Purpose
To compare the microbiological outcomes of membrane filter system and blood culture bottle techniques in culturing diluted vitrectomy cassette vitreous.
Design
Retrospective comparative case series.
Methods
Diluted vitrectomy cassette vitreous specimens from March 25, 2002 to July 11, 2012 were cultured using both membrane filter system and blood culture bottles. The isolates were divided into 3 groups: ones that had positive cultures with (1) both membrane filter system and blood culture bottles, (2) membrane filter system only, and (3) blood culture bottles only. The 48-hour as well as 2-week results were documented.
Results
A total of 447 patients with 168 positive cultures were studied. At the 48-hour time point, 126 isolates were documented. Of those, 104 (82%) were culture positive with both membrane filter system and blood culture bottles, 15 (12%) were culture positive only with membrane filter system, and 7 (6%) were culture positive only with blood culture bottles. At the 2-week time point, an additional 42 organisms were isolated. Of those, 19 (45%) were culture positive with both membrane filter system and blood culture bottles, 11 (26%) with membrane filter system only, and 12 (29%) with blood culture bottles only. Out of 168 total isolates, 123 (73%) were culture positive with both membrane filter system and blood culture bottles, 26 (16%) with membrane filter system only, and 19 (11%) with blood culture bottles only. Among all microbiological outcomes, there was no significant difference between membrane filter system and blood culture bottle ( P = .37). Of those organisms that were culture positive only with either membrane filter system or blood culture bottle, mold and Mycobacterium species were culture positive more commonly with membrane filter system ( P = .034 and P = .016, respectively), and gram-positive organisms were culture positive more commonly with blood culture bottles ( P = .021).
Conclusions
In the current study, a combination of membrane filter system and blood culture bottles for culture of diluted vitrectomy cassette vitreous provides the highest number of positive culture outcomes. The blood culture bottle method is technically easier and represents a viable alternative to the more complex membrane filter system technique.
Infectious endophthalmitis may occur after intraocular surgery or trauma, or can be of an endogenous source. The identification of the causative organism is of paramount importance as it allows a clinician to tailor therapies and to optimize patients’ visual outcomes. Initially endophthalmitis is treated empirically with broad-spectrum antibiotics. Culture results become especially important after 48 hours when a patient might need re-treatment, or if a patient is not responding and the treatment needs to be altered. When endophthalmitis is suspected, a specimen for culture can be obtained in several ways. It can be an anterior chamber sample, an undiluted vitreous sample, or a diluted vitreous sample. Vitreous specimens have higher rates of positive culture compared to aqueous samples. Undiluted vitreous is obtained either by vitreous tap and aspiration with a needle at the bedside or with a vitreous cutter connected to a syringe, instead of the aspiration line, before performing traditional pars plana vitrectomy in the operating room. Diluted vitreous can be obtained with the vitreous cutter once the infusion is turned on or from a vitrectomy cassette at the end of surgery. The current study focuses on comparing 2 culture techniques and microbiological outcomes for the diluted vitrectomy cassette vitreous.
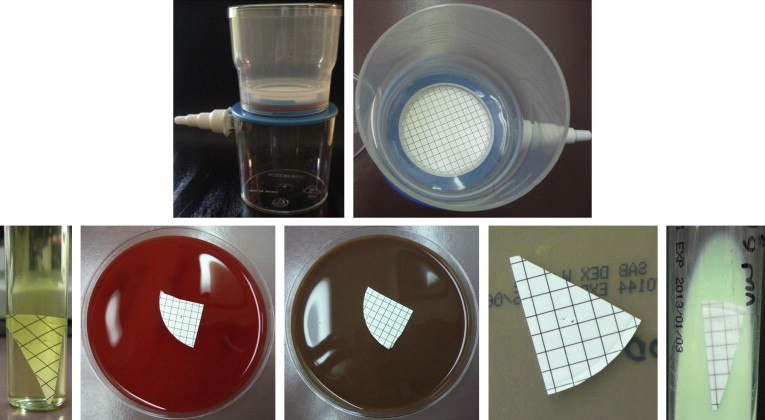
Techniques for culturing vitreous samples vary. The traditional method for culturing the undiluted vitreous is to place drops of the sample on solid media plates, into thioglycolate broth, as well as on slides for Gram stain. The traditional method for culturing the diluted vitrectomy cassette vitreous is membrane filter system. Membrane filter system requires sterile reconcentration of the diluted specimen by vacuum filtration over a 0.45-μm filter, cutting of the filter membrane into wedge-shaped portions, and placement of the sections on the appropriate media ( Figure ). Blood culture bottle technique represents an alternate method of culturing for both undiluted and diluted vitreous.
The comparison of blood culture bottle and traditional culturing techniques for undiluted vitreous has been the subject of several publications. However, these outcomes are hard to extrapolate to diluted vitrectomy cassette vitreous. In fact, there has been little published on utilization of the blood culture bottles for diluted vitrectomy cassette vitreous.
The current study compares microbiological outcomes of diluted vitrectomy cassette vitreous using both membrane filter system and blood culture bottle techniques at a university-based ocular microbiology laboratory. This study provides a direct comparison between the 2 culture techniques based on a large sample size of 447 patients over a 10-year period.
Methods
The current study is a retrospective comparative case series. The study was approved by the University of Miami Institutional Review Boards. The study examined the microbiological outcomes of diluted vitrectomy cassette vitreous specimens cultured from March 25, 2002 to July 11, 2012. Each sample was obtained from a standard 3-port pars plana vitrectomy performed at Bascom Palmer Eye Institute for clinical indications as deemed necessary by a surgeon. The vitrectomy itself was not done for the purposes of this study. Each sample was processed using both the traditional membrane filter system and blood culture bottle technique at the Bascom Palmer Eye Institute Ocular Microbiology Laboratory.
At the end of a vitrectomy, part of the vitreous effluent from the vitrectomy cassette was filtered through a 0.45-μm filter. The filter membrane was cut into wedges and cultured on blood agar, chocolate agar, Sabouraud agar, and Lowenstein-Jensen agar, and in thioglycolate broth.
Approximately 10 cc of diluted vitreous effluent was also injected into a blood culture bottle. During the study period Signal 70 mL and Septi-check 70 mL (both, Oxoid, Hampshire, UK) blood culture bottles were used. Both aerobic and anaerobic blood culture bottle cultures were set up. Blood culture bottles were observed manually on a daily basis for turbidity, color change, gas bubble production, and colony formation. In the Signal blood culture bottle, gas production forces fluid into the indicator chamber, indicating positive culture. An agar-coated paddle (biphasic system) was used in addition to liquid medium in the Septi-check blood culture bottle to aid in isolation of micro-organisms. If growth was detected, a Gram stain smear was prepared and appropriate subculture methods were used. Antimicrobial susceptibility testing was performed when appropriate.
The blood and chocolate agar plates were incubated at 35 C ± 2 C. Blood agar plates were incubated under both aerobic and anaerobic conditions; chocolate agar plates were incubated in 5% carbon dioxide. Sabouraud agar plates were incubated at 25 C. Lowenstein-Jensen agar was incubated at 35 C ± 2 C in an aerobic atmosphere supplemented with carbon dioxide, and thioglycolate broth at 35 C ± 2 C.
Only the vitrectomy cassette vitreous specimens that were cultured with both membrane filter system and blood culture bottles were studied. The indication for surgery was documented.
Plates and blood culture bottles were checked for growth daily. The time points used for the study included 24 hours, 48 hours, 1 week, and 2 weeks. “No growth” was reported at 7 days for blood agar, chocolate agar, and blood culture bottles; at 14 days for Sabouraud agar; at 21 days for thioglycolate broth; and at 8 weeks for Lowenstein-Jensen agar.
Organisms were classified as follows: (1) gram-positive organisms: Staphylococcus epidermidis , coagulase-negative Staphylococcus species, Staphylococcus aureus , Streptococcus species, Propionibacterium acnes , and miscellaneous gram-positive organisms; (2) gram-negative organisms; (3) Mycobacterium species; (4) fungal: yeast and mold.
Statistical analysis was performed using SPSS software (SPSS Inc, Chicago, Illinois, USA). The Pearson χ 2 test was used to compare the proportion of positive cultures using the membrane filter system and blood culture bottles overall and the proportion of positive cultures using the membrane filter system alone or blood culture bottles alone over positive culture in both membrane filter system and blood culture bottles. This was done for each organism as classified above. A P value <.05 was considered statistically significant.
Results
A total of 447 patients had diluted vitrectomy cassette vitreous specimens processed from March 25, 2002 to July 11, 2012. Out of 447 patients, 156 patients (35%) had positive culture results with either membrane filter system or blood culture bottles. Given that in some cases multiple organisms grew from the same sample or, in other cases, patients had separate positive cultures on different days, a total of 168 positive culture results were studied.
Out of 168 microbiological isolates that were culture positive with either membrane filter system or blood culture bottles, the most prevalent organisms was Staphylococcus epidermidis (n = 31), followed by yeast (n = 28), mold (n = 19), Propionibacterium acnes (n = 16), Streptococcus species (n = 15), coagulase-negative Staphylococcus species (n = 14), Mycobacterium species (n = 14), gram-positive organisms (n = 13), gram-negative organisms (n = 11), and Staphylococcus aureus (n = 7).
First examined were the combined 24- and 48-hour results. By 48 hours, a total of 126 organisms were culture positive with either or both of these methods. Out of 126 positive cultures, 104 (82%) grew with both membrane filter system and blood culture bottles. Fifteen (12%) grew only using the membrane filter system (mold [n = 5], coagulase-negative Staphylococcus species [n = 2], Mycobacterium species [n = 2], gram-negative organisms [n = 2], yeast [n = 2], Staphylococcus aureus [n = 1], and Staphylococcus epidermidis [n = 1]). Seven (6%) grew only with blood culture bottles ( Staphylococcus epidermidis [n = 4], coagulase-negative Staphylococcus species [n = 2], and Streptococcus species [n = 1]).
An additional 42 positive cultures were identified upon consideration of 1- and 2-week results (between 48 hours and 2 weeks). Out of the additional 42 microbiological isolates, 19 (45%) were culture positive with both membrane filter system and blood culture bottles. Eleven (26%) grew only using the membrane filter system ( Mycobacterium species [n = 5], mold [n = 3], gram-positive organisms [n = 1], Propionibacterium acnes [n = 1], and yeast [n = 1]). Twelve (29%) grew only with blood culture bottles ( Propionibacterium species [n = 5], gram-positive organisms [n = 2], coagulase-negative Staphylococcus species [n = 1], Staphylococcus epidermidis [n = 1], mold [n = 1], Streptococcus species [n = 1], and Staphylococcus species [n = 1]).
When the microbiological isolates were combined together, out of a total 168 positive cultures, 123 organisms (73%) grew with both membrane filter system and blood culture bottles ( Staphylococcus epidermidis [n = 25], yeast [n = 25], Streptococcus species [n = 13], gram-positive organisms [n = 10], mold [n = 10], Propionibacterium acnes [n = 10], gram-negative organisms [n = 9], coagulase-negative Staphylococcus species [n = 8], Mycobacterium species [n = 7], and Staphylococcus aureus [n = 6]). Twenty-six (16%) were culture positive only with membrane filter system (mold [n = 8], Mycobacterium species [n = 7], yeast [n = 3], coagulase-negative Staphylococcus species [n = 2], gram-negative organisms [n = 2], Staphylococcus aureus [n = 1], Staphylococcus epidermidis [n = 1], gram-positive organisms [n = 1], and Propionibacterium acnes [n = 1]). Nineteen organisms (11%) were culture positive only with blood culture bottles ( Staphylococcus epidermidis [n = 5], Propionibacterium species [n = 5], coagulase-negative S taphylococcus species [n = 3], Streptococcus species [n = 2], gram-positive organisms [n = 2], mold [n = 1], and Staphylococcus species [n = 1]).
Among all microbiological outcomes, there was no significant difference between membrane filter system and blood culture bottle techniques ( P = .37). When comparing the proportion of positive cultures using the membrane filter system alone or blood culture bottles alone over positive cultures using both membrane filter system and blood culture bottles, mold ( P = .034) and Mycobacterium species ( P = .016) were culture positive more commonly with membrane filter system, while gram-positive organisms were culture positive more commonly with blood culture bottles ( P = .021).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


