Medical and Surgical Treatments for Childhood Glaucomas
The successful treatment of childhood glaucoma presents many challenges, with control of intraocular pressure (IOP) as the first but not the only priority. The optimal treatment strategies for children often differ greatly from those for adults with glaucoma. Factors influencing decisions about therapy include those related not only to the type and severity of the glaucoma but also to the age and needs of the particular child.
MEDICAL THERAPY
Although surgical intervention is the primary treatment for primary congenital glaucoma and closed-angle glaucomas (e.g., secondary to cicatricial retinopathy of prematurity), medications are the initial and often the mainstay of therapy for juvenile open-angle glaucoma and other secondary glaucomas (e.g., such as those occurring in aphakia or with uveitis). Medications also play an important auxiliary role even in cases of congenital glaucoma, wherein they may help clear the cornea preoperatively to facilitate goniotomy and may help control IOP postoperatively until the success of surgical intervention has been determined. Medical therapy is also indicated in managing those difficult cases in which surgery poses particular risks or has incompletely controlled glaucoma (1). Besides inadequate IOP reduction, multiple factors conspire against the success of long-term medical therapy in childhood glaucomas: the difficulties with long-term adherence, adequate ascertainment of drug-induced side effects, and potential adverse systemic effects of protracted therapy, among others.
Many medications are now available for the reduction of IOP in patients with glaucoma. The Food and Drug Administration (FDA) initially approved all of them for use without requiring data on the safety and efficacy of these drugs in pediatric patients. Ongoing study of several major new drugs is currently being undertaken by several major pharmaceutical companies, under the supervision of the FDA. For example, a randomized, double-masked, 3-month trial compared dorzolamide, 2%, three times daily with timolol, 0.25% or 0.5%, once daily in patients younger than 6 years who had glaucoma; the study found both treatments to be relatively safe and effective (2). A similarly designed study, again conducted among children with glaucoma who were younger than 6, compared use of brinzolamide, 1%, twice a day with use of levobetaxolol, 0.5%, twice a day, and it demonstrated that both drugs were well tolerated and lowered IOP (3). Nonetheless, many of the commonly used glaucoma drugs still carry a warning that “safety and efficacy in pediatric patients have not been established.” Furthermore, certain drugs, such as brimonidine, carry warnings about dangerous systemic side effects in infants and young children. Because eyedrops are not downsized for pediatric use and because the plasma volume of a small child is much smaller than that of an average adult counterpart, blood levels of glaucoma drugs can reach high levels in young children at doses recommended for use in adults (4). Even topical glaucoma medication must be used with careful forethought in children, particularly in those who are very small or with special considerations such as premature birth, asthma, or other cardiac or pulmonary problems.
Table 40.1 gives information pertaining to the suggested use of various glaucoma drugs specifically in infants and children with glaucoma. (Detailed information on the use and mechanisms of these medications is provided elsewhere in this text.)
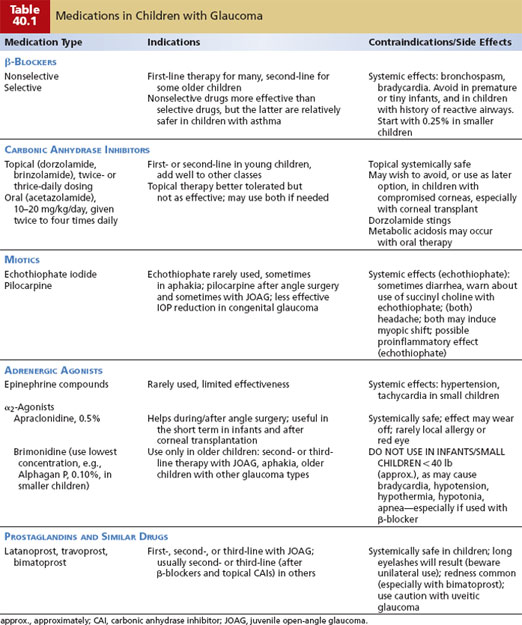
Carbonic Anhydrase Inhibitors
Oral carbonic anhydrase inhibitors, primarily acetazolamide (Diamox), have effectively reduced elevated IOP in infants and children with primary infantile (and other types of) glaucoma for decades, often reducing the IOP about 20% to 35%. When administered orally with food or milk three or four times daily (total dosage, 10 to 20 mg/kg/day), acetazolamide is fairly well tolerated (1,5). Caregivers should be queried specifically about the occurrence of diarrhea, diminished energy levels, and loss of appetite in children on this therapy, as such effects would necessitate a dosage adjustment or discontinuation of use. Metabolic acidosis has also been reported in infants (6), in whom it may manifest as rapid breathing and may be somewhat ameliorated with oral sodium citrate and citric acid oral solution (Bicitra, 1 mEq/kg/day) (7).
The topical carbonic anhydrase inhibitor, dorzolamide (Trusopt), offers a viable alternative to acetazolamide for many patients. In a small crossover trial, 11 children whose glaucoma was controlled on topical β-blocker and oral acetazolamide switched from the oral acetazolamide to topical dorzolamide, three times daily, in the study eye. Mean IOP reduction with use of the topical agent was approximately 25%, compared with approximately 35% on acetazolamide (8). Although systemic side effects occurred commonly in patients receiving the acetazolamide, no adverse effects were noted with the use of topical dorzolamide. The addition of oral acetazolamide to topical dorzolamide has been reported to reduce IOP further than when either drug is used alone (9).
A second topical carbonic anhydrase inhibitor, brinzolamide (Azopt), has also been well tolerated by children, with IOP reduction similar to that obtained with use of dorzolamide (Freedman SF, unpublished data). In one study of brinzolamide and levobunolol treatment in children with glaucoma younger than 6 years, both drugs were well tolerated, but brinzolamide was more effective in patients with glaucoma associated with systemic or ocular abnormalities than in patients with primary congenital glaucoma (3). The carbonic anhydrase inhibitors are useful for treating pediatric glaucoma and may be appropriate first- and second-line agents, respectively, when β-blocker use is contraindicated or inadequately effective (Table 40.1; also see the following text). (The combination of a topical carbonic anhydrase inhibitor [dorzolamide] with the β-blocker timolol is discussed further in the β-Blockers section.)
Miotics
The use of miotic drugs has largely been supplanted by that of newer medications. Cholinergic stimulators, often called miotics, have limited value in the treatment of childhood glaucoma. Eyes with congenital glaucoma often show poor IOP reduction to miotics, perhaps because of the abnormal insertion of the ciliary muscle into the trabecular meshwork (10,11). However, pilocarpine is often used to achieve and maintain miosis before and after goniotomy or trabeculotomy for congenital glaucoma (12,13). Stronger miotics, such as echothiophate iodide (phospholine iodide), have also been administered in infants, especially those with aphakic glaucoma, with less ocular irritation than that observed in adults (12). Echothiophate iodide therapy has sometimes been accompanied by diarrhea and requires extreme care in the concurrent use of succinyl choline for general anesthesia. Older children, if phakic, often experience severe visual blurring attributable to myopia induced by miotics. If they are necessary and effective in treating the glaucoma, miotics in these children may be better tolerated when the induced myopia is rendered stable, so that spectacles can compensate for it. When used in older children, higher concentrations (e.g., pilocarpine, 2% to 4%) may be useful (Table 40.1).
β-Adrenergic Antagonists (β-Blockers)
Topical β-blockers have been available for the treatment of glaucoma since the introduction of timolol in 1978. Several studies have examined the role of timolol in treating uncontrolled childhood glaucomas (4,14–18). In a study of 67 patients (100 eyes) with childhood glaucomas who began topical therapy with timolol before 18 years of age, 30 patients (40 eyes) experienced a mean IOP decrement of 21.3% and required no further surgery or medical therapy over a 2.5-year follow-up period (17). Most patients whose glaucoma stabilized on timolol did so using 0.25% twice daily, and all the patients with adverse reactions (10%) were using timolol, 0.5%. Only two patients discontinued use of timolol because of side effects—a 10-year-old who developed severe asthma and a 17-year-old with symptomatic bradycardia (17). The incidence of systemic side effects reported in these studies varied from 0% to 18% (4,14–18).
The most severe systemic adverse effects in children receiving topical timolol therapy have included acute asthma attacks, bradycardia, and apneic spells (the latter in neonates) (4,18–20). Plasma timolol levels measured in children using 0.25% timolol (ranging from 3.5 ng/mL in a 5-year-old to 34 ng/mL in a 3-week-old) vastly exceeded those in adults using 0.5% timolol (range, 0.34 to 2.45 ng/mL) (4). The use of punctal occlusion in adults further lowered mean 1-hour plasma timolol levels by 40% in the adult patients in this study (from 1.34 to 0.9 ng/mL). The high plasma timolol levels in children may be explained by a child’s volume of distribution for the drug, which is much smaller than that of an adult.
When timolol is used in small children, treatment should always begin with 0.25% drops, excluding those children with a history of asthma or bradycardia. Topical β-blockers should be used with extreme caution in neonates, with particular attention to the possibility of apnea. It may be reasonable to observe children for adverse systemic effects for 1 to 2 hours in the office after an initial dose of β-blocker has been given before prescribing the β-blocker for outpatient use (16,20). Punctal occlusion, when feasible, should be performed by parents or other caretakers (16). There is anecdotal evidence that using timolol as Timoptic XE or timolol gel-forming solution, once daily, may result in lower plasma drug levels, compared with the same concentration of solution used twice daily.
There is little information available on the use of topical β-blockers other than timolol in the treatment of childhood glaucoma. A short-term, randomized, double-masked comparison of levobetaxolol and brinzolamide in children younger than 6 years demonstrated that both drugs were well tolerated and lowered IOP in this group. In children naïve to prior medication, levobetaxolol was more effective in primary congenital glaucoma than in glaucoma with associated ocular or systemic abnormalities (3). Based on experience in adults, betaxolol, as a relatively β-1–selective β-blocker, may be less susceptible to precipitating acute asthma attacks (which may present as coughing) than the nonselective β-blockers. The remaining nonselective β-blockers should be approached in a fashion similar to timolol regarding risks and probable efficacy. As in adults, β-blockers used in children often do have an additive effect to oral and topical carbonic anhydrase inhibitors in treating children with glaucoma (1,15).
Two combination preparations that include timolol, 0.5%, are currently available commercially in the United States. The first preparation, combining timolol, 0.5%, and dorzolamide, 2.0% (Cosopt, now also available as generic; used twice daily), is a potent IOP-reducing agent in older children, but it must be avoided in infants because of the relatively high concentration of timolol. The newer drug, Combigan, combines timolol, 0.5%, plus brimonidine, 0.2%; this potent agent must be used with caution in children and never in those for whom either ingredient alone would be contraindicated (see Adrenergic Agonists section; Table 40.1).
Topical β-blockers, despite their contraindication in some cases, still have an important role in treating children with glaucoma and are appropriate first-line drugs for many children (Table 40.1).
Adrenergic Agonists
Epinephrine compounds have been used in infants and children with glaucoma (21,22), but there are little published data to suggest optimal dosing schedules or the magnitude of the pressure decrement to be expected from these drugs. These drugs, furthermore, are relegated to secondary importance because of their potential for systemic toxicity (e.g., tachyarrhythmias, hypertension) and their ocular side effects (e.g., irritation, reactive hyperemia, adrenochrome deposits), together with their limited effectiveness. Topical dipivefrin (Propine), as an epinephrine prodrug, should theoretically have fewer systemic side effects in children than epinephrine does.
The two commercially available α2-adrenergic agonists, apraclonidine and brimonidine, have a valid role in the treatment of pediatric glaucoma, although neither drug has been approved by the FDA for use in children. Apraclonidine (Iopidine, 0.5%) can be useful and well tolerated in the setting of angle surgery to minimize intraoperative hyphema (see later under Goniotomy) and may have a short-term role for treating infants who cannot tolerate β-blockers or who have had recent corneal transplantation (and in whom one therefore wishes to avoid topical carbonic anhydrase inhibitors). Wright and Freedman found an 8% incidence of side effects among 75 infants and children given apraclonidine, 0.5%, with lethargy reported in 3 children younger than 5 months of age (23).
Brimonidine (available as brimonidine, 0.2%, and Alphagan P, 0.10% and 0.15%) can be useful in reducing IOP in older children, but it must be used with extreme caution in younger children. Its use should be avoided altogether in infants and in small and underweight children, because of its propensity to cause severe systemic side effects. Topical brimonidine administration has caused bradycardia, hypotension, hypothermia, hypotonia, and apnea in infants, and severe somnolence in toddlers (24–26), especially when combined with topical β-blockers (27).
Brimonidine is rarely an appropriate first-line drug for children, except in selected older children with intolerance to β-blockers and carbonic anhydrase inhibitors. It may, however, be useful adjunctive therapy in those patients needing additional IOP reduction (Table 40.1).
The combination of brimonidine, 0.2%, and timolol, 0.5%, Combigan, is a potent drug (see the preceding text) that should not be used in children with contraindication to either of the component ingredients.
Prostaglandins
The prostaglandin-type drugs can prove useful in some selected cases of pediatric glaucoma, although published data are limited, and none of these drugs has received FDA approval for pediatric use. Latanoprost (Xalatan) has been useful in selected cases of pediatric glaucoma, particularly in patients with juvenile open-angle glaucoma and some patients with aphakia and port-wine stain–associated glaucoma; no serious systemic side effects have been reported (28–31). Travoprost (Travatan) has recently been reported to be well tolerated and effective at IOP reduction in selected patients with pediatric glaucoma (32). The prostaglandin drugs do induce growth of eyelashes in pediatric patients (29,30,33) (Fig. 40.1); surface redness, periocular skin pigmentation, and iris darkening have all been noted as well ((30); Freedman SF, unpublished data). Caution is advised if these drugs are used in children with uveitis, or with aphakia or pseudophakia (although reports of cystoid macular edema in pediatric cases are lacking at this time).

Figure 40.1 Long and thick eyelashes in both eyes of an 11-year-old boy who has taken latanoprost for treatment of mild aphakic glaucoma.
Prostaglandin-like agents do not yet seem appropriate as first-line treatment for children, except perhaps for selected cases of juvenile open-angle glaucoma with special risk for β-blocker use. These agents may play an important adjunctive role when IOP control is inadequate despite use of other medications already discussed (Table 40.1).
SURGICAL THERAPY
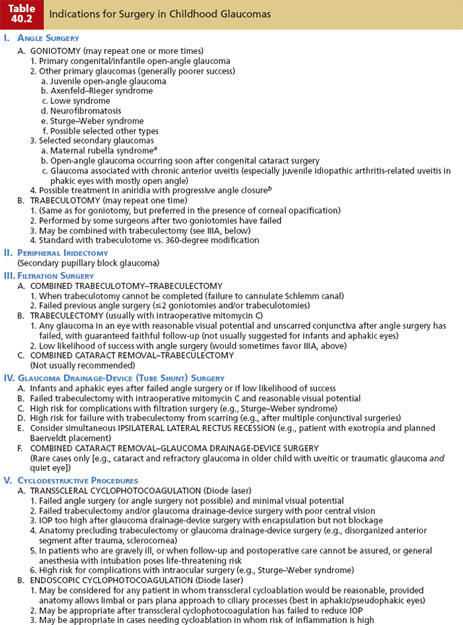
There are various surgical procedures available to treat children with glaucoma (Table 40.2). Although the appropriate intervention in some cases is clear and widely agreed on (e.g., angle surgery for congenital–infantile glaucoma [see later]), the optimal surgical algorithm is, in many cases, open to disagreement, even among experts who care for these children. One reason for this heterogeneity in surgical management undoubtedly relates to the challenges in performing surgery in children with refractory glaucoma. Even the anesthesia itself poses significant risks, especially in neonates. Many factors make the infant eye behave differently (usually in a more challenging way) from the adult eye during glaucoma surgery—a smaller palpebral fissure, less rigid and often thinned sclera and limbal tissue (especially in buphthalmic eyes), clouding of the cornea, and narrowness of the anterior chamber are a few. Postoperatively, it may be challenging to adequately protect the operated eye from accidental injury, to monitor for possible surgical complications and response to surgery, and to ensure adherence to medication regimens and recommended restriction of physical activity.

Often, it can be helpful to develop appropriate expectations on the part of the family ahead of the surgery; hence family members should be informed preoperatively of the multiple visits and additional anesthesias that may be needed postoperatively, and the likelihood that further surgery may be required to control the glaucoma. Often, the first examination under anesthesia can be immediately followed by the first indicated surgical procedure.
Angle Surgery
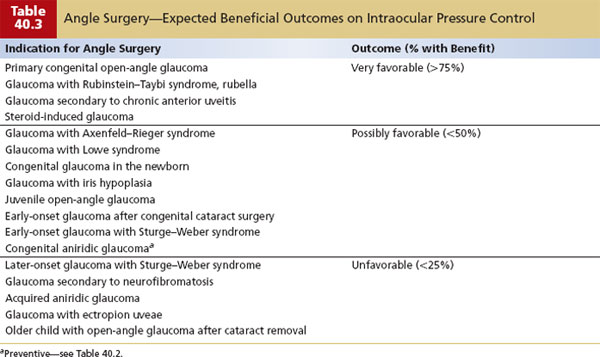
The introduction of angle surgery (first goniotomy and then trabeculotomy ab externo) drastically improved the previously poor prognosis for children with primary congenital–infantile glaucoma. Both goniotomy and trabeculotomy ab externo have their staunch advocates, but neither procedure has been definitively proven better than the other for treating primary infantile glaucoma. These procedures are also useful in other selected cases of pediatric glaucoma (see later and Table 40.3).
With the aim of incising the uveal trabecular meshwork under direct visualization, goniotomy is the surgical procedure of choice in many cases of primary congenital glaucoma. Trabeculotomy ab externo (see the following text), an alternative procedure, is especially useful when corneal clouding prevents an optimal view of the angle structures by gonioscopy.
Goniotomy
In 1893, the Italian ophthalmologist Carlo de Vincentiis described a new operation that attempted to open Schlemm canal by incising the angle tissues (without visualization of the angle) (34). Because of a high complication rate and poor results in adults with chronic open-angle glaucoma, this operation was initially abandoned. With the advantage of clinical gonioscopy, Otto Barkan modified the technique as an operation for primary congenital glaucoma in 1938, dubbing it “goniotomy” (Gk. gonio—angle and tomein—to cut) (35). This effective operation for congenital glaucoma dramatically improved the previously dismal prognosis for this condition (36). The technique for performing goniotomy has remained essentially unaltered for more than 50 years—a testament to the effectiveness and widespread use of this elegant, brief, conjunctival-sparing procedure as an initial intervention for primary congenital glaucoma (1). Although the aim of goniotomy is to open a route for aqueous humor to exit the anterior chamber into the Schlemm canal by removing obstructing tissue, the precise mechanism by which pressure reduction occurs remains obscure. Successful goniotomy does appear, however, to reduce the IOP by improving facility of aqueous outflow (37). Goniotomy enjoys its greatest success in the treatment of primary congenital glaucoma presenting between 3 and 12 months of age (1), but it may also be used in other primary developmental and secondary glaucomas, although with reduced success (1,37) (Table 40.3). Examples of these other primary glaucomas include juvenile open-angle glaucoma (38) and early-onset glaucomas associated with Sturge–Weber syndrome, neurofibromatosis, and Lowe syndrome. Several secondary glaucomas may respond favorably to goniotomy in some cases (7), including glaucoma complicating chronic anterior uveitis and selected cases of aphakic glaucoma presenting early after congenital cataract surgery (39,40). Goniotomy has been advocated as a prophylactic procedure in congenital aniridia before glaucoma develops, but its use in this setting is particularly technically challenging (41,42) (Table 40.3).
Preoperative medications should ideally be used for several days before planned goniotomy to maximally reduce the IOP and clear the cornea. Medications often used include oral acetazolamide or topical dorzolamide, together with apraclonidine, 0.5%, and judicious use of a topical β-blocker in selected cases. To produce miosis, pilocarpine, 1% or 2%, should be placed on the eye just before it undergoes surgery, to promote miosis and thereby aid in protecting the crystalline lens from injury during the procedure. Acetylcholine chloride 1:100 (e.g., Miochol) may be injected into the anterior chamber if necessary to promote further miosis. Apraclonidine, 0.5%, may be applied to the eye just before surgery and may help decrease intraoperative bleeding.
Basic Technique
Goniotomy is performed by using a surgical goniolens and a goniotomy knife or needle (Table 40.4; Fig. 40.2) (43). There are several available types of goniolens, in addition to the round-domed Barkan goniolens, including the Lister modification, which includes irrigation, the Swan–Jacobs lens, which incorporates a handle, as well as the Hill goniolens and Khaw surgical goniolens, both of which allow the surgeon holding the lens also to fixate the globe. Numerous modifications of the Barkan goniotomy knife have been described, including attached fiber optics for intraocular illumination (44). A nontapered Swan knife (or needle–knife) enters the anterior chamber easily and cuts in either direction. Alternatively, a disposable 25-gauge needle attached to a syringe containing viscoelastic or Miochol may be used in place of a knife, allowing the anterior chamber to be deepened before incision and to be maintained on instrument removal (45,46). The author prefers the latter method, using only enough viscoelastic to ensure chamber maintenance on needle withdrawal. Enthusiastic use of the viscoelastic may acutely increase corneal edema by increasing IOP, thereby degrading the surgeon’s view of the angle structures.
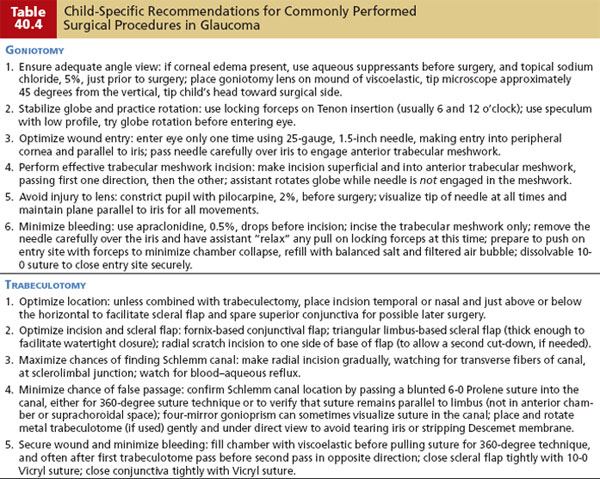
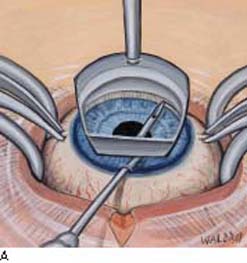

Figure 40.2 Goniotomy from temporal side, shown using a Barkan goniotomy lens and 25-gauge needle used as the goniotomy knife. A: Incision in anterior trabecular meshwork, shown beginning from right to left. B: Correct location and depth of the goniotomy incision.
To perform goniotomy safely and effectively, corneal clarity must be sufficient to allow an adequate view of the angle structures. To this end, preoperative use of glaucoma medications and prompt application of sodium chloride, 5%, drops to the cornea under anesthesia may improve the angle view in borderline cases. Although corneal epithelial scraping has been described to facilitate an angle view for goniotomy, corneal stromal edema often persists after epithelial removal; in this setting trabeculotomy may be preferred (see Trabeculotomy). Alternatively, endoscopic visualization has been used for goniotomy in the setting of corneal opacification (47–49).
Goniotomy surgery can be performed with a binocular head loupe, although the operating microscope provides better visualization (and affords the assistant a view of the angle) (50). The surgeon usually sits opposite to the portion of the angle to be operated (i.e., to the temporal side of the patient for nasal goniotomy), with the patient’s head slightly rotated away from the surgeon. Moody or other locking fixation forceps may be placed on the superior and inferior rectus muscles when a nasal or temporal goniotomy is planned. Alternatively, the globe can be adequately held by applying the locking forceps nearer to the limbus, at the level of the Tenon insertion, with less likelihood of acutely worsening corneal edema. Viscoelastic may be placed onto the central cornea just before the operating goniolens is placed and may be helpful in preventing the formation of air bubbles between the goniolens and the cornea. The goniotomy lens may be stabilized with a nontoothed fine forceps in the positioning holes of the lens, or it may be modified to include a handle.
The goniotomy knife or needle is placed through peripheral clear cornea 1 mm from the limbus, opposite to the midpoint of the intended goniotomy, in a plane parallel to the iris. The knife or needle is guided over iris tissue (not pupil) to engage trabecular meshwork in its anterior third, just posterior to the Schwalbe line (Fig. 40.2A). A circumferential incision is then made for about 4 to 5 clock-hours (Fig. 40.2B), and the knife or needle is carefully and quickly withdrawn from the eye over iris tissue at all times. The incision should be superficial, with no grating or scraping sensation noted. A deeper cleft, with exposure of whiter tissue may be noted in the wake of the incision, with a widening of the angle, and a posterior movement of peripheral iris in some cases. The assistant may help the surgeon to extend the angle available to goniotomy by rotating the eye clockwise and counterclockwise at the surgeon’s request. After knife (or needle) withdrawal, blood often egresses from the angle incision, stopping when the chamber is refilled with balanced salt solution; placing a sterile air bubble can assist in assessing the anterior chamber the next morning. A single suture of 10-0 Vicryl secures the corneal wound (37,51).
Postoperative treatment includes the use of topical antibiotic, steroid, and miotic agents. (Miotics are often omitted, however, in cases of uveitic glaucoma.) The baby’s head should be kept elevated (a car seat works well for this), and the eye should be shielded for 1 to 2 nights, until any hyphema has settled. If bilateral goniotomies are needed, they may be performed in a single anesthesia session, as long as all instruments are sterilized or replaced; all drapes, gowns, and gloves are replaced; and the fellow eye is reprepared and draped in sterile fashion after the first procedure (52).
Mild to moderate hyphemas commonly occur after goniotomy, but they almost always clear rapidly without sequelae over several days. Other complications after goniotomy are rare and include iridodialysis, cyclodialysis, the appearance of small peripheral anterior synechiae in the incised angle, damage to the crystalline lens, and retinal detachment in eyes with high myopia (42,52).
The results of goniotomy should be evaluated weekly in the immediate postoperative period and are often evident by 3 to 6 weeks. Gonioscopy after successful goniotomy often reveals a widened angle in the previous incision site, with improved visibility of the ciliary band and scleral spur (Fig. 40.3). Scattered peripheral anterior synechiae may sometimes develop in the bed of the goniotomy and may even partly obscure a view of the incised angle. Because 4 to 5 clock-hours of angle tissue are incised with a single goniotomy, repeated procedures in untreated portions of the angle may enhance pressure control in selected cases. Goniotomy may fail to control infantile glaucoma in some instances because of improper placement and depth of the angle incision, or the obliteration of the incision by peripheral synechiae. In approximately 10% of cases, if the first two procedures have produced substantial but still inadequate IOP reduction, a third goniotomy procedure may help further lower the IOP (1).
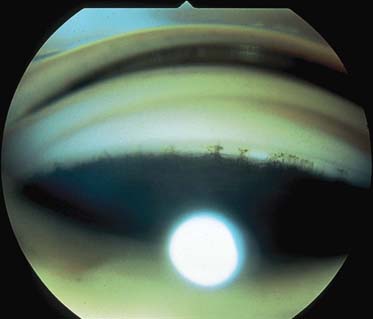
Figure 40.3 Cleft in angle after goniotomy, resulting in a widened angle to the right half of the gonioscopic view in a black infant with primary congenital glaucoma.
The success of goniotomy in controlling glaucoma varies with the cause of the glaucoma. The best results—80% to more than 90% success after one to two procedures—are achieved in infants with primary congenital glaucoma presenting between 3 months and 1 year of age (1,53). Others report lower success of closer to 70% after one to two procedures (54). In one study of seven infants treated with two simultaneous goniotomies in one eye and a single goniotomy in the fellow eye, no significant differences were noted in the results (55). Success rates with goniotomy (and angle surgery in general) are much lower for cases of primary congenital–infantile glaucoma presenting at birth or after 12 months of age (success in these groups is usually about 30% to 50%) (1,37,53).
Procedures Related to Goniotomy (Historical Perspective)
Scheie reported a modification of goniotomy, goniopuncture, which involved passage of a goniotomy knife through the trabecular meshwork and sclera to the subconjunctival space after standard goniotomy (56,57). Scarring of the limbal incision limited the usefulness of goniopuncture.
The Nd:YAG (neodymium:yttrium–aluminum–garnet) laser has been used to perform trabeculopuncture by directing laser energy gonioscopically at the trabecular meshwork, to penetrate through to the Schlemm canal. Success was reported with this procedure in six of eight eyes with juvenile glaucoma over a 6-month follow-up period (58). A technique requiring a large limbal incision, direct goniotomy has also been described, but it has been superseded by trabeculotomy (see later) (59).
Trabeculodialysis, a modification of goniotomy in which the trabecular meshwork is scraped or retracted from the scleral sulcus after a standard goniotomy incision, has been effective in the treatment of children with glaucoma secondary to anterior uveitis (60% pressure control reported in a series of 23 such patients) (39). Goniotomy alone is also effective in these patients (37,40).
Argon laser trabeculoplasty is ineffective in the treatment of childhood glaucomas and is not feasible to perform in young patients (60,61).
Trabeculotomy Ab Externo
The surgical technique of trabeculotomy ab externo is performed by cannulating the Schlemm canal from an external approach and then tearing through the trabecular meshwork into the anterior chamber. This procedure thus creates a direct communication between the anterior chamber and Schlemm canal. Burian and Smith independently described trabeculotomy ab externo in 1960 as an alternative procedure to goniotomy (62,63). The initial technique was later modified by Harms, Dannheim, and McPherson (1). Success rates varying from 73% to 100% have been reported for this procedure in congenital glaucoma (1). In a series of 140 eyes (89 children) with developmental glaucoma treated with trabeculotomy surgery, overall success was 89% after an average follow-up of 9.5 years (64). While conjunctival scarring and a longer surgical duration are the salient disadvantages of trabeculotomy (compared with goniotomy), this procedure is little affected by an edematous or scarred cornea. (Additional comparison of these two angle procedures follows.)
Basic Technique
In the surgical technique described by McPherson (65), a limbal-based conjunctival flap and a partial-thickness triangular or rectangular scleral flap are created as for standard trabeculectomy (see Chapter 38). Most surgeons prefer to perform trabeculotomy under a small fornix-based conjunctival peritomy. Preoperative use of pilocarpine helps to induce miosis, and use of topical apraclonidine may reduce intraoperative bleeding. An inferotemporal approach for trabeculotomy is suggested (unless combined trabeculectomy is planned) to spare the superior quadrants for possible later filtration or other surgery.
A radial scratch incision is made in the bed of the scleral flap across the sclerolimbal junction. This scratch incision is gradually deepened under high magnification until the Schlemm canal is identified just anterior to the circumferential fibers of the scleral spur (near the posterior aspect of the limbal “gray zone”). Often a small amount of blood or aqueous humor refluxes through the cut ends of the Schlemm canal, and the internal wall of the canal appears slightly pigmented. At this point (or earlier, if preferred, or if the anterior chamber is inadvertently entered before the Schlemm canal is identified), a paracentesis should be made, with injection into the anterior chamber of a small amount of viscoelastic recommended. To confirm the identity of the canal, a 6-0 gauge suture (Prolene with a cautery-blunted tip is recommended) should thread easily to both the left and the right sides of the radial incision. If resistance is met, the suture may need to be repositioned, the radial incision deepened, or a second parallel radial incision made beneath the same scleral flap to assist in finding the Schlemm canal (the presence of the suture in Schlemm canal may sometimes be confirmed by gonioscopy by using a Zeiss four-mirror lens). After the canal has been located, the internal arm of a trabeculotome should be passed gently into the canal (to the right side first for a right-handed surgeon) as far as possible without meeting excessive resistance, and by using the parallel external arm as a guide (Fig. 40.4A). The internal arm is then gently rotated into the anterior chamber, with care to avoid entry into peripheral cornea or beneath the iris plane (Fig. 40.4B). Rotation of the trabeculotome into the anterior chamber tears through the intervening trabecular meshwork and requires little force (Fig. 40.4B, C). Rotation should be halted once about 75% to 80% of the internal arm of the trabeculotome is visible in the anterior chamber. The anterior chamber may shallow slightly, and blood may egress from the torn trabecular meshwork and Schlemm canal as the trabeculotome is removed from the eye along its path of entry. In similar fashion, the trabeculotome should be placed into the left side of the radial incision and the procedure repeated to the left. Leaving a portion of intact trabecular meshwork underlying the radial incision into the Schlemm canal helps prevent prolapse of iris into the wound. The scleral flap is then sutured with 10-0 Vicryl. If a limbus-based conjunctival flap was used, the flap may be closed with a running suture of 8-0 Vicryl as for standard trabeculectomy (66). Alternatively, wing sutures of 10-0 Vicryl often suffice for watertight closure of a fornix-based conjunctival flap. Subconjunctival antibiotic and short-acting steroid may be given at the end of the surgery.
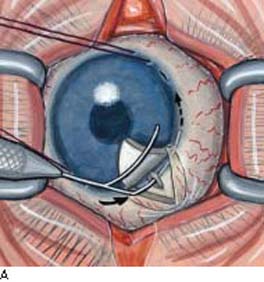
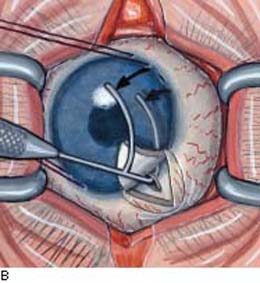

Figure 40.4 Trabeculotomy under a fornix-based conjunctival and partial-thickness scleral flap. Preferred inferotemporal approach is shown, using a traction suture at the limbus to help hold the eye in adduction. A: Placement of trabeculotome into the cut end of Schlemm canal to the right. B: Rotation of the trabeculotome into the anterior chamber, tearing through the intervening trabecular meshwork. C: View of internal arm of trabeculotome tearing through trabecular meshwork as the instrument is rotated into the anterior chamber.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


