CHAPTER 5
Glaucoma
INTRAOCULAR PRESSURE AND AQUEOUS HUMOR DYNAMICS
Glaucoma is a group of diseases resulting in an optic neuropathy that has characteristic changes in the optic nerve head (cupping) and progressive visual field loss. Elevated intraocular pressure is one of the primary associated risk factors but does not define the disorder.
 Intraocular pressure (IOP) is determined by the balance of aqueous humor production, outflow facility, and episcleral venous pressure.
Intraocular pressure (IOP) is determined by the balance of aqueous humor production, outflow facility, and episcleral venous pressure.
 Quantified by the Goldmann equation:
Quantified by the Goldmann equation:

where Po = IOP (millimeters of mercury).
F = Formation of aqueous (microliters per minute) = 2 to 3 μL/min in normal patients (0.5% to 1%/min).
C = Facility of outflow (microliters per minute per millimeter of mercury) = 0.28 μL/min/mm of mercury in normal patients.
Pv = Episcleral venous pressure (millimeters of mercury) = 8 to 9 mm Hg.
Composition of Aqueous Humor
 Aqueous humor is a clear medium that is slightly hypertonic compared to plasma. It maintains IOP and nourishes the lens, cornea, etc.
Aqueous humor is a clear medium that is slightly hypertonic compared to plasma. It maintains IOP and nourishes the lens, cornea, etc.
 No blood cells in normal aqueous humor
No blood cells in normal aqueous humor
 Inorganic ions:
Inorganic ions:
Na+, K+, and Mg2+ concentration similar to plasma.
Ca2+ half of plasma level.
Cl− and HCO3− are major anions.
 Organic anions:
Organic anions:
Lactate most abundant organic ion.
Ascorbic acid at very elevated levels (15 to 50 times plasma levels).
 Carbohydrates:
Carbohydrates:
Glucose about 70% plasma concentration, from facilitated transport into aqueous.
Higher levels in diabetics.
 Glutathione: important role in oxidative state of aqueous humor.
Glutathione: important role in oxidative state of aqueous humor.
 Urea:
Urea:
Approximately 85% of plasma concentration.
Crosses blood–aqueous barrier easily.
 Proteins:
Proteins:
Aqueous almost devoid of protein (1/200 to 1/500 of the protein found in plasma).
Enzymes with possible roles in the anterior chamber:
Hyaluronidase: may increase outflow facility of aqueous humor.
Carbonic anhydrase: regulation of bicarbonate levels in aqueous humor.
Lysozyme: antimicrobial role.
 Growth factors: higher levels in aqueous than plasma of TGF-β, acidic fibroblast growth factor (FGF) and basic FGF, insulin-like growth factor 1 (IGF-1), and transferrin.
Growth factors: higher levels in aqueous than plasma of TGF-β, acidic fibroblast growth factor (FGF) and basic FGF, insulin-like growth factor 1 (IGF-1), and transferrin.
 O2 and CO2.
O2 and CO2.
O2 at approximately 55 mm Hg: one third of atmosphereic concentration, corneal endothelium completely dependent on this source.
CO2 present at 40 to 60 mm Hg.
Production of Aqueous Humor
 Produced by ciliary processes, each composed of a central core of capillaries and connective tissue surrounded by an inner nonpigmented and an outer pigmented layer of epithelium (Figure 5.1). The nonpigmented and pigmented layers are arranged so that they face apex to apex, and the basement membrane of the nonpigmented layer faces the posterior chamber (PC).
Produced by ciliary processes, each composed of a central core of capillaries and connective tissue surrounded by an inner nonpigmented and an outer pigmented layer of epithelium (Figure 5.1). The nonpigmented and pigmented layers are arranged so that they face apex to apex, and the basement membrane of the nonpigmented layer faces the posterior chamber (PC).
 Three basic mechanisms: simple diffusion (passive movement of solutes governed by charge and concentration gradient), ultrafiltration (movement of water and solutes down pressure gradient), and active secretion (pressure-independent movement of substances against an electrochemical gradient by consumption of energy).
Three basic mechanisms: simple diffusion (passive movement of solutes governed by charge and concentration gradient), ultrafiltration (movement of water and solutes down pressure gradient), and active secretion (pressure-independent movement of substances against an electrochemical gradient by consumption of energy).
 Active transport is the major mechanism of aqueous formation; probably involves sodium pump at level of the nonpigmented epithelium.
Active transport is the major mechanism of aqueous formation; probably involves sodium pump at level of the nonpigmented epithelium.
 Inhibition by β-adrenergic antagonists (e.g., timolol), carbonic anhydrase inhibitors (CAIs) (e.g., acetazolamide and dorzolamide), and α2-adrenergic agonists (e.g., brimonidine and apraclonidine).
Inhibition by β-adrenergic antagonists (e.g., timolol), carbonic anhydrase inhibitors (CAIs) (e.g., acetazolamide and dorzolamide), and α2-adrenergic agonists (e.g., brimonidine and apraclonidine).
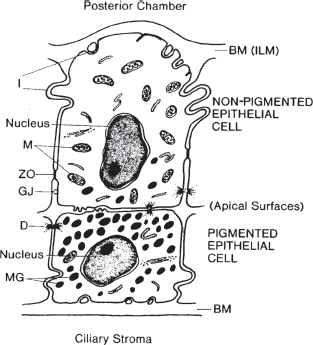
FIGURE 5.1. The ciliary body has two layers of epithelium aligned apex to apex. The pigmented epithelium is adjacent the stroma, whereas the nonpigmented epithelium is in contact with the posterior chamber. (From Shields MB. Textbook of glaucoma, 4th ed. Baltimore, MD: Lippincott Williams & Wilkins, 1998:10, with permission.)
Outflow
 Two pathways: trabecular (accounts for about 60% to 80% of outflow) and uveoscleral (remaining 20% to 40%).
Two pathways: trabecular (accounts for about 60% to 80% of outflow) and uveoscleral (remaining 20% to 40%).
 Trabecular meshwork (TM) is anatomically divided into uveal (most inner), corneoscleral, and juxtacanalicular (outermost) meshwork. Site of greatest resistance is the juxtacanalicular meshwork. Aqueous humor passes across meshwork into Schlemm’s canal and ultimately drains into episcleral veins (Figure 5.2).
Trabecular meshwork (TM) is anatomically divided into uveal (most inner), corneoscleral, and juxtacanalicular (outermost) meshwork. Site of greatest resistance is the juxtacanalicular meshwork. Aqueous humor passes across meshwork into Schlemm’s canal and ultimately drains into episcleral veins (Figure 5.2).
 Uveoscleral outflow from the anterior chamber through the ciliary muscle and into the suprachoroidal space and sclera, drained by emissarial channels of the sclera: increased by cycloplegia, adrenergic agonists (e.g., epinephrine), and prostaglandin analogues (e.g., latanoprost) in glaucoma therapy.
Uveoscleral outflow from the anterior chamber through the ciliary muscle and into the suprachoroidal space and sclera, drained by emissarial channels of the sclera: increased by cycloplegia, adrenergic agonists (e.g., epinephrine), and prostaglandin analogues (e.g., latanoprost) in glaucoma therapy.
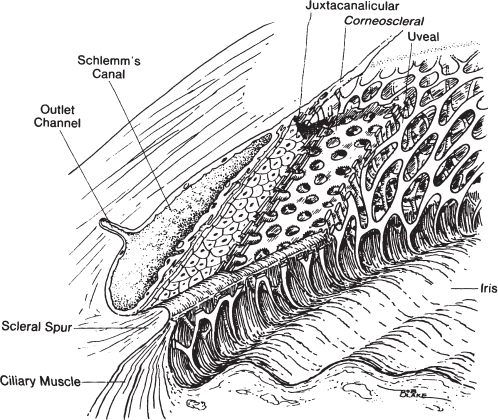
FIGURE 5.2. Diagram of the trabecular meshwork in cross section. (From Shields MB. Textbook of glaucoma, 4th ed. Baltimore, MD: Lippincott Williams & Wilkins, 1998:17, with permission.)
Intraocular Pressure Measurement Techniques
 Methods include indentation, applanation, rebound, noncontact, and pneumatic tonometry.
Methods include indentation, applanation, rebound, noncontact, and pneumatic tonometry.
 Indentation tonometry exemplified by Schiotz tonometer:
Indentation tonometry exemplified by Schiotz tonometer:
Consists of concave footplate contiguous with plunger that slides within shaft. Shaft displaces a lever system and provides a reading that can be converted to millimeters of mercury. Performed in supine position.
Reading is strongly influenced by ocular rigidity: falsely high in rigid eyes (hyperopia) and falsely low in nonrigid eyes (high myopia, use of cholinesterase inhibitors, and prior ocular surgery).
 Applanation tonometry includes Goldmann tonometer, Perkins tonometer, and Tono-Pen:
Applanation tonometry includes Goldmann tonometer, Perkins tonometer, and Tono-Pen:
Goldmann and Perkins tonometers function based on Imbert-Fick law:

where P = pressure, F = force, and A = area. IOP (P) is measured as the force (F) necessary to flatten the corneal apex a given area (A); diameter of 3.06 mm chosen because the surface tension of tears is counterbalanced by ocular rigidity at this diameter. In addition, multiplying the applied force by 10 gives IOP in millimeters of mercury. The area of flattening is assessed by placing fluorescein in the eye and using a split-field device to determine the flattened area (Figure 5.3)
Sources of error include excessive eyelid squeezing, Valsalva maneuver, pressure on the globe, extraocular muscle force applied to a restricted globe, corneal scarring or band keratopathy, corneal edema, excessive fluorescein (overestimates IOP), inadequate fluorescein (underestimates IOP), and astigmatism. Inaccuracy in cases of astigmatism can be minimized by rotating prism so that axis of least corneal curvature is opposite red mark on prism holder, or by taking average of two readings 90 degrees apart.
Tono-Pen uses constant area of applanation and determines force necessary to applanate this area. Several values are obtained and averaged to provide a digital readout. Less accurate at extreme values of IOP (overestimates low values and underestimates high values).
 Rebound tonometry (e.g., Icare tonometer):
Rebound tonometry (e.g., Icare tonometer):
A very light probe is used to make momentary contact with the cornea. Induction-based coil system measures probe deceleration, contact time, and other parameters during measurement. This information is used to calculate IOP.
 Noncontact (air-puff) tonometry:
Noncontact (air-puff) tonometry:
The force of the air stream increases linearly with time and stops when a given area of the central cornea is flattened. The duration of the air stream is converted to IOP.
Accurate in normal range but poor at extreme values, acceptable for mass screening.
 Pneumatic tonometry:
Pneumatic tonometry:
Composed in part of a probe with a floating pneumatic sensor and a rubber membrane that blocks the flow of air through the probe until the pressure buildup equals IOP.
Useful in cases of corneal scarring and edema.
 Central corneal thickness (CCT) effects on IOP measurement:
Central corneal thickness (CCT) effects on IOP measurement:
Thicker corneas overestimate IOP in a nonlinear fashion (~ 0.5 mm Hg difference for every 10 μm away from the population mean of 542 μm using Goldmann tonometry); conversely, thinner corneas underestimate IOP.
Hydration of the cornea (corneal edema) decreases its resistance to flattening and thus underestimates IOP (~ −2 mm Hg for every 70 μm change in corneal thickness, using Goldmann tonometry).
PRK/LASIK, which thin the cornea, cause underestimation of IOP.
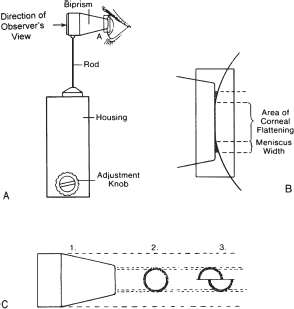
FIGURE 5.3. Diagram of the Goldmann applanation tonometer. The area of indentation is fixed, and the pressure can be derived. A: Diagrammatic representation of tonometer in apposition to the eye. B: Enlarged illustration of the corneal flattening created by the applanation by the tonometer tip. C: 1, Appearance of the tonometer; 2, tip cross section; 3, view of meniscus when viewed through the slit lamp. (From Shields MB. Textbook of glaucoma, 4th ed. Baltimore, MD: Lippincott Williams & Wilkins, 1998:55, with permission.)
CLINICAL EVALUATION OF GLAUCOMA
1. History including chief complaint, symptoms/onset/duration/severity, family history of glaucoma and vision loss, steroid use, previous IOP values, general medical history and medications, eye surgeries, and laser procedures.
2. Refraction for best acuity.
3. External examination to check for prominent episcleral veins or displacement of the globe from orbital disease.
4. Pupil examination to assess asymmetry of glaucomatous optic atrophy or possible corectopia or polycoria (iridocorneal endothelial [ICE] syndrome).
5. Slit-lamp examination to check for associated factors such as anterior chamber inflammation, pseudoexfoliation, and transillumination defects.
6. Perimetry to quantify visual field loss.
7. Tonometry.
8. Gonioscopy to assess angle width, presence of pigment, or peripheral anterior synechiae (PAS), etc.
9. Ophthalmoscopy to accurately assess optic disk contour and cup-to-disk ratio.
10. Special tests:
Tonography: assesses outflow facility by applying a known weight to the eye and measuring the change in IOP over time resulting from increased aqueous outflow.
Darkroom prone provocative test (DRPPT): compares IOP in supine position (not sitting) to IOP in prone position (in the dark and after 45 minutes). A rise of 9 mm Hg or more is considered a positive test result for occludable angle, and 4 to 8 mm Hg is equivocal.
Gonioscopy
Normal Angles
 Angle cannot be visualized without goniolens, since light reflected from angle undergoes total internal reflectivity at the air-cornea surface.
Angle cannot be visualized without goniolens, since light reflected from angle undergoes total internal reflectivity at the air-cornea surface.
 Goniolens eliminates this interface with a surface of higher refractive index, allowing light from angle structures to leave at an angle greater than the angle of total internal reflectivity.
Goniolens eliminates this interface with a surface of higher refractive index, allowing light from angle structures to leave at an angle greater than the angle of total internal reflectivity.
 Goniolenses are of two types, direct and indirect:
Goniolenses are of two types, direct and indirect:
Direct includes Koeppe lens, which consists of 50-diopter (D) concave lens with a back surface that fits onto the anesthetized cornea. Other examples include the Layden, Swan-Jacobs, and Hoskins-Barkan lenses. The angle is visualized using a handheld binocular magnifier and a separate light source. Advantages of Koeppe gonioscopy include direct panoramic view of entire angle, ease of changing viewing angle into the angle of the eye (useful in cases of concave iris), and ability to rapidly compare the angle of both eyes.
Indirect includes Zeiss or Volk four-mirror and Goldmann mirror lenses. The Zeiss has an interface surface flatter than the corneal surface, eliminating the need for a coupling agent. The Goldmann lens is steeper than the cornea and requires a high-viscosity coupling agent; contact surface is actually on the sclera.
Advantages of the Zeiss lens include rapidity of application, no need for coupling interface solution (saline for Koeppe and high-viscosity agent for Goldmann), and ability to perform compression gonioscopy (the application of force on the cornea with the Zeiss lens to open the angle).
 Angle structures from anterior to posterior are cornea, Schwalbe’s line, anterior TM, posterior TM, scleral spur, ciliary body band, and iris (Figure 5.4).
Angle structures from anterior to posterior are cornea, Schwalbe’s line, anterior TM, posterior TM, scleral spur, ciliary body band, and iris (Figure 5.4).
 Grading systems of angle depth include Shaffer, Spaeth, and van Herick systems.
Grading systems of angle depth include Shaffer, Spaeth, and van Herick systems.
Shaffer system is graded as follows:
Grade 0 = Closed angle.
Grade slit = 5 degrees or less.
Grade I = 10 degrees.
Grade II = 20 degrees.
Grade III = 30 degrees.
Grade IV = 40 degrees or greater.
Grades slit, I, and II are considered occludable angles.
Spaeth system includes Shaffer system but expands to include description of angle configuration and iris insertion.
R = Regular, no significant iris bowing.
S = Steep, iris arises from its root in steep convex curve.
Q = Quixotic, iris bows posteriorly (concave) from its root.
A = Above Schwalbe’s line, closed angle.
B = Below Schwalbe’s line, attachment to TM.
C = Scleral spur.
D = Deep, anterior ciliary body visible.
E = Extremely deep, unusually large portion of ciliary body band visible.
Current nomenclature for the description of an angle includes appearance of iris insertion in parentheses followed by anatomic insertion; for example, (C)D = anatomic insertion at the ciliary body but appears to be just below scleral spur without compression gonioscopy. Furthermore, an angle may be described with a number to indicate the angle of iris approach followed by letters to indicate iris insertion and angle configuration (e.g., 30CS).
van Herick technique grades angle depth based on slit-lamp examination, not gonioscopy. A thin beam is focused at an angle of 45 to 60 degrees on the cornea and anterior chamber (AC) at the temporal limbus.
I = AC depth < one fourth corneal thickness.
II = One fourth corneal thickness.
III = One fourth to half corneal thickness.
IV = Up to full corneal thickness or greater.
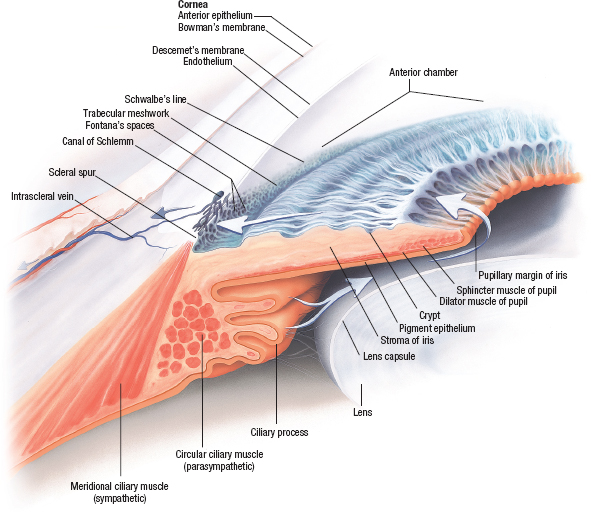
FIGURE 5.4. Gonioscopic view of the angle structures. (Asset provided by Anatomical Chart Co.)
Abnormal Angles
Abnormal angle vessels: Normal radial iris vessels may cross angle; neovascular vessels (Figure 5.5) typically arborize at the TM and can cause contraction and PAS.
Pigmentation: Increased meshwork pigmentation may be seen with aging and in pigmented individuals; however, heavy pigmentation or Sampaolesi line (accumulation of pigment along ridge where cornea transitions into the angle recess) suggests possible pseudoexfoliation, pigment dispersion syndrome, or trauma.
PAS: Adhesions between iris and TM; signify prior AC inflammation, appositional angle closure, angle neovascularization, corneal endothelial migration (ICE syndrome), or trauma. PAS tend to be sheetlike connections, whereas iris processes are fine, wispy extensions from the iris to the cornea.
Cyclodialysis cleft: Typically after trauma, the ciliary body is separated from the ciliary sulcus and its attachment to the scleral spur, leaving a deep cleft. This can cause hyposecrection of aqueous humor and/or increased filtration of aqueous humor to the suprachoroidal space (uveoscleral outflow), leading to hypotony.
Iridodialysis: After blunt trauma, separation of the iris root from the ciliary body occurs. This can be seen along with or separate from a cyclodialysis cleft. Usually associated with hyphema, may not be recognized until anterior chamber blood has cleared. Can cause monocular diplopia and polycoria.
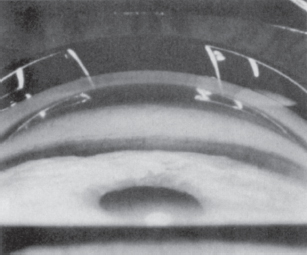
FIGURE 5.5. Neovascular vessels in the angle are evidence of severe posterior segment ischemia. (From Epstein DL. Chandler and Grant’s glaucoma, 4th ed. Baltimore, MD: Lippincott Williams & Wilkins, 1997:72, with permission.)
Optic Nerve
Assessment of Optic Nerve Changes
 Best method is use of slit lamp and a Hruby lens, a posterior pole contact lens, or a 60-, 78-, or 90-D lens.
Best method is use of slit lamp and a Hruby lens, a posterior pole contact lens, or a 60-, 78-, or 90-D lens.
 Cup-to-disk (c/d) ratio: Assess both horizontal and vertical dimensions. The physiologic c/d ratio is genetically determined. Two thirds of normal c/d ratios are less than 0.3, and only 6% of the normal population has c/d of 0.5 or greater. C/d ratios greater than 0.3 should be viewed with suspicion. The size of the disk correlates with the size of the cup. Smaller optic disks tend to have smaller physiologic cups and vice versa. Normal optic disk size is approximately 1.5 to 2.2 mm in diameter. For quantitative measurement of optic disk diameter, use the slit lamp and adjust the height of the slit beam to match the vertical diameter of the disk. The lens used must be taken into account for calculation: Multiply measurement by 1.1 for a 78-D lens and by 1.3 for a 90-D lens. Progressive enlargement of the cup is evidence of glaucoma, and c/d asymmetry of 0.2 or greater is very suspect for glaucoma. It should be noted that blacks have a higher physiologic c/d ratio in general.
Cup-to-disk (c/d) ratio: Assess both horizontal and vertical dimensions. The physiologic c/d ratio is genetically determined. Two thirds of normal c/d ratios are less than 0.3, and only 6% of the normal population has c/d of 0.5 or greater. C/d ratios greater than 0.3 should be viewed with suspicion. The size of the disk correlates with the size of the cup. Smaller optic disks tend to have smaller physiologic cups and vice versa. Normal optic disk size is approximately 1.5 to 2.2 mm in diameter. For quantitative measurement of optic disk diameter, use the slit lamp and adjust the height of the slit beam to match the vertical diameter of the disk. The lens used must be taken into account for calculation: Multiply measurement by 1.1 for a 78-D lens and by 1.3 for a 90-D lens. Progressive enlargement of the cup is evidence of glaucoma, and c/d asymmetry of 0.2 or greater is very suspect for glaucoma. It should be noted that blacks have a higher physiologic c/d ratio in general.
 Rim contour: Focal neural rim damage may be detected as focal notching, thinning, or pallor and have corresponding visual field loss on perimetry. In normal individuals, neuroretinal rim thickness follows the ISNT rule: I = inferior rim is the thickest, followed by S = superior, N = nasal, and finally the T = temporal portion of the rim.
Rim contour: Focal neural rim damage may be detected as focal notching, thinning, or pallor and have corresponding visual field loss on perimetry. In normal individuals, neuroretinal rim thickness follows the ISNT rule: I = inferior rim is the thickest, followed by S = superior, N = nasal, and finally the T = temporal portion of the rim.
 Disk splinter hemorrhage: focal sign for glaucomatous damage; may signify progression of glaucoma and be recurrent. More commonly seen in normal tension glaucoma (Figure 5.6).
Disk splinter hemorrhage: focal sign for glaucomatous damage; may signify progression of glaucoma and be recurrent. More commonly seen in normal tension glaucoma (Figure 5.6).
 Nerve fiber layer: best viewed with red-free illumination. Both wedge-shaped focal loss and diffuse atrophy can occur in glaucoma.
Nerve fiber layer: best viewed with red-free illumination. Both wedge-shaped focal loss and diffuse atrophy can occur in glaucoma.
 Peripapillary atrophy (PPA) occurs as two types: alpha-zone and beta-zone peripapillary atrophy. It represents loss of choriocapillaris and RPE adjacent to the optic disk. Alpha-zone PPA is the outer or peripheral zone of PPA that can be seen in normal patients and other disease states (e.g., myopia). It has unknown impact on glaucoma. Beta-zone PPA is the central zone of atrophy adjacent to the disk that has been shown to be present with higher frequency and to a greater degree in patients with glaucoma.
Peripapillary atrophy (PPA) occurs as two types: alpha-zone and beta-zone peripapillary atrophy. It represents loss of choriocapillaris and RPE adjacent to the optic disk. Alpha-zone PPA is the outer or peripheral zone of PPA that can be seen in normal patients and other disease states (e.g., myopia). It has unknown impact on glaucoma. Beta-zone PPA is the central zone of atrophy adjacent to the disk that has been shown to be present with higher frequency and to a greater degree in patients with glaucoma.
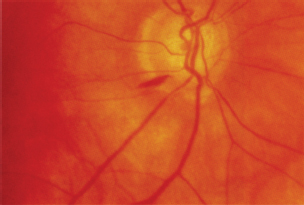
FIGURE 5.6. Splinter hemorrhage at the disk margin.
Visual Fields
Defined as the entire visual space one can see at a given moment. For each eye, the visual field extends 90 degrees temporally, 70 degrees inferiorly, 60 degrees nasally, and 50 degrees superiorly.
 Hill of vision: refers to the three-dimensional representation of differential light sensitivity in the visual field (Figure 5.7). The best visual acuity is at the apex of the hill and descends from there, more steeply nasally than temporally.
Hill of vision: refers to the three-dimensional representation of differential light sensitivity in the visual field (Figure 5.7). The best visual acuity is at the apex of the hill and descends from there, more steeply nasally than temporally.
 Perimetry refers to the testing of the visual field:
Perimetry refers to the testing of the visual field:
Threshold: dimmest spot able to be detected. The bracketing method is used to determine threshold in computerized static perimetry. Threshold testing is preferable in glaucoma patients and suspects.
Suprathreshold: light stimulus greater than threshold. Suprathreshold testing is useful for screening individuals not suspected of having glaucoma.
Kinetic testing: testing of sensitivity by moving a light stimulus from nonseeing to seeing portion of the visual field.
Static testing: testing of points in the visual field using fixed points.
Isopter: demarcation between visible and nonvisible parts of the visual field; represents edge of threshold.
Scotoma: area of depressed light sensitivity compared with surrounding visual field; may be relative or absolute.
Luminescence: can be measured in apostilbs (asb) or decibels (dB). Apostilbs are nonlogarithmic units that increase with increasing intensity (decreasing light sensitivity). However, decibels are measured as 0.1 log units of light sensitivity and increase as the light stimulus becomes dimmer.
Isopter notations for the Goldmann perimeter are Roman numeral for spot size (area increases by fourfold per unit), Arabic numeral for light intensity (increases by 0.5 log unit or 3.15 per numeral), and lowercase letter for intermediate intensities (increases by 0.1 log unit per letter). Since spot size and intensity are related reciprocally, equivalent targets can be used by varying the two parameters (e.g., I4e = II3e = III2e = IV1e). Stimulus size, as stated above, increases fourfold per unit: 0 = 1/16 mm2, I = 1/4 mm2, II = 1 mm2, III = 4 mm2, IV = 16 mm2, and V = 64 mm2.
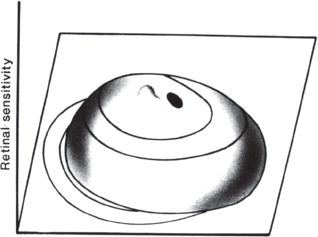
FIGURE 5.7. Hill of vision. The higher areas near the fovea represent greater light sensitivity.
Static Versus Dynamic Perimetry
 Advantages of kinetic perimetry (e.g., Goldmann):
Advantages of kinetic perimetry (e.g., Goldmann):
Rapid assessment of isopter contours and scotomas.
Familiarity among clinicians.
Goldmann perimeters are relatively inexpensive.
More dynamic interaction with patient.
 Disadvantages of kinetic testing:
Disadvantages of kinetic testing:
Requires more skilled technical assistance.
Testing is usually suprathreshold and may not detect early changes.
Not as quantitative as computerized static perimetry.
 Advantages of computerized static perimetry (e.g., Humphrey, Octopus):
Advantages of computerized static perimetry (e.g., Humphrey, Octopus):
Quantifiable results that are reproducible.
Tests threshold with greater sensitivity.
Computer-programmed operation does not require highly skilled training.
 Disadvantages of computerized static perimetry:
Disadvantages of computerized static perimetry:
More detailed data making interpretation more difficult.
Time-consuming and demanding on patient.
Equipment is more expensive.
Perimeter Defects and Errors
 Defects resulting from glaucomatous optic nerve damage:
Defects resulting from glaucomatous optic nerve damage:
Paracentral scotoma: round or ovoid defect within 10 degrees of fixation, an early defect seen in glaucoma; may be more common in low-tension glaucoma.
Arcuate Bjerrum scotoma: bowlike defect extending from blind spot to the horizontal raphe; occurs in the area 10 to 20 degrees from fixation (Figure 5.8).
Nasal step: defect in the nasal periphery respecting the horizontal raphe in which there is relative depression compared with the corresponding area of the opposite hemifield (Figure 5.9).
Temporal wedge: wedge-shaped defect extending from blind spot to the periphery.
Split fixation: central scotoma that respects the horizontal raphe; ominous sign.
Central island: both superior and inferior hemifield loss leaving only central island of tunnel vision; indicates very advanced glaucoma.
 Errors and artifacts in perimetry:
Errors and artifacts in perimetry:
Lens rim artifact: peripheral depression due to malpositioned lens.
Incorrect refraction: generalized depression.
Cloverleaf pattern: due to inattention late in computerized perimetry, since the program tests points in all four quadrants early on.
High false-positive rate: results in “white scotomas” on computerized fields because of impossibly high sensitivities.
Media opacity or miosis: cataracts and pilocarpine may cause generalized depressed fields.
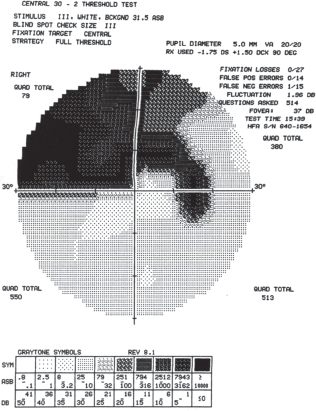
FIGURE 5.8. Bjerrum scotoma.

FIGURE 5.9. Nasal step.
Primary Open-Angle Glaucoma
Summary
Primary open-angle glaucoma (POAG) is generally a chronic, slowly progressive optic neuropathy characterized by optic disk cupping and associated visual field loss patterns despite an otherwise unremarkable clinical examination; there is an absence of other known etiologies of open-angle glaucoma (OAG). Elevated IOP is a key modifiable risk factor.
Etiology
Not clearly established. Abnormalities of perfusion, ganglion cell metabolism, and/or mechanical factors are thought to play the central roles.
 Mechanical: Increased intraocular pressure directly compresses ganglion cell axons against the lamina cribrosa, interrupting axon function and leading to ganglion cell death.
Mechanical: Increased intraocular pressure directly compresses ganglion cell axons against the lamina cribrosa, interrupting axon function and leading to ganglion cell death.
 Ischemic: Abnormalities of the optic nerve head microvascular circulation, stressed by increased pressure or vessel compromise by lamina cribrosa plate distortion, leads to ganglion cell death.
Ischemic: Abnormalities of the optic nerve head microvascular circulation, stressed by increased pressure or vessel compromise by lamina cribrosa plate distortion, leads to ganglion cell death.
 Neurotoxicity: Astrocytes or other CNS support cells may become dysfunctional resulting in disrupted axoplasmic transport, direct neurotoxicity from nitric oxide or TNF-α, and/or disruption of the neurotrophic extracellular matrix necessary to sustain ganglion cell function.
Neurotoxicity: Astrocytes or other CNS support cells may become dysfunctional resulting in disrupted axoplasmic transport, direct neurotoxicity from nitric oxide or TNF-α, and/or disruption of the neurotrophic extracellular matrix necessary to sustain ganglion cell function.
 A direct relationship between IOP and existing/subsequent optic nerve damage has been established.
A direct relationship between IOP and existing/subsequent optic nerve damage has been established.
Signs and Symptoms
Usually asymptomatic.
Loss of peripheral visual field early in disease; central visual field loss later in course.
Genetics
 Multifactorial inheritance with lack of penetrance and variable expressivity.
Multifactorial inheritance with lack of penetrance and variable expressivity.
 First-degree relatives of glaucoma patients are at increased risk: 10% for siblings and 4% for offspring. Twenty-five percent of new cases of POAG have positive family history.
First-degree relatives of glaucoma patients are at increased risk: 10% for siblings and 4% for offspring. Twenty-five percent of new cases of POAG have positive family history.
 Juvenile-onset glaucoma has been isolated to chromosome 1q. This form of juvenile-onset glaucoma is inherited as an atuosomal dominant trait. This gene has also been linked to some adult forms of open-angle glaucoma.
Juvenile-onset glaucoma has been isolated to chromosome 1q. This form of juvenile-onset glaucoma is inherited as an atuosomal dominant trait. This gene has also been linked to some adult forms of open-angle glaucoma.
 Inherited form of glaucoma associated with aniridia: mutation in the PAX6 gene located at 11p13. Sporadic form of aniridia associated with development of Wilms tumor.
Inherited form of glaucoma associated with aniridia: mutation in the PAX6 gene located at 11p13. Sporadic form of aniridia associated with development of Wilms tumor.
Demographics
Occurs in 1.3% to 2.1% of general population over 40 years old.
Incidence increases with aging.
Estimates: 1 in 10 elderly blacks and 1 in 50 elderly whites (four to five times more prevalent in blacks).
Primary Risk Factors
 Family history
Family history
 Age
Age
 Race
Race
 Increased IOP
Increased IOP
 Central Corneal Thickness (CCT)
Central Corneal Thickness (CCT)
Ophthalmic Findings
Bilateral (may be asymmetric).
Increased IOP (usually >22 mm Hg).
Gonioscopy: angle open, without visible pathologic features.
Optic disk:
Increased c/d ratio; asymmetry to fellow eye.
Asymmetry of the neuroretinal rim.
Focal thinning of the neuroretinal rim: “notching.”
Optic disk splinter hemorrhage (Figure 5.6).
Vertical elongation of cup.
Retinal nerve fiber layer (NFL) loss.
Associated Ophthalmic Disorders
Increased incidence of central retinal vein occlusion in patients with glaucoma or OHTN.
Increased incidence of myopia (may be selection bias).
Systemic Findings
Increased prevalence of both elevated mean IOP and POAG in patients with diabetes mellitus. Diabetes as an independent risk factor for POAG remains controversial. Weak association exists between POAG and cardiovascular disease (hypertension, ischemic factors).
Special Tests
Gonioscopy: to rule out secondary causes, verify open angle.
Central corneal thickness (pachymetry): affects IOP measurements by all applanation methods.
Red-free illumination: to visualize NFL defects.
Diurnal IOP readings: to rule out spurious low IOP reading.
Automated visual field: to quantitatively evaluate visual field status.
Tonography: to measure relative outflow facility.
Blue-yellow perimetry (also known as short-wavelength automated perimetry, or SWAP): thought to detect visual field loss earlier. Projects a blue stimulus onto a yellow background, thereby isolating koniocellular, blue/yellow ganglion cells.
Frequency-doubling technology (FDT) perimetry: also thought to detect visual field loss earlier, it employs low spatial frequency sinusoidal grating undergoing rapid phase-reversal flicker. Isolates magnocellular cells.
Pathology
 Ganglion cell death (cells at inferior or superior aspect of disk appear to be more susceptible).
Ganglion cell death (cells at inferior or superior aspect of disk appear to be more susceptible).
 Increased c/d ratio; loss of neuroretinal rim.
Increased c/d ratio; loss of neuroretinal rim.
 Electron microscopy: decreased celluarity of TM and “extracellular plaques” in TM.
Electron microscopy: decreased celluarity of TM and “extracellular plaques” in TM.
Disease Course
 Insidious, painless, slowly progressive.
Insidious, painless, slowly progressive.
 Nonreversible visual field loss; only rare instances of reversal of cupping.
Nonreversible visual field loss; only rare instances of reversal of cupping.
 Optic disk changes may be observed before visual field changes.
Optic disk changes may be observed before visual field changes.
Treatment and Management
 Lowering IOP is the only proven modifiable risk factor for preventing future disk damage and progressive visual field loss.
Lowering IOP is the only proven modifiable risk factor for preventing future disk damage and progressive visual field loss.
 Stereo photographs: to detect subtle changes in disk over time.
Stereo photographs: to detect subtle changes in disk over time.
 Computerized imaging: provides a topographical map of disk for a more quantitative analysis.
Computerized imaging: provides a topographical map of disk for a more quantitative analysis.
 Periodic evaluation of visual fields: to assess treatment results.
Periodic evaluation of visual fields: to assess treatment results.
 Correlate visual field changes with optic disk changes.
Correlate visual field changes with optic disk changes.
 “Target pressure” concept: Consistently achieve 25% to 66% of presenting IOP to limit further visual field loss (dependent on severity of glaucoma); continue to monitor visual field and disk changes even at target IOP for effectiveness of treatment, no matter how low the current IOP.
“Target pressure” concept: Consistently achieve 25% to 66% of presenting IOP to limit further visual field loss (dependent on severity of glaucoma); continue to monitor visual field and disk changes even at target IOP for effectiveness of treatment, no matter how low the current IOP.
 “Glaucoma suspect” concept: patients who have high IOP or glaucomatous-appearing disks, but without corresponding visual field loss. There is no clear consensus on when or how to treat ocular hypertensives who do not have glaucomatous disks or visual field loss. A personalized assessment of risk factors and patient goals must guide treatment decisions. In general, initiate therapy if IOP is greater than 30 mm Hg, and lower than that if risk factors or evidence of glaucomatous optic nerve damage is present.
“Glaucoma suspect” concept: patients who have high IOP or glaucomatous-appearing disks, but without corresponding visual field loss. There is no clear consensus on when or how to treat ocular hypertensives who do not have glaucomatous disks or visual field loss. A personalized assessment of risk factors and patient goals must guide treatment decisions. In general, initiate therapy if IOP is greater than 30 mm Hg, and lower than that if risk factors or evidence of glaucomatous optic nerve damage is present.
 There is no known “cure”: The visual field loss is irreversible and the treatments have undesired effects. Therefore, the goal is to preserve visual field adequate for patient’s lifetime and visual demands.
There is no known “cure”: The visual field loss is irreversible and the treatments have undesired effects. Therefore, the goal is to preserve visual field adequate for patient’s lifetime and visual demands.
Medications
β-Blockers.
CAI inhibitors.
Prostaglandin analogues.
Adrenergic agonists.
Cholinergic agents.
Laser Surgery Indications
 Use laser trabeculoplasty in mild to moderate glaucoma.
Use laser trabeculoplasty in mild to moderate glaucoma.
 Effect may be temporary.
Effect may be temporary.
Filtration Surgery Indications (General Concepts)
 Progressive visual field loss or optic disk changes despite maximum tolerated medical therapy.
Progressive visual field loss or optic disk changes despite maximum tolerated medical therapy.
 Sustained highly elevated IOP (i.e., >40 mm Hg), even if without visual field loss or optic disk changes.
Sustained highly elevated IOP (i.e., >40 mm Hg), even if without visual field loss or optic disk changes.
 Advanced visual field loss (small margin for tolerating further damage [i.e., loss progressing to fixation]).
Advanced visual field loss (small margin for tolerating further damage [i.e., loss progressing to fixation]).
Follow-Up
 Per specific case; at least every 6 months for IOP check.
Per specific case; at least every 6 months for IOP check.
 Recently diagnosed patients need repeated visual field tests in order to rule out learning artifact, and frequent visits to establish satisfactory IOP control.
Recently diagnosed patients need repeated visual field tests in order to rule out learning artifact, and frequent visits to establish satisfactory IOP control.
 Up to 50% of patients with glaucoma (all types) have an initial screening IOP of less than 21 mm Hg.
Up to 50% of patients with glaucoma (all types) have an initial screening IOP of less than 21 mm Hg.
 Establish consistency of visual field test-taking parameters.
Establish consistency of visual field test-taking parameters.
Differential Diagnosis
Normal tension glaucoma: identical disease to POAG but patient never has documented IOP greater than 22 mm Hg.
Chronic/intermittent angle-closure glaucoma: peripheral anterior synechiae, occludable angles, symptoms, episodic IOP elevations.
Exfoliation glaucoma: anterior lens capsule changes, pupillary margin transillumination defects.
Pigmentary glaucoma: Krukenberg spindle, heavy deposition of pigment on TM, midperipheral iris transillumination defects, symptomatic with exercise or mydriasis.
Other optic neuropathies are generally nonprogressive and show no cupping of the optic disk.
Reference
Booth A, Churchill A, Anwar R, et al. The genetics of primary open angle glaucoma. Br J Ophthalmol 1997;81:409–414.
Normal Tension Glaucoma
Summary
Normal tension glaucoma (NTG) is a progressive optic neuropathy with typical glaucomatous optic disk damage and visual field loss with open angles as in POAG. However, the IOP is consistently less than 22 mm Hg. Also known as “low tension glaucoma” (LTG), it is probably a subset of POAG.
Etiology
Not well established. Thought to be due to relatively IOP-independent mechanisms such as microvascular damage; although not considered the main pathogenic factor, IOP has been established as a significant modifier of future disk damage and visual field loss.
Signs and Symptoms
Asymptomatic, visual field loss apparent later in natural history.
Demographics
Typically in elderly patients (over age 70 years).
No established racial predilection.
Ophthalmic Findings
Identical to POAG, except that IOP is normal.
When compared with POAG:
Visual field defects tend to be steeper, deeper, and closer to fixation.
Increased incidence of optic disk splinter hemorrhages.
Systemic Findings
Possible relationship to history of hypotensive shock, postural hypotension, migraines.
Special Tests
Diurnal IOP curve to rule out spurious low IOP reading.
Pathology
Obscure/undetermined but shares final common pathway of ganglion cell death.
Disease Course
Progressive nature is key characteristic. Some will have progressive damage despite very low IOPs.
Treatment and Management
 Progression of disease (further visual field loss or disk changes) should be documented before diagnosis and initiation of therapy.
Progression of disease (further visual field loss or disk changes) should be documented before diagnosis and initiation of therapy.
 The only current therapeutic strategy is to lower IOP further.
The only current therapeutic strategy is to lower IOP further.
Medications
Same as for POAG.
Follow-Up
Same as for POAG.
Differential Diagnosis
POAG with diurnal variation: on diurnal IOP curve testing has peaks in IOP greater than 22 mm Hg.
Angle-closure glaucoma (intermittent or chronic): has suggestive history, symptoms, features of occludable angle in both eyes, episodes of elevated IOP.
Previous glaucoma damage: burned-out pigmentary glaucoma, history (key feature of NTG diagnosis is progressive nature of visual field loss and disk changes despite “normal” IOP).
Nonglaucomatous optic neuropathy: nonprogressive (i.e., always inquire about a severe hypotensive episode such as massive blood loss during surgery that may explain a stable visual field loss).
Congenital optic nerve defect: nonprogressive.
Traumatic glaucoma: Previous eye trauma (usually blunt) may lead to dysfunction of TM and aqueous outflow compromise. The relative magnitude of the trauma may be implied by findings such as angle recession (though the angle recession itself may not be directly responsible for aqueous outflow compromise).
Reference
Grosskreutz C, Netland PA. Low-tension glaucoma. Int Ophthalmol Clin 1994;34:173–185.
Pigment Dispersion Syndrome and Pigmentary Glaucoma
Pigment dispersion syndrome (PDS) is characterized by spokelike midperipheral iris pigment epithelial thinning with pigment deposition on the corneal endothelium, TM, and lens periphery. If associated with consistently high IOP, visual field loss, and glaucomatous optic disk damage: “pigmentary glaucoma,” a type of secondary open-angle glaucoma (SOAG).
Etiology
 Pigment dispersion is thought to be caused by direct mechanical contact between the anterior lens zonules and iris pigment epithelium.
Pigment dispersion is thought to be caused by direct mechanical contact between the anterior lens zonules and iris pigment epithelium.
 Blinking is theorized to create a stop-valve effect by increasing AC pressure relative to PC pressure (and thus the reverse pupillary block configuration of the iris).
Blinking is theorized to create a stop-valve effect by increasing AC pressure relative to PC pressure (and thus the reverse pupillary block configuration of the iris).
Signs and Symptoms
Asymptomatic.
Episodic blurring, halos, and possible ocular pain (due to acute rises in IOP associated with exercise or mydriasis).
Demographics
Associated with moderate myopia.
Increased incidence in male patients.
Usually 20 to 50 years of age.
Whites (rare in blacks).
Approximately 25% to 50% of PDS patients progress to pigmentary glaucoma.
Ophthalmic Findings
 Krukenberg spindle: vertical pattern of pigment deposition on corneal endothelium.
Krukenberg spindle: vertical pattern of pigment deposition on corneal endothelium.
 Open angle with dense, homogeneously pigmented TM (Figure 5.10).
Open angle with dense, homogeneously pigmented TM (Figure 5.10).
 Sampaolesi line: pigment deposition anterior to Schwalbe’s line.
Sampaolesi line: pigment deposition anterior to Schwalbe’s line.
 Iris transillumination defects: spokelike loss of pigment at iris midperiphery. In pseudophakes, the pattern follows the optic and haptic implant edges.
Iris transillumination defects: spokelike loss of pigment at iris midperiphery. In pseudophakes, the pattern follows the optic and haptic implant edges.
 Pigment “dusting” on iris surface.
Pigment “dusting” on iris surface.
 Pigmented cells in AC after dilation.
Pigmented cells in AC after dilation.
 Scheie stripe: pigment on lens capsule at zonule attachment site.
Scheie stripe: pigment on lens capsule at zonule attachment site.
 Large fluctuations in IOP (sudden large IOP elevation is observed following exercise or dilation).
Large fluctuations in IOP (sudden large IOP elevation is observed following exercise or dilation).
 Iris contour concavity is frequently observed (“Q” configuration in the Spaeth classification).
Iris contour concavity is frequently observed (“Q” configuration in the Spaeth classification).
 Nearly always bilateral.
Nearly always bilateral.
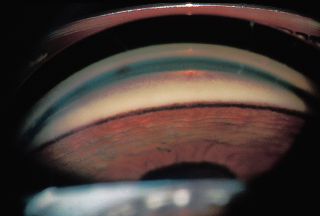
FIGURE 5.10. Pigment dispersion syndrome. The heavily pigmented meshwork band is evident.
Special Tests
Ultrasound biomicroscopy (UBM) confirms iris anatomic configuration of reverse pupillary block (“Q” shape).
Pathology
Direct dispersion of pigment into TM leads to degeneration of TM cells, trapping of cellular debris, and sclerosis of TM beams.
Disease Course
 In one study, 35% of patients with PDS and elevated IOP developed visual field loss or optic disk cupping (mean follow-up of 17 years).
In one study, 35% of patients with PDS and elevated IOP developed visual field loss or optic disk cupping (mean follow-up of 17 years).
 Signs and symptoms may decrease as patient ages.
Signs and symptoms may decrease as patient ages.
Treatment and Management
 PDS with normal optic disks, visual fields, and IOP: Follow as a glaucoma suspect.
PDS with normal optic disks, visual fields, and IOP: Follow as a glaucoma suspect.
 If glaucomatous changes develop, treat medically as in POAG.
If glaucomatous changes develop, treat medically as in POAG.
 Laser trabeculoplasty has good efficacy in these patients if medications are not effective.
Laser trabeculoplasty has good efficacy in these patients if medications are not effective.
 Laser iridotomy is indicated if reverse pupillary block component is observed (usually considered in young patients).
Laser iridotomy is indicated if reverse pupillary block component is observed (usually considered in young patients).
Medications
 Same as for POAG.
Same as for POAG.
 Miotics have been shown to reduce iris transillumination defects and pigment dispersion.
Miotics have been shown to reduce iris transillumination defects and pigment dispersion.
Follow-Up
Patients with PDS are followed as glaucoma suspects.
Differential Diagnosis
Exfoliation syndrome/glaucoma: seen in older patients, pupillary margin iris defects, anterior lens capsule changes. Less dense pigment deposition, no symptoms.
POAG: no iris transillumination defects, less abundant pigment deposition, asymptomatic, older patients.
Inflammatory open-angle glaucoma: Nonpigmented cells and aqueous flare present, iris transillumination may be present.
Iris melanoma: has iris mass, very heavy pigment deposition.
Reference
Migliazzo CV, Shaffer RN, Nykin R, et al. Long-term analysis of pigmentary dispersion syndrome and pigmentary glaucoma. Ophthalmology 1986;93:1528–1536.
Exfoliation syndrome or pseudoexfoliation (XS) is characterized by the deposition of a distinctive fibrillar material throughout the anterior segment, in particular, on the anterior lens surface. If associated with glaucoma, it is termed “exfoliative glaucoma” (XG), formerly called pseudoexfoliative glaucoma (PXG). This is in distinction to “true exfoliation” (i.e., that classically associated with glass blowing), which is now called “capsular exfoliation.”
Etiology
A manifestation of a generalized basement disorder, the deposition of fibrillar material occludes the TM and thus compromises aqueous outflow.
Signs and Symptoms
Rarely symptomatic.
Patients may complain of foreign body sensation.
Demographics
 Varies considerably with population studied: XG accounts for greater than 50% of OAG cases in Scandanavian countries but for only 1.6% of OAG cases in the southeastern United States.
Varies considerably with population studied: XG accounts for greater than 50% of OAG cases in Scandanavian countries but for only 1.6% of OAG cases in the southeastern United States.
 Rarely seen in patients less than 50 years of age; most patients are more than 70 years old.
Rarely seen in patients less than 50 years of age; most patients are more than 70 years old.
Ophthalmic Findings
 Corneal endothelium pigment deposition: usually diffuse, may rarely be in Krukenberg spindle pattern.
Corneal endothelium pigment deposition: usually diffuse, may rarely be in Krukenberg spindle pattern.
 Iris transillumination defects: “moth-eaten” iris appearance at pupillary margin (Figure 5.11); may be easier to observe with mydriasis.
Iris transillumination defects: “moth-eaten” iris appearance at pupillary margin (Figure 5.11); may be easier to observe with mydriasis.
 Pigment deposition on iris anterior surface.
Pigment deposition on iris anterior surface.
 Diffuse spotty pigmentation throughout angle; pigmentation anterior to Schwalbe’s line (Sampaolesi line) is frequently present.
Diffuse spotty pigmentation throughout angle; pigmentation anterior to Schwalbe’s line (Sampaolesi line) is frequently present.
 The anterior lens characteristically has a target pattern: A clear intervening area separates a central translucent zone from a peripheral area of granular deposition (best seen with mydriasis). The clear intervening zone is thought to be secondary to rubbing of the iris on the anterior lens capsule (Figure 5.12).
The anterior lens characteristically has a target pattern: A clear intervening area separates a central translucent zone from a peripheral area of granular deposition (best seen with mydriasis). The clear intervening zone is thought to be secondary to rubbing of the iris on the anterior lens capsule (Figure 5.12).
 Increased incidence of phacodonesis, lens subluxation, and increased risk of vitreous loss with cataract surgery attributable to weakened lens zonules.
Increased incidence of phacodonesis, lens subluxation, and increased risk of vitreous loss with cataract surgery attributable to weakened lens zonules.
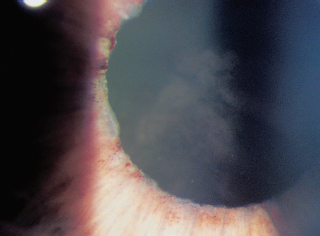
FIGURE 5.11. Exfoliation syndrome. The pupillary border of the iris may have a “moth-eaten” appearance.
Systemic Findings
Identical basement membrane findings throughout body: of no known consequence.
Pathology
 A primary basement membrane disorder.
A primary basement membrane disorder.
 Exfoliative material histochemically resembles elastic microfibrils and other extracellular matrix components.
Exfoliative material histochemically resembles elastic microfibrils and other extracellular matrix components. Obstruction of TM by pseudoexfoliative material and/or underlying TM dysfunction leads to compromised aqueous outflow.
Obstruction of TM by pseudoexfoliative material and/or underlying TM dysfunction leads to compromised aqueous outflow.

FIGURE 5.12. Target-shaped deposition of exfoliative material on the anterior lens capsule. The intervening clear zone is thought to be due to iridolenticular rubbing.
Disease Course
 In an eye with XS and normal IOP, there is a 5.3% and a 15.4% chance of developing disk or field changes at 5 and 10 years, respectively.
In an eye with XS and normal IOP, there is a 5.3% and a 15.4% chance of developing disk or field changes at 5 and 10 years, respectively.
 In an eye with XS and elevated IOP, there is a 35% chance of developing disk or field damage in 9 years (vs. 18% of ocular hypertensives).
In an eye with XS and elevated IOP, there is a 35% chance of developing disk or field damage in 9 years (vs. 18% of ocular hypertensives).
 XG has a worse prognosis than POAG, frequently responding poorly to medical therapy and more likely to lead to development of visual field loss (48% vs. 19% for POAG).
XG has a worse prognosis than POAG, frequently responding poorly to medical therapy and more likely to lead to development of visual field loss (48% vs. 19% for POAG).
Treatment and Management
 Approach is similar to POAG.
Approach is similar to POAG.
 Increased incidence of cataract extraction complications, since zonular weakness may lead to zonular dehiscence, tears in posterior capsule, vitreous loss, dropped nucleus.
Increased incidence of cataract extraction complications, since zonular weakness may lead to zonular dehiscence, tears in posterior capsule, vitreous loss, dropped nucleus.
 Lens extraction does not alleviate findings or alter disease course.
Lens extraction does not alleviate findings or alter disease course.
 Laser trabeculoplasty can be very effective with good uptake by pigmented TM, but there is shorter duration of response when compared to POAG.
Laser trabeculoplasty can be very effective with good uptake by pigmented TM, but there is shorter duration of response when compared to POAG.
 Trabeculectomy results are similar when compared to patients with POAG, but these patients have increased postoperative inflammation.
Trabeculectomy results are similar when compared to patients with POAG, but these patients have increased postoperative inflammation.
Medications
Same as for POAG, although generally less effective.
Follow-Up
XS patients are at increased likelihood of developing glaucomatous damage and therefore must be followed closely as glaucoma suspects.
Differential Diagnosis
PDS/pigmentary glaucoma: younger patients with midperipheral iris transillumination defects, more abundant pigmentary deposition on TM and cornea, lack of anterior lens capsule changes.
Capsular exfoliation (also known as capsular delamination, “true exfoliation”): history of glass blowing or welding.
Toxic exfoliation (uveitis and retained foreign body): symptoms, inflammation, and history of trauma.
References
Henry JC, Krupin T, Schmitt M, et al. Long-term follow-up of pseudoexfoliation and the development of elevated intraocular pressure. Ophthalmology 1987;94:545–552.
Kozart DM, Yanoff M. Intraocular pressure status in 100 consecutive patients with exfoliation syndrome. Ophthalmology 1982;89:214–218.
Naumann GO, Schlotzer-Schrehardt U, Kuchle M. Pseudoexfoliation syndrome for the comprehensive ophthalmologist: intraocular and systemic manifestations. Ophthalmology 1998;105:951–968.
Pohjanpelto P. Influence of exfoliation syndrome on prognosis in ocular hypertension >25 mm Hg: a long-term follow-up. Acta Ophthalmol 1986;64:39–44.
Primary Angle-Closure Glaucoma
Primary angle-closure glaucoma (PACG) is acute, chronic, or intermittent elevation of IOP as a result of mechanical blockage of the TM by the iris root, without underlying secondary etiology (only anatomic predisposition). Identical glaucomatous optic neuropathy damage to POAG.
Etiology
PACG with pupillary block: Flow of aqueous humor from PC through pupil and into AC is limited anatomically; therefore aqueous humor accumulates in the PC. This creates a relative pressure gradient (high pressure in the PC and low in the AC), forcing the iris root to take a relatively anterior position and leading to angle narrowing or closure. Pupillary block may be absolute (i.e., posterior synechiae that totally obstruct aqueous flow into AC) or relative (i.e., anatomic factors create a pressure gradient). This is by far the most frequent etiology of PACG.
PACG without pupillary block (“plateau iris configuration”): an increasingly recognized anatomic variant, caused by relatively anteriorly positioned ciliary processes that create an anteriorly positioned iris root with planar configuration centrally. Plateau iris cannot be diagnosed with certainty until any possible pupillary block component is relieved with peripheral iridotomy.
Signs and Symptoms
 Acute angle closure (sudden, rapid increase in IOP):
Acute angle closure (sudden, rapid increase in IOP):
Painful, red, congested, “steamy” eye.
Nausea and vomiting (has been misdiagnosed as an acute condition of the abdomen).
Blurred vision.
Rainbow-colored halos around lights.
 Intermittent (angle opens and closes spontaneously):
Intermittent (angle opens and closes spontaneously):
Transient blurry vision, halos, and/or headaches secondary to acute rises in IOP; IOP is normal between episodes.
Episodes occur over days or weeks.
 Chronic (progressive angle closure):
Chronic (progressive angle closure):
May be asymptomatic.
IOP may gradually rise over time.
Course may resemble POAG.
Demographics
 In a population over 40 years of age, PACG prevalence is 0.1% to 0.6% in whites, 0.1% to 0.2% in blacks, 2.1% to 5.0% in the Inuit, 0.4% to 1.4% in East Asians, 0.3% in Japanese, and 2.3% in a mixed ethnic group in South Africa.
In a population over 40 years of age, PACG prevalence is 0.1% to 0.6% in whites, 0.1% to 0.2% in blacks, 2.1% to 5.0% in the Inuit, 0.4% to 1.4% in East Asians, 0.3% in Japanese, and 2.3% in a mixed ethnic group in South Africa.
 Highly prevalent in Eskimos and eastern Asians (studies have suggested that PACG accounts for 70% of all glaucoma cases in China).
Highly prevalent in Eskimos and eastern Asians (studies have suggested that PACG accounts for 70% of all glaucoma cases in China).
 Two to four times more prevalent in female than in male patients, regardless of race.
Two to four times more prevalent in female than in male patients, regardless of race.
 Small, hyperopic eyes are at increased risk.
Small, hyperopic eyes are at increased risk.
Ophthalmic Findings
 Acute:
Acute:
High IOP (40 to 80 mm Hg).
Middilated, sluggish, often irregular pupil.
Corneal edema.
Congested episcleral and conjunctival blood vessels.
Shallow AC.
AC cell and flare.
May have optic disk swelling.
 Intermittent:
Intermittent:
Peripheral anterior synechiae.
During episodes, findings resemble acute ACG.
 Chronic:
Chronic:
PAS.
During episodes, findings resemble acute ACG.
The most frequent newly diagnosed ocular disease when glaucoma specialist enters region without prior glaucoma specialist care.
 “Glaukomflecken” are characteristic white anterior capsular opacities that represent focal necrotic lens epithelium remaining from prior angle-closure episodes.
“Glaukomflecken” are characteristic white anterior capsular opacities that represent focal necrotic lens epithelium remaining from prior angle-closure episodes.
 Gonioscopy of fellow eye shows a similar narrow, occludable angle.
Gonioscopy of fellow eye shows a similar narrow, occludable angle.
Systemic Findings
Patients may present with abdominal pain, nausea, and vomiting in acute episodes.
Special Tests
 Compression gonioscopy to differentiate appositional from synechial angle closure (use Zeiss or Volk or Sussman four-mirror lens; Goldman three-mirror is inadequate for this test, since its large area of ocular contact suctions and distorts angle features).
Compression gonioscopy to differentiate appositional from synechial angle closure (use Zeiss or Volk or Sussman four-mirror lens; Goldman three-mirror is inadequate for this test, since its large area of ocular contact suctions and distorts angle features).
 Provocative mydriatic test: compare predilation IOP with postdilation IOP. This is of controversial predictive value; an increase of 8 mm Hg is considered the upper limit of normal.
Provocative mydriatic test: compare predilation IOP with postdilation IOP. This is of controversial predictive value; an increase of 8 mm Hg is considered the upper limit of normal.
 DRPPT: Measure IOP in the maximum physiologic conditions that could precipitate angle closure (compare IOPs recorded at same body position).
DRPPT: Measure IOP in the maximum physiologic conditions that could precipitate angle closure (compare IOPs recorded at same body position).
 Anterior segment OCT and UBM may be useful in delineating the degree of angle closure in differing lighting conditions.
Anterior segment OCT and UBM may be useful in delineating the degree of angle closure in differing lighting conditions.
Pathology
Ganglion cell death similar to that seen in POAG.
Disease Course
 Depends on acute, intermittent, or chronic characteristics.
Depends on acute, intermittent, or chronic characteristics.
 In cases of acute angle closure, the untreated fellow eye has a 40% to 80% chance of developing acute angle closure over next 5 to 10 years. Prophylactic medical therapy with miotics does not significantly alter this course.
In cases of acute angle closure, the untreated fellow eye has a 40% to 80% chance of developing acute angle closure over next 5 to 10 years. Prophylactic medical therapy with miotics does not significantly alter this course.
 “Mixed mechanism glaucoma”: PACG leads to TM dysfunction and thus POAG-like disease course even after angle is anatomically reopened.
“Mixed mechanism glaucoma”: PACG leads to TM dysfunction and thus POAG-like disease course even after angle is anatomically reopened.
Treatment and Management
The definitive treatment is laser or surgical peripheral iridotomy (PI).
 Methods to facilitate laser PI:
Methods to facilitate laser PI:
Pretreat with argon laser, then Nd:YAG laser to open PI.
A sectoral pupilloplasty peaks the pupil or laser iridoplasty may relieve some pupillary block component (less congestion).
If attack broken medically, may wait until next day to perform PI, when less congestion is present.
 May need to reduce the IOP with other topical or systemic medications first, then use cholinergics.
May need to reduce the IOP with other topical or systemic medications first, then use cholinergics.
 Globe compression (compression onto central portion of cornea only, since the goal is to force aqueous peripherally and open angle).
Globe compression (compression onto central portion of cornea only, since the goal is to force aqueous peripherally and open angle).
 Surgical paracentesis in extreme cases.
Surgical paracentesis in extreme cases.
 Prophylactic laser iridotomy of contralateral eye (assuming similar anatomy) is highly recommended to decrease risk of future angle closure.
Prophylactic laser iridotomy of contralateral eye (assuming similar anatomy) is highly recommended to decrease risk of future angle closure.
 Lensectomy/cataract extraction may need to be undertaken if the above treatments fail.
Lensectomy/cataract extraction may need to be undertaken if the above treatments fail.
Medications
First, combination therapy with topical β-blockers, α2-agonists, CAIs, prostaglandin analogues, and/or hyperosmotic systemic agents (e.g., mannitol). The goal is to relieve congestion until definitive therapy can be performed. Pilocarpine 1% may break mild attacks by inducing miosis which pulls peripheral iris away from the TM. However, it is often ineffective when pressure is high due to pupillary sphincter ischemia. Stronger miotics should be avoided and may, in fact, precipitate angle closure by advancing lens-iris diaphragm anteriorly. Nonselective adrenergic agonists (apraclonidine) should also be avoided due to vasoconstriction effects as this could worsen iris ischemia.
Follow-up
 Miotic therapy in fellow eye until prophylactic PI can be performed.
Miotic therapy in fellow eye until prophylactic PI can be performed.
 There is a greater than 50% chance of developing angle closure in the fellow eye.
There is a greater than 50% chance of developing angle closure in the fellow eye.
Differential Diagnosis
Always examine contralateral eye for narrow occludable angles, a key feature of PACG.
Secondary angle-closure glaucoma (SACG): Another ophthalmic disorder is identifiable as the etiology (see next section); the contralateral angle is nonoccludable.
Inflammatory open-angle glaucoma (glaucomatocyclitic crisis, Posner-Schlossman syndrome): has a more prominent component of aqueous inflammation; the contralateral eye has an open angle.
Traumatic glaucoma: history, angle recession, PAS.
POAG: no history or features of angle closure seen.
SOAG: angle is open; pigmentary or pseudoexfoliative features seen.
References
2007–2008 Basic and Clinical Science Course (BCSC), Section 10: Glaucoma. American Academy of Ophthalmology, San Francisco, 2007.
Erie JC, Hodge DO, Gray DT. The incidence of primary angle-closure glaucoma in Olmstead County, Minnesota. Arch Ophthalmol 1997;115:177–181.
Kim YY, Jung HR. Clarifying the nomenclature for primary angle-closure glaucoma. Surv Ophthalmol 1997;42:125–136.
Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol 2006;90: 262–267.
Wilensky JT, Ritch R, Kolker AE. Should patients with anatomically narrow angles have prophylactic iridectomy? Surv Ophthalmol 1996;41:31–36.
Secondary Angle-Closure Glaucoma
A variety of ocular disorders may precipitate angle closure. Identifying and treating the underlying primary disorder is the definitive management. When both open-angle and closed-angle pathogenetic mechanisms are present (simultaneously or consecutively): “combined mechanism glaucoma.”
There are two basic mechanisms of secondary angle closure:
 Iris root “pushed” anteriorly to close angle:
Iris root “pushed” anteriorly to close angle:
Lens-related.
Miotics.
Posterior segment masses or tumors.
Ciliary body swelling, choroidal effusion/hemorrhage, or ciliary-block glaucoma.
 Iris root “pulled” anteriorly to close angle:
Iris root “pulled” anteriorly to close angle:
Neovascularization of angle.
Inflammation.
ICE syndrome.
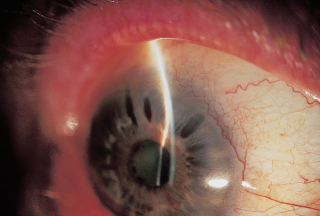
FIGURE 5.13. Iris bombe. Notice the anterior bowing of the iris and the apposition of the iris and cornea peripherally in the slit beam.
Etiology
 Anterior segment inflammation: may create posterior synechiae that adhere the iris pupillary margin to the lens, thus obstructing aqueous flow into the AC. The iris periphery then balloons outward in response to this increased pressure in the PC, creating an “iris bombe” configuration (Figure 5.13).
Anterior segment inflammation: may create posterior synechiae that adhere the iris pupillary margin to the lens, thus obstructing aqueous flow into the AC. The iris periphery then balloons outward in response to this increased pressure in the PC, creating an “iris bombe” configuration (Figure 5.13).
 Lens-induced glaucoma:
Lens-induced glaucoma:
“Phacomorphic glaucoma”: Enlargement of a hypermature lens may narrow the AC and precipitate angle closure.
Subluxed lens or microspherophakia may also cause angle closure.
AC intraocular lenses (IOLs) may occlude the pupil: Management is with PI and lens extraction as required.
 Postoperative flat AC: may lead to formation of PAS and permanent occlusion of angle.
Postoperative flat AC: may lead to formation of PAS and permanent occlusion of angle.
 Drug-Induced: Topiramate (Topamax) is an oral antiepileptic, antidepressant, and headache therapy that can cause an acute syndrome of bilateral myopic shift, uniformly shallow AC, and elevated IOP from acute angle closure. Mechanism is choroidal effusion that causes profound rotation of the lens-iris diaphragm.
Drug-Induced: Topiramate (Topamax) is an oral antiepileptic, antidepressant, and headache therapy that can cause an acute syndrome of bilateral myopic shift, uniformly shallow AC, and elevated IOP from acute angle closure. Mechanism is choroidal effusion that causes profound rotation of the lens-iris diaphragm.
 Epithelial and fibrous downgrowth:
Epithelial and fibrous downgrowth:
Occurs postoperatively when epithelium or other fibrovascular tissue migrates into the surgical wound and covers various anterior segment structures, including the TM.
Difficult to diagnose; flattened smooth-appearing iris surface that whitens with Argon laser treatment, but may need paracentesis specimen to confirm diagnosis (aqueous aspirate cytology).
 Miotics: may induce ACG by moving the lens-iris diaphragm anteriorly.
Miotics: may induce ACG by moving the lens-iris diaphragm anteriorly.
 Ocular trauma: may precipitate PAS formation and angle closure.
Ocular trauma: may precipitate PAS formation and angle closure.
 Neovascular glaucoma.
Neovascular glaucoma.
 ICE syndrome.
ICE syndrome. Posterior segment masses:
Posterior segment masses:
May mechanically force the lens-iris diaphragm anteriorly or stimulate angle neovascularization and thus close the angle (e.g., large ocular melanoma, large anterior uveal cysts).
Nonrhegmatogenous retinal detachments (RDs) may have an associated subretinal effusion or hemmorrhage that “pushes” the bullous RD anteriorly against the lens-iris diaphragm and thus narrows or closes the angle.
 Vitreoretinal disorders, other conditions:
Vitreoretinal disorders, other conditions:
Ciliary-block (“malignant”) glaucoma: Aqueous humor is misdirected posteriorly into vitreous space.
Following panretinal photocoagulation, there may be ciliary body thickening and an anterior choroidal detachment that forces the lens-iris diaphragm anteriorly.
Severe central retinal vein occlusion (CRVO) may cause swelling of the choroid and ciliary body and thus shallow the AC.
Retinopathy of prematurity (ROP) is associated with cicatrization of retrolental tissue.
Persistent hyperplastic primary vitreous (PHPV) angle closure may be secondary to cataract and contracture of the primary vitreous.
 Nanophthalmos:
Nanophthalmos:
Has all the classic anatomic features (microphthalmia, hyperopia, small corneal diameter, thick sclera, narrow angles) that are susceptible to angle closure.
High incidence of angle closure.
High incidence of uveal effusions with intraocular surgery, which push lens-iris diaphragm forward. Avoid pilocarpine which can worsen pupillary block. Prophylactic sclerotomies can be used in select cases to prevent choroidal effusions.
Reference
Greenidge KC. Angle-closure glaucoma. Int Ophthalmol Clin 1990;30:177–186.
Inflammatory Glaucoma
Uveitic Glaucoma
Summary
Ocular inflammation and uveitis can be associated with elevated IOP and glaucoma, which can involve an open or closed angle. Frequently, the cause of the inflammation is elusive (Table 5.1).
Table 5.1 Common causes of elevated intraocular pressure in acute uveitis
Etiology
 Open angle:
Open angle:
Trabecular obstruction with inflammatory cells, proteins, or other chemical mediatiors of the inflammatory process.
Trabeculitis.
 Closed angle (Figure 5.14):
Closed angle (Figure 5.14):
Synechial angle closure.
Pupillary block from posterior synechiae.
 Steroid induced.
Steroid induced.
Signs and Symptoms
Pain.
Blurred vision.
Photophobia.
Demographics
Uveitis affects a wide variety of patients, depending on the specific disease entity.
Ophthalmic Findings
Anterior segment cells, aqueous flare, keratic precipitates.
Conjunctival hyperemia.
Keratitis.
Anterior and posterior synechiae.
Iris bombe.
Cataract.
Posterior segment inflammation (retinitis, vasculitis, choroiditis).
Macular edema.
Optic disk edema.
Sterile hypopyon.
Elevated IOP.
Systemic Findings
Arthritis (JRA, HLA-B27).
Skin lesions (herpes zoster, Behçet syndrome, Vogt-Koyanagi-Harada [VKH] syndrome, Lyme disease, sarcoid).
Pulmonary nodules (sarcoid).
Special Tests
HLA typing (HLA-B27).
Angiotensin-converting enzyme (ACE) and lysozyme.
Purified protein derivative (PPD) skin test.
Fluorescent treponemal antibody, absorbed (FTA-Abs) and Venereal Disease Research Laboratory (VDRL).
Antinuclear antibody (ANA).
Erythrocyte sedimentation rate (ESR).
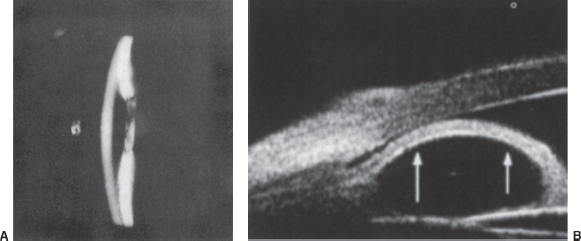
FIGURE 5.14. A, B: Posterior synechiae at the pupillary margin prevent aqueous from entering the anterior chamber, resulting in iris bombe and angle closure. (Courtesy of Joel S. Schuman, MD.)
Pathology
Tissues involved show signs of acute or chronic inflammation. Specific pathologic changes are highly dependent on disease entity.
Disease Course
 Acute process generally resolves within several months, but the glaucoma can linger if there are structural changes.
Acute process generally resolves within several months, but the glaucoma can linger if there are structural changes.
 Chronic uveitis and its sequelae can last several weeks to years and typically return after a quiescent period. The glaucoma can accompany acute exacerbations or remain as a result of chronic damage to outflow structures.
Chronic uveitis and its sequelae can last several weeks to years and typically return after a quiescent period. The glaucoma can accompany acute exacerbations or remain as a result of chronic damage to outflow structures.
Treatment and Management
 Treat underlying cause of uveitis.
Treat underlying cause of uveitis.
 Medical management of glaucoma.
Medical management of glaucoma.
 Surgical management of glaucoma (includes peripheral iridectomy, filtering procedures, ciliary body ablation, and aqueous shunt procedures).
Surgical management of glaucoma (includes peripheral iridectomy, filtering procedures, ciliary body ablation, and aqueous shunt procedures).
Medications
1. Inflammation is treated with steroids (topical, subconjunctival, or systemic) and in severe cases with cytotoxic immunosuppressive agents.
2. Bacterial, viral, and parasitic causes are treated with appropriate antimicrobials.
3. Cycloplegic agents (atropine, scopolamine, phenylephrine) are used to break synechiae, treat ciliary pain, and stabilize the blood–aqueous barrier.
4. Glaucoma medications include β-blockers, α-agonists, and topical or oral CAIs. Miotics may cause breakdown of the blood–aqueous barrier and worsening of synechiae. Prostaglandins theoretically may worsen inflammation but are administered in very small concentrations. Prostaglandin analogues can also reactivate dendritic HSV keratitis or keratouveitis.
Follow-Up
Follow-up depends on the disease entity, but frequent visits are needed to assess IOP and inflammation.
Differential Diagnosis
Steroid-induced glaucoma: Elevated IOP can result from steroid treatment for ocular inflammation. The glaucoma usually remits following cessation of the steroids. Patients with POAG are more frequently steroid responders, and it may be difficult to separate the steroid effect from the primary glaucoma.
Reference
Moorthy RS, Mermoud A, Baerveldt G, et al. Glaucoma associated with uveitis. Surv Ophthalmol 1997;41:361–394.
Glaucomatocyclitic Crisis (Posner-Schlossman Syndrome)
Summary
This syndrome is an idiopathic open-angle inflammatory glaucoma occurring in young to middle-aged adults. It is typically unilateral and acute.
Etiology
 Actual pathogenesis is unknown but has been postulated to be due to an idiopathic trabeculitis. Herpesvirus infection has also been suggested.
Actual pathogenesis is unknown but has been postulated to be due to an idiopathic trabeculitis. Herpesvirus infection has also been suggested.
 Prostaglandin-related vascular events may be related.
Prostaglandin-related vascular events may be related.
 Steroid-induced glaucoma.
Steroid-induced glaucoma.
Demographics
Ages 20 to 50 years.
Male and female patients equally affected.
Signs and Symptoms
Unilateral involvement.
Mild to moderate ocular pain.
Blurred vision.
Halos around lights.
Ophthalmic Findings
Keratic precipitates within 2 to 3 days of symptoms.
Little or no conjunctival hyperemia.
Corneal edema.
Elevated IOP, 40 to 70 mm Hg.
Few inflammatory cells.
Enlarged pupil in affected eye.
Systemic Findings
None.
Special Tests
 Tonography reveals decreased outflow facility in affected eye.
Tonography reveals decreased outflow facility in affected eye.
 Increase in aqueous humor production.
Increase in aqueous humor production.
Pathology
Tissues involved show signs of acute or chronic inflammation. Specific pathological changes are highly dependent on disease entity.
Disease Course
Acute uveitis generally resolves within several months, but the glaucoma can linger if there are structural changes.
Treatment and Management
 Does not always necessitate long term or prophylactic treatment; in many cases the disease is self-limited.
Does not always necessitate long term or prophylactic treatment; in many cases the disease is self-limited.
 During the attack, IOP can be treated medically.
During the attack, IOP can be treated medically.
Medications
 Inflammation is treated with topical steroids and/or topical + systemic nonsteroidal anti-inflammatory drugs (NSAIDs).
Inflammation is treated with topical steroids and/or topical + systemic nonsteroidal anti-inflammatory drugs (NSAIDs).
 Glaucoma medications include β-blockers, α-agonists, and topical or oral CAIs. Prostaglandins theoretically may worsen inflammation but are administered in very small concentrations.
Glaucoma medications include β-blockers, α-agonists, and topical or oral CAIs. Prostaglandins theoretically may worsen inflammation but are administered in very small concentrations.
Follow-Up
The patient may be seen during attack recurrences and on a yearly basis to rule out development of open-angle glaucoma.
Differential Diagnosis
Uveitic glaucoma of other etiology.
Acute angle-closure glaucoma: The angle is closed in the involved eye and occludable in the fellow eye, pain is severe, no keratic precipitates.
Neovascular glaucoma: rubeosis iridis, pain is severe, synechial angle closure.
Pigmentary glaucoma: can also have an acute rise in IOP, especially after heavy exercise, accompanied by pigment release, heavily pigmented angle structures, radial iris transillumination defects.
References
Posner A, Schlossman A. Syndrome of unilateral recurrent attacks of glaucoma with cyclitic symptoms. Arch Ophthalmol 1953;39:517–535.
Raitta C, Vannas A. Glaucomatocyclitic crisis. Arch Ophthalmol 1977;95:608–612.
Fuchs Heterochromic Iridocyclitis
Summary
This syndrome is a chronic idiopathic inflammatory glaucoma associated with iris stromal atrophy and cataract. Presentation is often due to decreased vision secondary to cataract.
Etiology
Actual pathogenesis is unknown.
Demographics
 Usually unilateral, but can be bilateral in 13% of patients.
Usually unilateral, but can be bilateral in 13% of patients.
 Onset at ages 30 to 40 years.
Onset at ages 30 to 40 years.
Signs and Symptoms
Unilateral involvement.
No ocular pain.
Blurred vision.
Ophthalmic Findings
Stellate keratic precipitates diffusely scattered throughout cornea.
Iris atrophy and heterochromia (involved eye is lighter, except in blue irides).
Elevated IOP, with 15% progressing to glaucoma.
Few inflammatory cells.
Cataract.
Fine blood vessels covering angle structures, which bleed when traumatized but do not cause synechial angle closure. Fine blood vessels can cause angle bleeding during intraocular surgery (Amsler’s sign).
Systemic Findings
None.
Special Tests
Iris angiography reveals leakage from normal iris vessels.
Pathology
 Iris: reduction in the number of stromal melanocytes, degeneration of iris pigment epithelium, thickening of blood vessels.
Iris: reduction in the number of stromal melanocytes, degeneration of iris pigment epithelium, thickening of blood vessels.
 Inflammatory cells and membrane in the AC angle.
Inflammatory cells and membrane in the AC angle.
Disease Course
Chronic, smoldering iridocyclitis.
Gradual development of glaucoma and cataract.
Treatment and Management
 Do not treat iridocyclitis with long-term steroid therapy, since the inflammation is unresponsive to steroids.
Do not treat iridocyclitis with long-term steroid therapy, since the inflammation is unresponsive to steroids.
 IOP can be treated medically but may eventually require surgery.
IOP can be treated medically but may eventually require surgery.
 Cataract extraction when necessary.
Cataract extraction when necessary.
Medications
Glaucoma medications include β-blockers, α-agonists, and topical or oral CAIs. Prostaglandins theoretically may worsen inflammation but are administered in very small concentrations.
Follow-Up
The patient is followed up on a regular basis similar to follow-up for POAG.
Differential Diagnosis
Uveitic glaucoma of other origin.
JRA: occurs in younger patients and is often associated with joint disease.
Reference
Jones NP. Glaucoma in Fuchs heterochromic uveitis: etiology, management and outcome. Eye 1991;6:662–667.
Lens-Induced Glaucoma
Phacolytic Glaucoma
Summary
Phacolytic, or lens protein, glaucoma is caused by a blockage of the TM with lens proteins from an intact hypermature cataract.
Etiology
High molecular weight proteins leak through the intact lens capsule of a hypermature cataract. These proteins obstruct the aqueous outflow pathway, causing an elevated IOP. Macrophages ingesting the proteins and inflammatory debris may play a role in blocking the TM.
Demographics
Can be seen in any adult patient with a hypermature cataract.
Does not occur in children.
Signs and Symptoms
Decreased vision.
Moderate to severe ocular pain.
Halos around lights.
Ophthalmic Findings
See Figure 5.15.
Granulomatous keratic precipitates.
Significant conjunctival hyperemia.
Corneal edema.
Elevated IOP.
White cataract, may have white material on capsular surface or wrinkling of the anterior lens capsule.
AC flare.
The lens may be in place or dislocated into the vitreous.
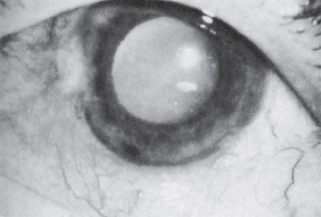
FIGURE 5.15. Phacolytic glaucoma. Hypermature cataract with leakage of lens proteins through the intact lens capsule. (From Epstein DL. Lens-induced open-angle glaucoma. In: Ritch R, Shields MB, eds. The secondary glaucomas. St. Louis, MO: Mosby, 1982:424, with permission.)
Systemic Findings
None.
Special Tests
 Paracentesis shows engorged macrophages.
Paracentesis shows engorged macrophages.
 High–molecular-weight proteins in aqueous humor.
High–molecular-weight proteins in aqueous humor.
Pathology
 Eosinophilic proteinlike material and engorged lipid-laden macrophages in the TM.
Eosinophilic proteinlike material and engorged lipid-laden macrophages in the TM.
 The number of macrophages does not correspond to the severity of the glaucoma.
The number of macrophages does not correspond to the severity of the glaucoma.
Disease Course
The glaucoma typically abates after cataract extraction.
Treatment and Management
 Reduce IOP by medical treatment.
Reduce IOP by medical treatment.
 Reduce inflammation with topical steroids and cycloplegics.
Reduce inflammation with topical steroids and cycloplegics.
 Cataract extraction following reduction in IOP and inflammation.
Cataract extraction following reduction in IOP and inflammation.
Follow-Up
The patient should be seen on the first postoperative day and regularly until the IOP normalizes.
Differential Diagnosis
Uveitic glaucoma.
Acute angle-closure glaucoma: The angle is closed in the involved eye and occludable in the fellow eye, pain is severe, no keratic precipitates.
Glaucomatocyclitic crisis: recurrent attacks of idiopathic inflammatory glaucoma without cataract.
Lens-particle glaucoma: history of lens trauma or surgery with retained lens particles and a violation of the capsule.
Reference
Flocks M, Littwin CS, Zimmerman LE. Phacolytic glaucoma: clinicopathologic study of 138 cases of glaucoma associated with hypermature cataract. Arch Ophthalmol 1955;54:37–47.
Lens-Particle Glaucoma
Summary
Lens-particle glaucoma is caused by retained lenticular material following trauma or surgery in which the lens capsule is violated.
Etiology
Liberated lens material obstructs the aqueous outflow pathway, causing an elevated IOP.
Demographics
Can be seen in any patient with lens material in the anterior or posterior chamber.
Signs and Symptoms
Decreased vision.
Moderate ocular pain.
Halos around lights.
Photophobia.
History of recent trauma, cataract surgery, or laser capsulotomy.
Ophthalmic Findings
See Figure 5.16.
Keratic precipitates.
Conjunctival hyperemia.
Elevated IOP.
White fluffy lens material free in the anterior or posterior chamber.
AC flare.
Open AC angle by gonioscopy.
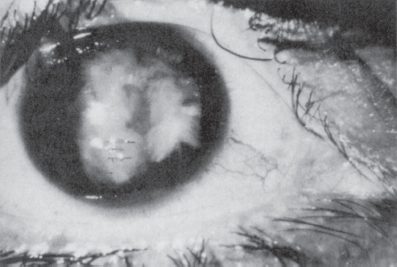
FIGURE 5.16. Lens-particle glaucoma. Retained lens fragments swell and occlude the outflow pathways. (From Epstein DL. Lens-induced open-angle glaucoma. In: Ritch R, Shields MB, eds. The secondary glaucomas. St. Louis, MO: Mosby, 1982:427, with permission. Courtesy of C. Davis Belcher III, MD.)
Systemic Findings
None.
Special Tests
None.
Pathology
Lens particles, inflammatory cells, and engorged macrophages are seen in the AC.
Disease Course
The glaucoma typically abates after removal of the lens particles.
Treatment and Management
 Reduce IOP by medical treatment.
Reduce IOP by medical treatment.
 Reduce inflammation with topical steroids and cycloplegics.
Reduce inflammation with topical steroids and cycloplegics.
 Remove lens particles via aspiration or vitrectomy for larger pieces of lens material.
Remove lens particles via aspiration or vitrectomy for larger pieces of lens material.
 Examine optic nerve to assess damage and urgency of treatment.
Examine optic nerve to assess damage and urgency of treatment.
Follow-Up
The patient should be seen frequently, especially during the first week.
Differential Diagnosis
Uveitic glaucoma.
Acute angle-closure glaucoma: The angle is closed in the involved eye and occludable in the fellow eye, pain is severe, no keratic precipitates.
Glaucomatocyclitic crisis: recurrent attacks of idiopathic inflammatory glaucoma without cataract.
Phacolytic glaucoma: mature or hypermature cataract with an intact lens capsule.
Infectious endophthalmitis: needs to be ruled out unless lens material is clearly visible.
Phacoanaphylactic glaucoma: absence of fluffy lens material, also follows trauma or surgery.
Reference
Epstein DL. Diagnosis and management of lens-induced glaucoma. Ophthalmology 1982;89:227–230.
Phacoantigenic Glaucoma
Summary
Phacoantigenic (phacoanaphylactic) glaucoma is a rare granulomatous inflammatory response to penetrating lens injury resulting from an immunologic response to lens protein.
Etiology
 Previously thought to be an immune rejection of previously sequestered lens material analogous to immune rejection of a foreign tissue transplant.
Previously thought to be an immune rejection of previously sequestered lens material analogous to immune rejection of a foreign tissue transplant.
 Now hypothesized to be an immunologic disease resulting from a loss of normal immune tolerance to lens material.
Now hypothesized to be an immunologic disease resulting from a loss of normal immune tolerance to lens material.
Demographics
Can be seen in any patient after penetrating lens injury.
Signs and Symptoms
Decreased vision.
Moderate ocular pain.
Halos around lights.
Photophobia.
History of recent trauma, cataract surgery, or laser capsulotomy.
Ophthalmic Findings
Keratic precipitates (often granulomatous).
Conjunctival hyperemia.
Corneal edema.
Elevated IOP.
Synechiae formation.
AC flare.
Systemic Findings
None.
Special Tests
Aqueous aspiration shows polymorphonuclear neutrophils (PMNs).
Pathology
 Typical zonal granulomatous inflammation.
Typical zonal granulomatous inflammation.
 The lens is surrounded by an inner layer of PMNs, a middle layer of multinucleated giant cells, and an outer layer of mixed mononuclear cells.
The lens is surrounded by an inner layer of PMNs, a middle layer of multinucleated giant cells, and an outer layer of mixed mononuclear cells.
Disease Course
Without removal of the lens material, the glaucoma and inflammation worsen and may result in phthisis.
Treatment and Management
 Reduce IOP by medical treatment.
Reduce IOP by medical treatment.
 Reduce inflammation with topical steroids and cycloplegics.
Reduce inflammation with topical steroids and cycloplegics.
 Remove lens particles as soon as possible via aspiration or vitrectomy.
Remove lens particles as soon as possible via aspiration or vitrectomy.
Follow-Up
The patient should be seen frequently, especially during the first week.
Differential Diagnosis
Toxic reactions to intraocular lens material or intracameral injections.
Lens particle glaucoma: fluffy white material in the AC.
Phacolytic glaucoma: mature or hypermature cataract with an intact lens capsule.
Infectious endophthalmitis: needs to be ruled out unless lens material is clearly visible.
Sympathetic ophthalmia: granulomatous panuveitis following ocular injury.
Reference
Marak GE. Phacoanaphylactic endophthalmitis. Surv Ophthalmol 1992;36:325–339.
Traumatic Glaucoma
Hyphema
Elevated IOP attributable to intraocular bleeding following eye trauma can be a result of hyphema, or later from ghost cell or hemolytic glaucoma. Spontaneous hyphema is managed differently and should alert one to coagulopathies, neovascularization, sickle cell disease, blood dyscrasias and, in children, juvenile xanthogranuloma.
Etiology
Hyphema: red blood cells in the AC obstruct the outflow pathway.
Demographics
Can be seen in any patient with blunt or penetrating ocular trauma, which is more common in young male patients.
Signs and Symptoms
Decreased vision.
Ocular pain.
Photophobia.
History of recent trauma.
Ophthalmic Findings
Hyphema: layered red blood cells (RBCs) or a blood clot in the AC.
Microhyphema: RBCs suspended in the aqueous humor.
Corneal blood staining.
Conjunctival hyperemia and edema.
Other signs of ocular trauma such as lens subluxation, ruptured globe, eyelid edema, and ecchymosis.
Systemic Findings
None.
Special Tests
 Hemoglobin electrophoresis in African American patients, especially those with spontaneous hyphema, mild ocular trauma, or IOP elevation that is out of proportion to hyphema or prolonged in nature.
Hemoglobin electrophoresis in African American patients, especially those with spontaneous hyphema, mild ocular trauma, or IOP elevation that is out of proportion to hyphema or prolonged in nature.
 B-scan ultrasound if the posterior pole cannot be visualized.
B-scan ultrasound if the posterior pole cannot be visualized.
Pathology
Blood and blood breakdown products are seen in the AC and outflow pathway tissues and in the corneal endothelium and stroma in corneal blood staining.
Disease Course
 The glaucoma typically resolves after spontaneous clearing of the blood.
The glaucoma typically resolves after spontaneous clearing of the blood.
 Rebleeding may occur and is most common at 3 to 7 days, when clot lysis and retraction occur. Rebleeding is estimated to occur in 5% to 10% of cases. This increases the risk of optic nerve damage, corneal blood staining, or vitreous hemorrhage. Risk factors for rebleeding include black race, patients using aspirin, those having systemic hypertension or ocular hypotony, or those presenting more than 24 hours after injury.
Rebleeding may occur and is most common at 3 to 7 days, when clot lysis and retraction occur. Rebleeding is estimated to occur in 5% to 10% of cases. This increases the risk of optic nerve damage, corneal blood staining, or vitreous hemorrhage. Risk factors for rebleeding include black race, patients using aspirin, those having systemic hypertension or ocular hypotony, or those presenting more than 24 hours after injury.
 Sickle cell disease may make the bleeding and the IOP elevation worse. The RBCs tend to become sickle shaped and rigid in the AC and are less able to be cleared through the outflow pathway.
Sickle cell disease may make the bleeding and the IOP elevation worse. The RBCs tend to become sickle shaped and rigid in the AC and are less able to be cleared through the outflow pathway.
Treatment and Management
 Medical management with aqueous suppressants, topical steroids, and cycloplegic agents to control inflammation and IOP. CAIs may worsen sickling of RBCs in patients with sickle cell disease by increasing aqueous ascorbic acid and thus changing the pH of the aqueous. Adrenergic agonists with α1-agonist activity (epinephrine, dipivefrin, apraclonidine) should also be avoided in sickle cell patients because of their vasoconstriction effects which could cause anterior segment ischemia.
Medical management with aqueous suppressants, topical steroids, and cycloplegic agents to control inflammation and IOP. CAIs may worsen sickling of RBCs in patients with sickle cell disease by increasing aqueous ascorbic acid and thus changing the pH of the aqueous. Adrenergic agonists with α1-agonist activity (epinephrine, dipivefrin, apraclonidine) should also be avoided in sickle cell patients because of their vasoconstriction effects which could cause anterior segment ischemia.
 Bed rest and elevation of the head of bed to promote layering of the blood. Bilateral patching may be indicated in severe cases (these are of unproven value).
Bed rest and elevation of the head of bed to promote layering of the blood. Bilateral patching may be indicated in severe cases (these are of unproven value).
 Surgical intervention is advised if there is a likelihood of optic nerve damage or corneal blood staining. Patients with sickle cell disease or prior glaucomatous optic atrophy should have a lower threshold for intervention.
Surgical intervention is advised if there is a likelihood of optic nerve damage or corneal blood staining. Patients with sickle cell disease or prior glaucomatous optic atrophy should have a lower threshold for intervention.
AC washout without disturbing the clot is usually sufficient.
Surgical evacuation of the clot. This may increase the chance of rebleeding and should be approached with caution.
Trabeculectomy can afford temporary control of IOP and allow removal of RBCs or clot.
Medications
Glaucoma medications include β-blockers, α2-agonists, hyperosmotics, and CAIs (avoid in sickle cell patients).
 Cycloplegia should be performed.
Cycloplegia should be performed.
 Aminocaproic acid (50 mg/kg by mouth [p.o.] every 4 hours ×5 days) can be considered to prevent rebleeding but is usually unnecessary. It can cause postural hypotension and is contraindicated in patients with hepatic or renal disease, coagulopathies, cardiovascular or cerebrovascular disease, or pregnancy. Topical forms of this drug can be administered.
Aminocaproic acid (50 mg/kg by mouth [p.o.] every 4 hours ×5 days) can be considered to prevent rebleeding but is usually unnecessary. It can cause postural hypotension and is contraindicated in patients with hepatic or renal disease, coagulopathies, cardiovascular or cerebrovascular disease, or pregnancy. Topical forms of this drug can be administered.
 Oral steroids can be used as an alternative to aminocaproic acid. A relatively high dose is needed: prednisone 1.5 to 2.0 mg/kg PO daily for clot stabilization.
Oral steroids can be used as an alternative to aminocaproic acid. A relatively high dose is needed: prednisone 1.5 to 2.0 mg/kg PO daily for clot stabilization.
 A topical form of aminocaproic acid (Caprogel) has been developed and studied for efficacy. Phase III, multicenter, placebo-controlled trial for use in traumatic hyphema provides evidence that Caprogel is safe and reduces rebleeding rates below that of placebo (authors do recommend a larger trial for more definitive conclusions).
A topical form of aminocaproic acid (Caprogel) has been developed and studied for efficacy. Phase III, multicenter, placebo-controlled trial for use in traumatic hyphema provides evidence that Caprogel is safe and reduces rebleeding rates below that of placebo (authors do recommend a larger trial for more definitive conclusions).
 Tissue plasminogen activator (tPA) intracameral injection can accelerate the resolution of a hyphema, but may cause rebleeding.
Tissue plasminogen activator (tPA) intracameral injection can accelerate the resolution of a hyphema, but may cause rebleeding.
Follow-Up
Follow-up examinations during the first week, 3 to 4 weeks after stabilization, and yearly. Examine the optic nerve for damage, the outflow structures for angle recession, and the rest of the eye for signs of traumatic damage.
Differential Diagnosis
1. Early:
Inflammatory cells and proteins causing increased IOP.
TM tears.
2. Late:
Traumatic angle recession: occurs later, characteristic gonioscopic appearance of widened ciliary body band.
Hemolytic glaucoma: Hemolytic debris and hemoglobin-filled macrophages block outflow.
Ghost cell glaucoma: Denatured RBCs from the vitreous block the outflow pathway when a break in the anterior hyaloid allows entrance into the AC.
Lens-induced glaucoma.
Epithelial or fibrous downgrowth: characteristic sheets of abnormal tissue covering and distorting structures.
Retinal detachment (Schwartz syndrome): Degenerated photoreceptor elements from an old RD block the outflow pathway.
References
Filipe JA, Barros H, Castro-Correia J. Sports-related ocular injuries: a three-year follow-up study. Ophthalmology 1997;104:313–318.
Pieramici DJ, Goldberg MF, Melia M, et al. A phase III, multicenter, placebo-controlled clinical trial of topical aminocaproic acid (Caprogel) in the management of traumatic hyphema. Ophthalmology 2003;110(11):2106–2112.
Sihota R, Sood NN, Agarwal HC. Traumatic glaucoma. Acta Ophthalmol Scand 1995;73:252–254.
Ghost Cell and Hemolytic Glaucoma
Summary
Ghost cell glaucoma occurs when degenerated RBCs from a vitreous hemorrhage gain access to the AC through a disrupted anterior hyaloid face and obstruct aqueous outflow. Hemolytic glaucoma usually follows a hyphema, and involves obstruction of the angle from blood breakdown products and hemosiderin-laden macrophages.
Etiology
Ghost cell: Ghost cells are RBCs that have lost their intracellular hemoglobin and are less pliable than normal RBCs. They gain entrance to the AC and obstruct the outflow pathway.
Hemolytic: Hemolytic debris from macrophages and the breakdown products of blood obstruct the TM.
Demographics
Can be seen in any patient with blunt or penetrating ocular trauma, which is more common in young male patients.
Signs and Symptoms
Decreased vision.
Ocular pain.
Photophobia.
History of trauma.
Ophthalmic Findings
Ghost cells (swollen, tan cells) or pigment-laden macrophages in the AC and angle (Figure 5.17).
Disrupted anterior hyaloid face.
Old hyphema.
Conjunctival hyperemia.
Other signs of ocular trauma such as angle recession, lens subluxation, ruptured globe, eyelid edema, and ecchymosis.
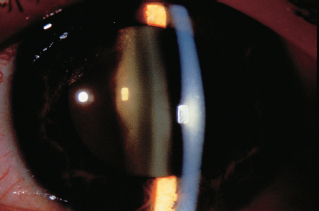
FIGURE 5.17. Ghost cell glaucoma. After a hyphema, degenerated red blood cells swell and do not traverse the trabecular meshwork as easily. Notice the layering of blood and khaki-colored cells. (From Tasman W, Jaeger E. The Wills Eye Hospital atlas of clinical ophthalmology, 2nd ed. Lippincott Williams & Wilkins, 2001.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


