Glaucomas Associated with Disorders of the Lens
Several disorders of the crystalline lens are associated with various forms of glaucoma. In some cases, such as the exfoliation syndrome (see Chapter 15), a cause-and-effect relationship between the lenticular abnormality and the glaucoma is uncertain. In other situations, including some forms of dislocated lenses and cataracts, the glaucoma is more clearly a result of the alteration in the lens.
GLAUCOMAS ASSOCIATED WITH DISLOCATION OF THE LENS
Terminology
Several terms have been applied to the clinical situation in which the crystalline lens is displaced from its normal, central position behind the iris. Subluxation of the lens implies an incomplete dislocation in which the lens is still at least partially behind the iris but is tilted or displaced slightly in an anterior or a posterior direction or perpendicular to the optical axis. With complete dislocation, the entire lens may be in the anterior chamber or may have fallen posteriorly into the vitreous cavity. The term ectopia of the lens, or ectopia lentis, is also applied to cases of lens dislocation, but it is nonspecific with regard to the degree of lens displacement.
Subluxation or complete dislocation of the lens may be associated with a number of clinical conditions, all of which can lead to glaucoma by a variety of mechanisms. We first review the more common clinical forms of ectopia lentis and then consider the mechanisms by which these conditions may lead to intraocular pressure (IOP) elevation and how these glaucomas are managed.
Clinical Forms of Ectopia Lentis
Traumatic Dislocation
Trauma is the most common cause of a displaced lens (1,2) (Fig. 18.1). In one series of 166 cases, injury was reported to account for 53% of the total group (2).
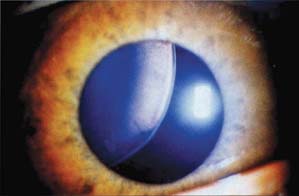
Figure 18.1 Dislocation or subluxation of the lens can result from various disorders that can lead to glaucoma. In this case, the lens is dislocated superotemporally in a patient with ectopia lentis et papillae, which is characterized by small, subluxed lenses and oval or slit-like pupils that are displaced in the opposite direction of the lens.
Exfoliation Syndrome
The exfoliation syndrome can be associated with spontaneous or traumatic lens subluxation or dislocation (see Chapter 15).
Simple Ectopia Lentis
Dislocation of the lens may occur without associated ocular or systemic abnormalities as a congenital anomaly or as a spontaneous disorder later in life (3). Both forms are typically inherited by an autosomal dominant mode (3). The condition is usually bilateral and symmetrical, with lens dislocation generally upward and outward and occasionally into the anterior chamber. Associated problems include glaucoma and retinal detachment.
Ectopia Lentis et Pupillae
Ectopia lentis et pupillae is a rare, autosomal recessive condition characterized by small, subluxated lenses and by oval or slit-shaped pupils that are displaced, usually in the opposite direction from that of the lens (3) (Fig. 18.2). The condition is associated with a wide variety of other ocular abnormalities, including severe axial myopia with related fundus changes, enlarged corneal diameters, iris transillumination defects, poor pupillary dilation, persistent pupillary membranes, iridohyaloid adhesions, prominent iris processes, cataracts, retinal detachment, and glaucoma (4). The condition is usually bilateral, although marked variation may be seen between eyes of the same patient. The pathogenesis of this disorder is unknown, but an ultrasound biomicroscopic study of an affected patient demonstrated a lack of definition of the ciliary processes except in the quadrant toward which the pupil was displaced and a membrane-like structure extending from the proximal pupillary margin over the tips of the ciliary processes to a more posterior origin (5). The investigators proposed a localized abnormality of the secondary vitreous with persistence of the marginal bundle of Drualt, resulting in a mechanical tethering of the iris or pupil margin to the vitreous base or anterior vitreous face and localized zonular disruption. Others have suggested a neuroectodermal defect resulting in hypoplasia or absence of the posterior pigment epithelium layer and dilator muscle of the iris or a mesodermal defect with persistence of the anterior and lateral elements of the tunica vasculosa lentis (4). The ultrasound biomicroscopy findings are consistent with histopathologic case reports in the German literature from the beginning of the past century (6–8).

Figure 18.2 Patient with ectopia lentis et pupillae, showing typical displacement of pupils.
It has been suggested that simple ectopia lentis may be an incomplete expression of ectopia lentis et pupillae, because both may occur in the same family and have peripheral iris transillumination (4). Some patients with ectopia lentis et pupillae may have mild systemic changes suggestive of Marfan syndrome.
Marfan Syndrome
This autosomal dominant disorder is characterized by a tall, slender individual with long, slender fingers and toes (i.e., arachnodactyly) and frequent cardiovascular disease (3). Marfan syndrome and ectopia lentis have been linked to a single fibrillin gene on chromosome 15, and arachnodactyly was linked to the fibrillin gene on chromosome 5 (9). In a review of 160 consecutive patients, the most striking ocular abnormality was enlargement of the globe, presumably caused by scleral stretching (10). The lens was dislocated in 193 of the eyes, and this correlated with increased ocular axial length, suggesting that stretching and rupture of the zonular fibers lead to the dislocation. The ectopia lentis typically appears in the fourth to fifth decade of life and is rarely complete, but it is usually seen as an upward subluxation (Fig. 18.3). Bilateral spontaneous lens dislocation has been described in early childhood with associated glaucoma (11). Glaucoma may result from the lens dislocation, but it is also associated with surgical aphakia or occurs as an anomaly of the anterior chamber angle. In one review of 573 patients, 29 (5%) had glaucoma, and the most common mechanisms were chronic open angle and glaucoma following lens extraction or scleral buckling procedure (12). Retinal detachment is also a common finding in the phakic or aphakic eye of a patient with Marfan syndrome.

Figure 18.3 Upward lens subluxation in a patient with Marfan syndrome.
Homocystinuria
Patients with homocystinuria may resemble those with Marfan syndrome in habitus and ocular problems, but they differ by having an autosomal recessive inheritance pattern and frequently having mental retardation (3,13). Homocystinuria may result from one of several enzyme deficiencies in homocysteine metabolism. The diagnosis can be confirmed by the demonstration of homocysteine in the urine. The differentiation between Marfan syndrome and homocystinuria is important because the patient with homocystinuria is subject to thromboembolic episodes, which can lead to death in early adulthood and creates a significant surgical risk. If the condition is diagnosed in a newborn, appropriate dietary treatment and vitamin supplementation can substantially reduce the risk for ocular complications (14). The lens dislocation occurs earlier in life than in the Marfan syndrome and is more often in a downward direction, and complete dislocation into the vitreous or anterior chamber is frequent. Glaucoma is more commonly related to the lens dislocation than is the case with Marfan syndrome. Retinal detachment is a common problem.
One article examined the results of medical versus surgical treatment for lens subluxation or dislocation in a retrospective case series of 45 patients (15). Medical therapy was attempted initially in all patients and was the sole therapy used for five patients. Eighty-two procedures were performed with the patients under general anesthesia, and two surgical complications and one postoperative complication occurred. Lens dislocation into the anterior chamber was the most frequent indication for surgery (50%), followed by pupillary block glaucoma (12%). Prophylactic peripheral iridectomy was not successful in preventing lens dislocation into the anterior chamber in five patients. The investigators recommend that surgical treatment should be considered, especially for cases of repeated lens dislocation into the anterior chamber or pupillary block glaucoma.
Weill–Marchesani Syndrome
Weill–Marchesani syndrome is the antithesis of the aforementioned conditions with respect to habitus; these patients are short and stocky (16,17). The principal features of the syndrome are short fingers (i.e., brachydactyly); muscular hypertrophy; and small, round lenses (i.e., microspherophakia) (Fig. 18.4). Lens dislocation in these patients occurs as frequently as in patients with Marfan syndrome and homocystinuria, and glaucoma is more common than in either of the latter two conditions (18). In his original publication, Marchesani (17) hypothesized that an overdevelopment or hyperplasia of the ciliary body might be the reason for spherophakia. However, an ultrasonographic biomicroscopy study of three patients with this syndrome and normal axial lengths demonstrated that the ciliary body actually appeared smaller than normal (19). The investigators hypothesized that the small ciliary body represents the underlying reason for elongated zonules and that it may be exerting less force on the lens, giving rise to the spherical shape of the lens. An ultrastructural study of the lens from a patient with the Weill–Marchesani syndrome revealed degeneration and necrosis of the epithelial cells and destruction of cortical fibers, which was thought to result, in part, from the trauma and irritation of a highly mobile lens in close contact with the iris (20). The small, round lens in this condition also has loose zonules, and the glaucoma may be related to lens dislocation or a forward shift of the lens, causing pupillary block glaucoma (18), which can be precipitated or aggravated by miotic therapy. Bilateral angle-closure glaucoma has also been reported after mid-dilatation with cyclopentolate in a child with the Weill–Marchesani syndrome but without lens subluxation (21). Angle-closure glaucoma may be treated with laser iridectomy or peripheral iridoplasty depending on the relative proportion of pupillary block as the mechanism of the angle closure (22).

Figure 18.4 Partial lens dislocation in a patient with Weill– Marchesani syndrome. The loose zonules allow the lens to assume a typical, small round shape (i.e., microspherophakia).
Spontaneous Dislocation
In some middle-aged or older individuals, dislocation of the lens may occur spontaneously, usually in association with cataract formation (1). Spontaneous dislocation has also been reported in eyes with high myopia, uveitis, buphthalmos, or megalocornea.
Other Conditions with Associated Ectopia Lentis
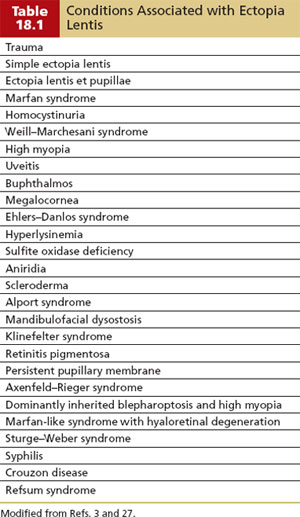
Other rare congenital disorders associated with lens dislocation include Ehlers–Danlos syndrome, hyperlysinemia, sulfite oxidase deficiency, and aniridia. Additional conditions associated with ectopia lentis are included in Table 18.1.
Examination and Investigation
Slitlamp examination may reveal lenticular subluxation and dislocation. If zonules are weak, then phacodonesis or iridodonesis may also be present. Even with these signs, the nature of the accompanying zonular defect may be uncertain. Ultrasonographic biomicroscopy enables in vivo imaging of the zonules and can detect zonular loss and stretching directly (Fig. 18.5) (23). In a study of 18 eyes with clinically suspected zonular abnormalities, ultrasonographic biomicroscopy demonstrated evidence of missing zonules in 11 eyes and evidence of zonular stretch in 11 eyes. All of the eyes examined demonstrated increased lenticular sphericity in the area of the zonular disorder, and nine eyes showed ciliary body flattening.


Figure 18.5 A: Ultrasonographic biomicroscopy showing stretched zonules. B: Ultrasonographic biomicroscopy showing broken zonules with rounding up of the ciliary body and adjacent lens equator.
Mechanisms of Glaucoma Associated with Subluxated or Dislocated Lens
Subluxation or complete dislocation of the lens in any of the aforementioned clinical conditions may lead to glaucoma by various mechanisms. In general, these mechanisms of glaucoma apply to all forms of ectopia lentis.
Pupillary Block
The lens may block aqueous flow through the pupil if it is dislocated into the pupil or anterior chamber or subluxed or tilted forward against the iris without entering the anterior chamber. This mechanism is particularly common with microspherophakia, as in the Weill–Marchesani syndrome, because of loose zonules of the lens. Pupillary block in the latter condition is often worsened by miotic therapy, which allows further relaxation of zonular support, and cycloplegic agents may help by pulling the lens posteriorly. Pupillary block may also be associated with a dislocated lens due to herniation of vitreous into the pupil. Peripheral anterior synechiae may develop from a long-standing pupillary block and produce chronic IOP elevation.
Phacolytic Glaucoma
In some cases, the lens may dislocate completely into the vitreous cavity and later undergo degenerative changes with release of material that obstructs aqueous outflow (24). In one reported case, this condition was associated with retinal perivasculitis, which cleared along with the glaucoma after removal of the lens (25). (Phacolytic glaucoma without dislocation is discussed later in this chapter.)
Concomitant Trauma
In cases of traumatic dislocation of the lens, concomitant trauma to the anterior chamber angle from the initial injury may be the cause of the associated glaucoma (1,3). A transient pressure elevation of uncertain origin may persist for days or weeks after traumatic dislocation of the lens. (The mechanisms of glaucoma associated with trauma are considered in more detail in Chapter 25.)
Management
If the lens is displaced anteriorly in the anterior chamber or partially through the pupil, the condition may be relieved by dilating the pupil and allowing the lens to reposit back into the posterior chamber (26). A miotic agent may then be used to keep the lens behind the iris, but miotic therapy should be avoided when the pupillary block is caused by loose zonules, because contraction of the ciliary muscle further relaxes the zonular support, making the pupillary block worse (27). If the lens is completely dislocated in the anterior chamber, it is probably better to constrict the pupil and surgically remove the lens, rather than letting it fall back into the vitreous. Cycloplegic agents may help to break the attack by pulling the lens posteriorly. Hyperosmotic agents, carbonic anhydrase inhibitors, or topical β-blockers may also be useful in breaking the attack. The definitive treatment, however, is laser iridotomy (or incisional iridectomy, if necessary). The iridotomy should be placed peripherally to avoid subsequent obstruction by the lens. Prophylactic iridotomy in cases of microspherophakia has also been advocated to avoid pupillary block glaucoma (27). Laser peripheral iridoplasty may also be helpful in some cases of angle-closure glaucoma without a significant pupillary block component (22). The extraction of a subluxated lens is associated with increased surgical risk and should usually be avoided unless the lens is in the anterior chamber or lens extraction is needed to relieve the glaucoma or improve vision.
Phacolytic Glaucoma
Phacolytic glaucoma is the only situation in cases of lens dislocation in which cataract extraction is the procedure of choice (28). Subluxated lenses can be successfully removed through a pars plana approach with vitreous instruments (25).
Chronic Glaucomas
Chronic glaucoma due to peripheral anterior synechiae or concomitant trauma in eyes with dislocated lenses is generally managed by standard medical measures. Laser trabeculoplasty has a low success rate in eyes with open-angle glaucoma associated with trauma, although this approach is often reasonable to try when medical therapy is no longer adequate before recommending incisional surgical intervention.
GLAUCOMAS ASSOCIATED WITH CATARACT FORMATION
It has long been recognized clinically that several forms of glaucoma may occur in association with the formation of cataracts. However, an incomplete understanding of the various mechanisms for these glaucomas has led to a plethora of terms and considerable controversy and confusion. Later observations have provided new explanations and terminology for several of the glaucomas associated with cataract formation.
Phacolytic (Lens Protein) Glaucoma
Terminology
In 1900, Gifford (29) described a form of open-angle glaucoma associated with a hypermature cataract. Among the terms subsequently suggested for this condition were phacogenic glaucoma and lens-induced uveitis (30,31). Flocks and colleagues (32) reported histologic findings suggesting that the glaucoma-inducing mechanism was a macrophagic response to lens material. They proposed that this condition be called phacolytic glaucoma, which is the term most often used today. However, Epstein and colleagues (33,34) have provided evidence that high-molecular-weight lens protein may be primarily responsible for the obstruction to aqueous outflow in this disorder, and the term lens protein glaucoma has been suggested (35).
Clinical Features
The typical patient presents with an acute onset of monocular pain and redness. There is usually a history of gradual reduction in visual acuity over the preceding months or years. Vision at the time of presentation may be reduced to light perception. The examination reveals a high IOP, conjunctival hyperemia, and diffuse corneal edema. The anterior chamber angle is open and usually grossly normal. A heavy flare is typically seen in the anterior chamber and is often associated with iridescent or hyperrefringent particles (Fig. 18.6). The latter have been variably reported to represent calcium oxalate or cholesterol crystals and are a helpful diagnostic sign in phacolytic glaucoma (36–38). Chunks of white material may also be seen in the aqueous and on the anterior lens capsule and corneal endothelium. In five cases, specular microscopy revealed regular, round cells, about three times the size of an erythrocyte, which were found by histologic study of aqueous aspirates to represent macrophages (37). Rare cases of vitreous opacification have been reported (39). The opacities were observed at the time of cataract surgery and resolved spontaneously over 12 weeks. The cataract is typically mature and opaque (Fig. 18.7A) or hypermature (i.e., liquid cortex), but it may, rarely, be immature. A less common variation of phacolytic glaucoma is the previously discussed situation in which the lens has dislocated into the vitreous and undergone phacolysis (Fig. 18.7B). The latter cases differ clinically in that the glaucoma tends to be more subacute.

Figure 18.6 High-magnification slitlamp view showing iridescent particles in the aqueous in a patient with phacolytic glaucoma. The white, cloudy cornea is seen to the right, and the dark iris to the left, of the photograph. (Courtesy of L. Frank Cashwell Jr, MD.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


