrasonography and orbital CT scanning may be necessary.
The foreign body should be removed completely, using saline, cotton swab, spud, or forceps, as needed. The fornices should be swept for small particles as well. Antibiotic ointment with a pressure patch should be applied for the first 24 hours if the foreign body has left a central abrasion, and the child should be seen on the following day. Antibiotic drops can be used if an open abrasion remains, or the patch can be reapplied. Artificial tears and/or Celluvisc should be given for use every 1 to 2 hours once the patch is removed for residual abrasions or irritation caused by a foreign body. A follow-up visit should be scheduled for 1 week for known residual material (3).
Laceration
In addition to the eyelids, the conjunctiva can also be lacerated in cases of trauma. Symptoms with a conjunctival laceration can include pain, redness, foreign body sensation, or a history of trauma. Clinical signs that can be seen upon examination include sodium fluorescein stain of the conjunctiva, rolled conjunctival edges around the laceration, conjunctival or subconjunctival hemorrhage, and a possible direct view to the sclera if the laceration is sufficiently deep.
Work-up for conjunctival lacerations begins with a careful history to determine the nature of the injury, what type of object caused the laceration, and when the injury occurred. It is important to determine the risk of any possible penetrating injury as early as possible in the examination. Slit lamp examination with intraocular pressure (IOP) measurement (if no known globe rupture or penetrating injury) and dilation are indicated. B-scan, orbital CT, and exploratory surgery may all be necessary as well, particularly if a globe rupture is suspected.
The patient should be given antibiotic ointment three times a day (tid) for 7 days, with pressure patching as needed for 24-hour periods, depending on injury severity. Sutures are used as needed to close more significant lacerations. Follow-up visits will range from 24 hours to 1 week, depending on the extent of the injury and compliance with pressure patching and medication instillation (3).
Conjunctivitis



