Table 4.1 Classification of uveitis entities
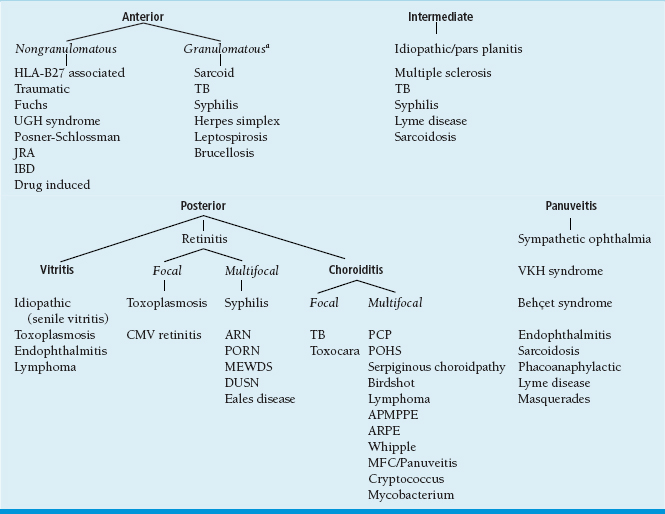
aGranulomatous uveitis can always present with nongranulomatous findings initially.
APMPPE, acute posterior multifocal placoid pigment epitheliopathy; ARN, acute retinal necrosis; ARPE, acute retinal pigment retinopathy; CMV, cytomegalovirus; DUSN, diffuse unilateral subacute neuroretinitis; IBD, inflammatory bowel disease; JRA, juvenile rheumatoid arthritis; MEWDS, multiple evanescent white dot syndrome; MFC, multifocal choroiditis; PCP, pneumocystis pneumoniae choroiditis; PORN, progressive outer retinal necrosis; POHS, presumed ocular histoplasmosis syndrome; TB, tuberculosis; UGH, uveitis-glaucoma-hyphema; VKH, Vogt-Koyanagi-Harada.
aFrom Kimura SJ, Thygeson P, Hogan MJ. Signs and symptoms of uveitis, I: anterior Uveitis. Am J Ophthalmol 1959;47:155–170, with permission.
bFrom Kimura SJ, Thygeson P, Hogan MJ. Signs and symptoms of uveitis, II: classification of the posterior manifestations of uveitis. Am J Ophthalmol 1959;47:171–176, with permission.
Hla-B27–Associated Diseases
Summary
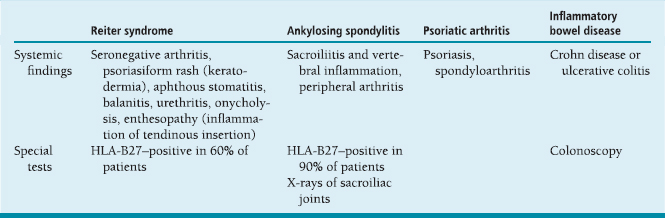
The HLA-B27 antigen is associated with a number of systemic and ocular inflammatory conditions including Reiter syndrome, ankylosing spondylitis, psoriatic arthritis, and inflammatory bowel disease (Table 4.3; Figure 4.1).
Signs and Symptoms
Photophobia.
Sudden onset.
Unilateral (can alternate between eyes).
Demographics
Caucasian men.
Ophthalmic Findings
Recurrent episodes of iridocyclitis; can be severe with fibrin, hypopyon (Figure 4.1).
Posterior synechiae.
Nongranulomatous keratic precipitates.
Decreased intraocular pressure (IOP).
Macular edema common.
Disease Course
May spontaneously resolve.
Recurrent episodes common.
Treatment and Management
Intensive topical corticosteroids.
In severe cases, periocular or oral steroids may be needed.
Cycloplegics.
Etiology
 Unknown.
Unknown.
 Cross-reactivity of the HLA-B27 antigen and bacterial antigens (molecular mimicry).
Cross-reactivity of the HLA-B27 antigen and bacterial antigens (molecular mimicry).
References
Rodriguez A, Akova YA, Pedroza-Seres M, et al. Posterior segment ocular manifestations in patients with HLA-B27-associated uveitis. Ophthalmology 1994;101:1267–1274.
Tay-Kearney ML, Schwam BL, Lowder C, et al. Clinical features and associated systemic diseases of HLA-B27 uveitis. Am J Ophthalmol 1996;121:47–56.
Wakefield D, Montanaro A, McCluskey P. Acute anterior uveitis and HLA-B27. Surv Ophthalmol 1991;36:223–233.
Plasmoid(orplastic)aqueous: descriptive term for anterior chamber fluid containing so much protein that the cells are suspended and do not move with the normal convection currents. HLA-B27–associated uveitis is one of the most common causes.
Posner-Schlossman Syndrome
Other name: glaucomatocyclitic crisis.
Summary
Posner-Schlossman syndrome is a rare condition characterized by recurrent episodes of high IOP with mild iridocyclitis.
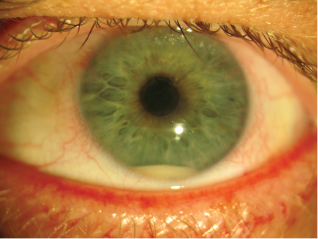
FIGURE 4.1. Severe HLA-B27–associated iridocyclitis with a plasmoid aqueous and hypopyon. (Courtesy of David Hinkle, MD.)
Etiology
Unknown.
Signs and Symptoms
Mild blurred vision.
Mild discomfort.
Many patients have very few symptoms.
Demographics
Ages, 20 to 40 years; rare in elderly individuals.
Men more often than women.
Ophthalmic Findings
Usually unilateral, acute attacks.
IOP greater than 40 mm Hg with accompanying corneal edema.
Few small, nongranulomatous keratic precipitates.
Mild anterior chamber inflammation.
Open-angle glaucoma.
No posterior synechiae.
Systemic Findings
None.
Special Tests
None.
Pathology
None.
Disease Course
 Resolution in 1 to 3 weeks with or without treatment.
Resolution in 1 to 3 weeks with or without treatment.
 Complications: glaucomatous damage to optic nerve.
Complications: glaucomatous damage to optic nerve.
Antiglaucoma medications.
Topical corticosteroids.
Glaucoma surgery in rare cases.
Differential Diagnosis
 Acute angle-closure glaucoma (closed angle, corneal edema, and severe pain).
Acute angle-closure glaucoma (closed angle, corneal edema, and severe pain).
 Fuchs heterochromic iridocyclitis (mild IOP elevation, iris heterochromia, stellate keratic precipitates).
Fuchs heterochromic iridocyclitis (mild IOP elevation, iris heterochromia, stellate keratic precipitates).
 Herpetic uveitis (decreased corneal sensation, increased IOP, keratitis, iris atrophy).
Herpetic uveitis (decreased corneal sensation, increased IOP, keratitis, iris atrophy).
Reference
Harstad HK, Ringvold A. Glaucomatocyclitic crises (Posner-Schlossman syndrome): a case report. Acta Ophthalmol Scand Suppl 1986;64:146–151.
Phacoantigenic Uveitis
Other names: phacoanaphylactic endophthalmitis, phacoanaphylactic uveitis.
Summary
Phacoantigenic uveitis is a granulomatous reaction to lens proteins occurring following injury to the lens capsule and leakage of lens proteins into the anterior chamber.
Etiology
 Autoimmunity to lens proteins that are normally sequestered and unrecognized by the immune system.
Autoimmunity to lens proteins that are normally sequestered and unrecognized by the immune system.
 May have history of penetrating lens injury, rupture of the lens capsule, or retained lens fragments following cataract surgery.
May have history of penetrating lens injury, rupture of the lens capsule, or retained lens fragments following cataract surgery.
Ophthalmic Findings
Chronic granulomatous anterior uveitis.
Lens capsular disruption or retained lens material.
Systemic Findings
None.
Special Tests
Anterior chamber aspirate for cultures and smears to exclude an intraocular infection.
Pathology
Zonal granuloma:
Inner zone of neutrophils adjacent to lens material.
Middle zone of monocytes, macrophages, giant cells.
Outer zone of granulation tissue with plasma cells.
Disease Course
Chronic smoldering inflammation, may resemble a low-grade endophthalmitis.
Treatment and Management
 Topical, periocular corticosteroids: temporizing measure to decrease inflammation.
Topical, periocular corticosteroids: temporizing measure to decrease inflammation.
 Surgical removal of lens fragments: definitive treatment.
Surgical removal of lens fragments: definitive treatment.
Differential Diagnosis
Phacolytic glaucoma: caused by leakage of lens proteins from hypermature lens.
Chronic endophthalmitis: consider organisms such as Propionibacterium acnes and other indolent bacteria and fungi.
References
Filipe JC, Palmares J, Delgado L, et al. Phacolytic glaucoma and lens-induced uveitis. Int Ophthalmol 1993;17: 289–293.
Thach AB, Marak GE Jr, McLean IW, et al. Phacoanaphylactic endophthalmitis: a clinicopathologic review. Int Ophthalmol 1991;15:271–279.
Uveitis-Glaucoma-Hyphema Syndrome
Summary
Uveitis-glaucoma-hyphema (UGH) syndrome is a rare condition related to ill-fitting intraocular lenses (IOLs) causing uveal irritation.
Etiology
Chronic uveal irritation caused by a poorly fitting IOL.
Signs and Symptoms
Ocular tenderness.
Decreased vision.
Ophthalmic Findings
Anterior uveitis, rarely with a hypopyon.
Hyphema.
Glaucoma.
IOL (usually poorly fitting anterior chamber lens, iris-fixated IOL, single-piece IOL placed in ciliary sulcus, or IOL within capsular bag with zonular laxity).
Iridodenesis, transillumination frequently seen if posterior chamber IOL.
Systemic Findings
None.
None.
Disease Course
Chronic, recurrent episodes of inflammation.
Treatment and Management
Medical management occasionally is sufficient.
IOL explant/exchange/repositioning.
Medications
Antiglaucoma medications.
Anti-inflammatory medications.
Differential Diagnosis
Endophthalmitis.
Lens-induced uveitis.
HLA-B27–associated uveitis.
References
Beehler CC. UGH syndrome with the 91Z lens. J Am Intraocul Implant Soc 1983;9:459.
Choyce DP. Complications of the AC implants of the early 1950’s and the UGH or Ellingson syndrome of the late 1970’s. J Am Intraocul Implant Soc 1978;4:22–29.
Percival SP, Das SK. UGH syndrome after posterior chamber lens implantation. J Am Intraocul Implant Soc 1983;9:200–201.
Causes of Uveritis with Hyphema
 HLA-B27-associated uveitis.
HLA-B27-associated uveitis.
 Varicella-zoster virus (VZV).
Varicella-zoster virus (VZV).
 Herpes simplex virus (HSV).
Herpes simplex virus (HSV).
 Postoperative endophthalmitis.
Postoperative endophthalmitis.
 UGH syndrome.
UGH syndrome.
 Behcet syndrome.
Behcet syndrome.
 Fuchs heterochromic iridocyclitis.
Fuchs heterochromic iridocyclitis.
Viral Diseases
Summary
The most common viral origins causing iridocyclitis are HSV and VZV. These frequently have other signs indicative of a concurrent or prior herpes virus infection.
Signs and Symptoms
Unilateral pain, photophobia, redness, decreased vision.
Ophthalmic Findings
 Granulomatous, nongranulomatous, or stellate keratic precipitates.
Granulomatous, nongranulomatous, or stellate keratic precipitates.
 Diffuse distribution of keratic precipitates or concentrated under area of keratitis.
Diffuse distribution of keratic precipitates or concentrated under area of keratitis.
 Hypopyon.
Hypopyon.
 Elevated IOP.
Elevated IOP.
 Evidence of previous ocular herpes infections:
Evidence of previous ocular herpes infections:
Epithelial dendrite.
Stromal keratitis or scarring.
Corneal hypoesthesia.
Iris atrophy (Figure 4.2).
Irregular pupil.
Anterior uveitis.
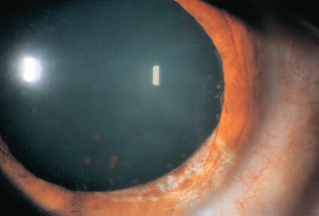
FIGURE 4.2. Varicella zoster can cause an occlusive vasculitis resulting in segmental iris atrophy.
Systemic Findings
 Skin rash affecting V1 dermatome (Hutchinson sign) (varicella zoster).
Skin rash affecting V1 dermatome (Hutchinson sign) (varicella zoster).
 Periocular blisters, cold sores (herpes simplex).
Periocular blisters, cold sores (herpes simplex).
Treatment and Management
 Topical corticosteroid drops.
Topical corticosteroid drops.
 Cycloplegia.
Cycloplegia.
 Acyclovir: the use of antivirals in isolated iridocyclitis is controversial. The Herpetic Eye Disease Study showed a trend toward improvement with acyclovir, but did not recruit enough patients in this subgroup to show statistical significance.
Acyclovir: the use of antivirals in isolated iridocyclitis is controversial. The Herpetic Eye Disease Study showed a trend toward improvement with acyclovir, but did not recruit enough patients in this subgroup to show statistical significance.
References
The Herpetic Eye Disease Study Group. A controlled trial of oral acyclovir for iridocyclitis caused by herpes simplex virus. Arch Ophthalmol 1996;114:1065–1072.
Wilhelmus KR, Dawson CR, Barron BA, et al. Risk factors for herpes simplex virus epithelial keratitis recurring during treatment of stromal keratitis or iridocyclitis: Herpetic Eye Disease Study Group. Br J Ophthalmol 1996;80: 969–972.
 HSV.
HSV. VZV.
VZV. Posner-Schlossman syndrome.
Posner-Schlossman syndrome. Sarcoidosis.
Sarcoidosis. Fuchs heterochromic iridocyclitis.
Fuchs heterochromic iridocyclitis.Uveitis with Diffusely Distributed Keratic Precipitates
 HSV.
HSV.
 VZV.
VZV.
 Sarcoidosis.
Sarcoidosis.
 Fuchs heterochromic iridocyclitis.
Fuchs heterochromic iridocyclitis.
 Toxoplasmosis.
Toxoplasmosis.
Juvenile Idiopathic Arthritis (Chronic Arthritis of Children)
Summary
Juvenile idiopathic arthritis (JIA) encompasses several forms of childhood arthritis. Young girls with pauciarticular arthritis most frequently develop iridocyclitis.
Etiology
Unknown.
Signs and Symptoms
Usually asymptomatic.
Demographics
Young girls predominantly, onset usually less than 16 years of age.
Ophthalmic Findings
 Bilateral chronic, nongranulomatous iridocyclitis.
Bilateral chronic, nongranulomatous iridocyclitis.
 Frequently develop band keratopathy (Figure 4.3), posterior synechiae, cataracts, and glaucoma.
Frequently develop band keratopathy (Figure 4.3), posterior synechiae, cataracts, and glaucoma.
Systemic Findings
Monoarticular or pauciarticular arthritis more common than polyarticular arthritis.
Special Tests
Rheumatoid factor negative.
Antinuclear antibody (ANA) positive (60%).
Disease Course
Chronic smoldering inflammation leading to complications such as band keratopathy, cataracts, glaucoma, and hypotony.
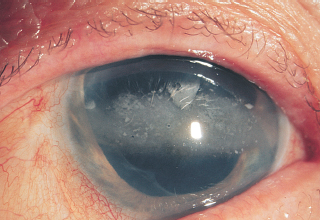
FIGURE 4.3. Chronic ocular inflammation resulting in band keratopathy in a patient with juvenile rheumatoid arthritis. (From Tasman W, Jaeger E. The Wills Eye Hospital atlas of clinical ophthalmology, 2nd ed. Lippincott Williams & Wilkins, 2001.)
Treatment and Management
 Topical, periocular, or systemic corticosteroids, cycloplegia, immunosuppressive agents.
Topical, periocular, or systemic corticosteroids, cycloplegia, immunosuppressive agents.
 Surgical removal of cataracts, lens implantation is controversial and historically contraindicated.
Surgical removal of cataracts, lens implantation is controversial and historically contraindicated.
Medications
 Topical and periocular corticosteroids.
Topical and periocular corticosteroids.
 Immunosuppression if intolerant or resistant to steroids.
Immunosuppression if intolerant or resistant to steroids.
References
Giannini EH, Malagon CN, Van Kerckhove C, et al. Longitudinal analysis of HLA associated risks for iridocyclitis in juvenile rheumatoid arthritis. J Rheumatol 1991;18:1394–1397.
Wolf MD, Lichter PR, Ragsdale CG. Prognostic factors in the uveitis of juvenile rheumatoid arthritis. Ophthalmology 1987;94:1242–1248.
Traumatic Iritis
Summary
Blunt trauma to the eye can disrupt the blood–ocular barrier causing an anterior iridocyclitis.
Signs and Symptoms
Pain, redness, photophobia immediately or several days following blunt injury to the eye.
Ophthalmic Findings
Mild iridocyclitis.
Hypopyon (rare).
Middilated, sluggish pupil.
Decreased IOP.
 Usually resolves quickly.
Usually resolves quickly.
Treatment and Management
 Rule out ruptured globe and corneal abrasion.
Rule out ruptured globe and corneal abrasion.
 Topical corticosteroids (may not be needed in mild cases).
Topical corticosteroids (may not be needed in mild cases).
 Cycloplegia.
Cycloplegia.
 Check for angle recession, iridodialysis, or cyclodialysis on subsequent visits.
Check for angle recession, iridodialysis, or cyclodialysis on subsequent visits.
Fuchs Heterochromic Iridocyclitis
Summary
Fuchs heterochromic iridocyclitis is a unilateral, chronic low-grade inflammatory condition characterized by stellate keratic precipitates, cataract formation, glaucoma, and iris heterochromia.
Etiology
Unknown.
Syndrome likely related to multiple infectious agents including toxoplasmosis and rubella, among others.
Signs and Symptoms
Usually none.
Ophthalmic Findings
 Iris heterochromia: lighter iris color in brown eyes; darker blue in blue eyes (Figure 4.4).
Iris heterochromia: lighter iris color in brown eyes; darker blue in blue eyes (Figure 4.4).
 Stellate keratic precipitates, diffusely distributed over cornea.
Stellate keratic precipitates, diffusely distributed over cornea.
 Cataracts.
Cataracts.
 Mild, low-grade iritis, anterior vitreous cells, and opacities.
Mild, low-grade iritis, anterior vitreous cells, and opacities.
 Abnormal-angle vessels, predisposed to bleeding and hyphema formation (Amsler sign) during ocular surgery.
Abnormal-angle vessels, predisposed to bleeding and hyphema formation (Amsler sign) during ocular surgery.
 Glaucoma.
Glaucoma.
 Usually unilateral, but rarely bilateral.
Usually unilateral, but rarely bilateral.

FIGURE 4.4. Iris heterochromia in the affected right eye. Loss of iris stroma results in a deeper blue. (Courtesy of Brian Forbes, MD.)
Disease Course
Chronic, low-grade inflammation.
Development of cataracts and glaucoma.
Treatment and Management
Steroids of limited use.
Differential Diagnosis
Herpetic iridocyclitis.
Posner-Schlossman syndrome.
Neovascular glaucoma.
References
Jones NP. Fuchs’ heterochromic uveitis: an update. Surv Ophthalmol 1993;37:253–272.
La Hey E, de Jong PT, Kijlstra A. Fuchs’ heterochromic cyclitis: review of the literature on the pathogenetic mechanisms. Br J Ophthalmol 1994;78:307–312.
Quentin CD, Reiber H. Fuchs heterochromic cyclitis: rubella virus antibodies and genome in aqueous humor. Am J Ophthalmol 2004;138:46–54.
Summary
Intermediate uveitis is a broad descriptive term for inflammation primarily affecting the vitreous and peripheral retina. A number of diseases can cause findings consistent with intermediate uveitis.
Etiology
 Pars planitis: idiopathic.
Pars planitis: idiopathic.
 Inflammatory:
Inflammatory:
Sarcoidosis.
Inflammatory bowel disease.
Multiple sclerosis.
Autoimmune (associated with HLA-DR locus).
 Infectious:
Infectious:
Lyme disease.
Toxocariasis (unilateral disease).
Whipple disease.
Syphilis.
Tuberculosis (TB).
Signs and Symptoms
Floaters.
Decreased vision.
Ophthalmic Findings
Diffuse vitreous cells.
Peripheral vascular sheathing.
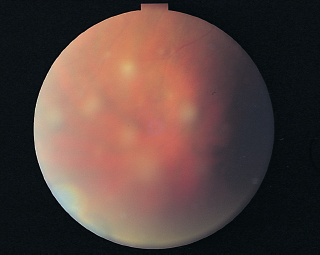
Pars plana “snowballs” or “snowbanks” (Figure 4.5).
Vitreous hemorrhage.
Cystoid macular edema.
Cataracts.
Retinal neovascularization.
Disease Course
 Extremely variable course: Some patients may have smoldering inflammation and retain good vision.
Extremely variable course: Some patients may have smoldering inflammation and retain good vision.
 Others progress to cyclitic membranes, retinal detachment (RD), and phthisis.
Others progress to cyclitic membranes, retinal detachment (RD), and phthisis.
Treatment and Management
Cryotherapy or peripheral laser photocoagulation.
Periocular and oral corticosteroids.
Immunosuppression (cyclosporine, azathioprine, methotrexate) if patient fails therapy or becomes intolerant to steroids.
Sarcoidosis
Summary
Sarcoidosis is an inflammatory condition characterized by noncaseating granulomas in multiple tissues. Ocular involvement is most frequently evident as granulomatous anterior uveitis or intermediate uveitis.
Demographics
 Sarcoid is more common in African Americans.
Sarcoid is more common in African Americans.
 Ocular inflammatory disease occurs in 25% to 50% of patients with systemic sarcoid.
Ocular inflammatory disease occurs in 25% to 50% of patients with systemic sarcoid.
 Ages, 20 to 50 years.
Ages, 20 to 50 years.
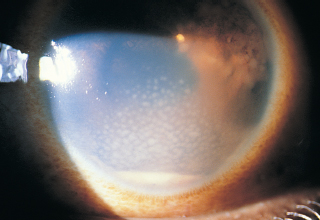
FIGURE 4.6. In granulomatous uveitis, large, greasy-appearing keratic precipitates can frequently be found in Arlt’s triangle. (From Tasman W, Jaeger E. The Wills Eye Hospital atlas of clinical ophthalmology, 2nd ed. Lippincott Williams & Wilkins, 2001.
Signs and Symptoms
Blurry vision, aching.
Ocular Findings
 Lid, orbit granuloma, conjunctival nodules, lacrimal gland infiltration with dry eye.
Lid, orbit granuloma, conjunctival nodules, lacrimal gland infiltration with dry eye.
 Classic signs:
Classic signs:
Chronic granulomatous iridocyclitis.
Mutton fat keratic precipitates (Figure 4.6).
Koeppe/Busacca nodules (Figure 4.7).
Posterior synechiae.
 Posterior:
Posterior:
Granulomas (retinal or choroidal).
Candlewax drippings (granulomas along vessels).
Cystoid macular edema.
Peripheral neovascularization.
Optic nerve edema.
Optic nerve granulomas.
Snowbanks, snowballs.
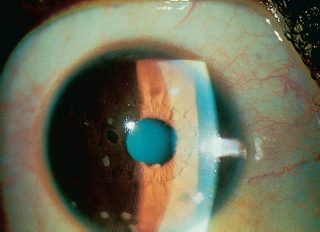
FIGURE 4.7. Koeppe nodules along the iris border at the 1, 4, and 8 o’clock positions. (From Tasman W, Jaeger E. The Wills Eye Hospital atlas of clinical ophthalmology, 2nd ed. Lippincott Williams & Wilkins, 2001.)
Systemic Findings
Hilar lymphadenopathy.
Erythema nodosum.
Skin granulomas.
Firm, painless lymphadenopathy.
Neurologic symptoms.
Special Tests
 Elevated angiotensin-converting enzyme (ACE) and/or lysozyme levels.
Elevated angiotensin-converting enzyme (ACE) and/or lysozyme levels.
 Chest radiograph (hilar adenopathy).
Chest radiograph (hilar adenopathy).
 Gallium scan (uptake in hilum, parotid gland, lacrimal gland).
Gallium scan (uptake in hilum, parotid gland, lacrimal gland).
 Biopsy of skin, conjunctival, lacrimal gland lesions.
Biopsy of skin, conjunctival, lacrimal gland lesions.
Treatment
Topical or periocular steroids.
Cycloplegia.
Immunosuppressives in refractory cases.
Pathology
Noncaseating epithelioid granulomas or tubercles.
Langhans giant cells, Schaumann or asteroid bodies.
References
Dana MR, Merayo-Lloves J, Schaumberg DA, et al. Prognosticators for visual outcome in sarcoid uveitis. Ophthalmology 1996;103:1846–1853.
Jabs DA, Johns CJ. Ocular involvement in chronic sarcoidosis. Am J Ophthalmol 1986;102:297–301.
Karma A, Huhti E, Poukkula A. Course and outcome of ocular sarcoidosis. Am J Ophthalmol 1988;106:467–472.
Power WJ, Neves RA, Rodriguez A, et al. The value of combined serum angiotensin-converting enzyme and gallium scan in diagnosing ocular sarcoidosis. Ophthalmology 1995;102:2007–2011.
Tuberculosis
Summary
Ocular inflammation attributed to Mycobacterium tuberculosis can present in many different forms and should be considered on every differential for uveitis.
Etiology
Infection attributable to M. tuberculosis or inflammatory reaction related to distant M. tuberculosis infection.
Epidemiology
 Approximately 1% to 2% of patients with TB develop ocular disease.
Approximately 1% to 2% of patients with TB develop ocular disease.
 Can affect any age; equal sex distribution.
Can affect any age; equal sex distribution.
 Any race, but more common in developing world.
Any race, but more common in developing world.
Ocular Findings
Can involve orbital adnexa, orbit, anterior and posterior segments.
Granulomatous or nongranulomatous uveitis.
Tubercle formation of eyelids and conjunctiva.
Corneal phlyctenule.
Conjunctivitis.
Scleritis.
Interstitial keratitis.
Anterior uveitis.
Vitritis.
Posterior uveitis.
Retinal vasculitis.
Choroidal granulomas.
Panuveitis.
Systemic Findings
 Can affect any organ system, lung most commonly affected.
Can affect any organ system, lung most commonly affected.
 Fever, fatigue, weight loss, and night sweats.
Fever, fatigue, weight loss, and night sweats.
Special Tests
 Tuberculin skin test (purified protein derivative [PPD]).
Tuberculin skin test (purified protein derivative [PPD]).
 Gamma interferon release assay (Quantiferon-Gold).
Gamma interferon release assay (Quantiferon-Gold).
 Chest x-ray: can be normal in 50% of patients with ocular TB.
Chest x-ray: can be normal in 50% of patients with ocular TB.
 Sputum cultures and smears for acid-fast bacilli.
Sputum cultures and smears for acid-fast bacilli.
 If possible, may culture or obtain pathologic examination of ocular specimen (nodules, granulomas).
If possible, may culture or obtain pathologic examination of ocular specimen (nodules, granulomas).
 Serum ACE and lysozyme levels may be elevated during active disease.
Serum ACE and lysozyme levels may be elevated during active disease.
 Human immunodeficiency virus (HIV) test: higher incidence in TB patients.
Human immunodeficiency virus (HIV) test: higher incidence in TB patients.
Pathology
 Caseating granulomatous inflammation consisting of fibroblasts lymphocytes.
Caseating granulomatous inflammation consisting of fibroblasts lymphocytes.
 Langhans giant cells, macrophages.
Langhans giant cells, macrophages.
Differential Diagnosis
 Sarcoidosis (increased ACE and lysozyme, anergic to PPD and other common antigens).
Sarcoidosis (increased ACE and lysozyme, anergic to PPD and other common antigens).
 Syphilis (rapid plasmin reagin [RPR], microhemagglutination-Treponema pallidium [MHA-TP]).
Syphilis (rapid plasmin reagin [RPR], microhemagglutination-Treponema pallidium [MHA-TP]).
 Consult infectious disease specialist.
Consult infectious disease specialist.
 Schlaegel test (of historical interest, no longer valid).
Schlaegel test (of historical interest, no longer valid).
 Multiple antituberculous drug therapy used to prevent formation of resistant strains:
Multiple antituberculous drug therapy used to prevent formation of resistant strains:
Isoniazid.
Rifampin.
Ethambutol.
Streptomycin.
Pyrazinamide.
 Topical and periocular steroids and cycloplegics are used for control of ocular inflammation.
Topical and periocular steroids and cycloplegics are used for control of ocular inflammation.
 Oral steroids contraindicated in patients with systemic TB without concomitant antituberculous therapy.
Oral steroids contraindicated in patients with systemic TB without concomitant antituberculous therapy.
Reference
Helm CJ, Holland GN. Ocular tuberculosis. Surv Ophthalmol 1993;38:229–256.
Syphilis
Summary
The ocular manifestations of syphilis are varied and protean. Almost every differential for uveitis contains syphilis.
Epidemiology
Acquired: young sexually active adults.
Etiology
Congenital: infection with spirochete Treponema pallidum.
Transmission
Congenital: transplacental.
Acquired: sexual.
Ocular Findings
 Congenital: salt-and-pepper retinopathy, chorioretinal scarring, cataract, glaucoma interstitial keratitis, optic atrophy.
Congenital: salt-and-pepper retinopathy, chorioretinal scarring, cataract, glaucoma interstitial keratitis, optic atrophy.
 Acquired:
Acquired:
Primary: usually none.
Secondary: acute, chronic, or recurrent granulomatous uveitis; scleritis; choroiditis; vitritis; papillitis; optic neuritis; vasculitis; keratitis linearis migrans (migrating deep stromal inflammation).
Tertiary: Argyll-Robertson pupils (light-near dissociation), iris gumma.
Systemic Findings
 Congenital: maculopapular rash, notched incisors (Hutchinson teeth), frontal bossing, saddle nose deformity.
Congenital: maculopapular rash, notched incisors (Hutchinson teeth), frontal bossing, saddle nose deformity.
 Acquired:
Acquired:
Primary: skin/mucus membrane lesions (painless chancre), lymphadenopathy.
Secondary: maculopapular rash, alopecia areata, fever, fatigue, sore throat, generalized lymphadenopathy.
Tertiary: gumma throughout body, aortic dilation, neurosyphilis (tabes dorsalis).
Diagnostic Tests
 RPR/Venereal Disease Research Laboratory (VDRL): nonspecific tests, reverts to negative result following treatment.
RPR/Venereal Disease Research Laboratory (VDRL): nonspecific tests, reverts to negative result following treatment.
 Fluorescent treponemal antibody, absorbed (FTA-Abs)/MHA-TP: specific for prior exposure to syphilis.
Fluorescent treponemal antibody, absorbed (FTA-Abs)/MHA-TP: specific for prior exposure to syphilis.
 Lumbar puncture VDRL and FTA-Abs: to look for neurosyphilis.
Lumbar puncture VDRL and FTA-Abs: to look for neurosyphilis.
 HIV testing: higher incidence of other concomitant sexually transmitted diseases (STDs).
HIV testing: higher incidence of other concomitant sexually transmitted diseases (STDs).
Treatment
 Consult with infectious disease specialist for antibiotic guidelines (usually penicillin for 10 to 14 days).
Consult with infectious disease specialist for antibiotic guidelines (usually penicillin for 10 to 14 days).
 Acute IK: topical steroids.
Acute IK: topical steroids.
 Corneal transplantation may be required for corneal scarring related to IK.
Corneal transplantation may be required for corneal scarring related to IK.
 Uveitis associated with syphilis: topical, periocular, and systemic steroids following adequate antibiotic prescription.
Uveitis associated with syphilis: topical, periocular, and systemic steroids following adequate antibiotic prescription.
Reference
Margo CE, Hamed LM. Ocular syphilis. Surv Ophthalmol 1992; 37:203–220.
Pars Planitis
Summary
At some centers, the terms pars planitis and intermediate uveitis are used interchangeably; however, in this context, pars planitis refers to intermediate uveitis of unknown etiology.
Epidemiology
Most commonly in second to fourth decades of life; 80% of cases are bilateral.
Signs and Symptoms
Blurry vision, floaters.
Ophthalmic Findings
Cystoid macular edema (CME, predominant cause of decreased vision).
Low-grade anterior chamber reaction.
Posterior synechiae (rare).
Posterior subcapsular cataract.
Subretinal and preretinal neovascular membranes.
Vitreous hemorrhage.
Retinal phlebitis.
Snowballs: cellular aggregates in vitreous.
Snowbank: fibrovascular exudative changes of the inferior pars plana.
Etiology
Unknown; possible association with the HLA-DR locus.
Disease Course
 Seventy-five percent have benign or mild chronic disease.
Seventy-five percent have benign or mild chronic disease.
 Twenty-five percent have severe chronic or relentlessly progressive inflammation leading to cyclitic membranes, RD, and phthisis.
Twenty-five percent have severe chronic or relentlessly progressive inflammation leading to cyclitic membranes, RD, and phthisis.
Treatment
Stepladder treatment approach strongly recommended if CME or vasculitis present, regardless of visual acuity.
Smoking cessation; smoking correlates with vision loss.
Periocular steroid injections with topical steroids for anterior segment inflammation.
Oral nonsteroidal anti-inflammatory drugs (NSAIDs) for recurrent inflammation.
Systemic steroids for persistent or recurrent inflammation.
Cryotherapy or peripheral laser photocoagulation.
Immunosuppression (cyclosporine, azathioprine, methotrexate) if patient fails therapy or becomes intolerant to steroids.
Pars plana vitrectomy if refractory.
References
Brockhurst R, Schepens C. Uveitis IV. Peripheral uveitis: the complications of retinal detachment. Arch Ophthalmol 1968;80:747–753.
Donaldson MJ, Pulido JS, Herman DC, et al. Pars planitis: a 20-year study of incidence, clinical features, and outcomes. Am J Ophthalmol 2007;144:812–817.
Kaplan HJ. In: Saari KM, ed. Uveitis update. Amsterdam, The Netherlands: Excerpta Medical, 1984:169–172.
Malinowski SM, Pulido JS, Goeken NE, et al. The association of HLA-B8, B51, DR2, and multiple sclerosis in pars planitis. Ophthalmology 1993;100:1199–1205.
Lyme Disease
Summary
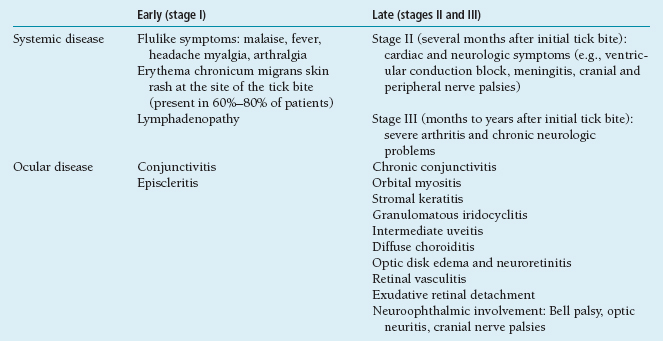
Lyme disease is a multisystem disorder caused by the spirochete Borrelia burgdorferi with ophthalmic, dermatologic, rheumatologic, neurologic, and cardiac manifestations (see Table 4.4).
Table 4.4 Stages of Lyme disease
Infection by the spirochete B. burgdorferi transmitted by Ixodes deer ticks.
Epidemiology
 Residents of tick-endemic areas: eastern coastal states, northern California, and the northern Midwest.
Residents of tick-endemic areas: eastern coastal states, northern California, and the northern Midwest.
 History of hiking, camping.
History of hiking, camping.
Special Tests
Serologic testing (ELISA most sensitive, Western blot for confirmation) for IgM and IgG against B. burgdorferi.
In endemic areas, baseline positive serology may be present in up to 15% of patients. Positive serology plus erythema chronicum migrans or one organ system involvement is diagnostic.
In nonendemic areas, involvement of two or more organ systems is needed for the diagnosis.
Serology will cross-react with other spirochetes such as T. pallidum.
Lumbar puncture: CSF pleocytosis.
Disease Course
Frequent recurrences.
Differential Diagnosis
Sarcoidosis, syphilis, and TB.
Treatment
Early (stage I):
1. Doxycycline.
2. Amoxicillin.
3. Erythromycin.
Late (stages II and III):
1. Ceftriaxone.
2. Penicillin G.
3. Doxycycline (may be less effective).
References
Copeland RA Jr. Lyme uveitis. Int Ophthalmol Clin 1990;30: 291–293.
Winward KE, Smith JL, Culbertson WW, et al. Ocular Lyme borreliosis. Am J Ophthalmol 1989;108:651–657.
Zaidman GW. The ocular manifestations of Lyme disease. Int Ophthalmol Clin 1997;37:13–28.
Summary
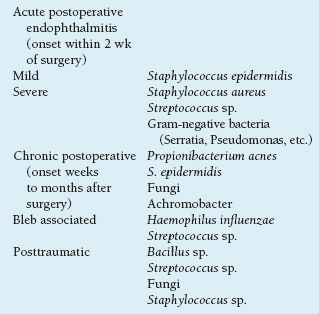
Endophthalmitis describes infectious intraocular inflammation (anterior chamber and vitreous) (Table 4.5).
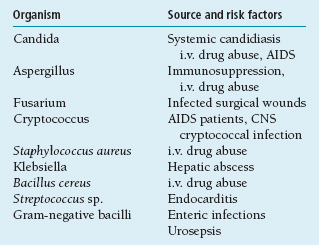
Table 4.5 Organisms most often responsible for exogenous endophthalmitis
Acute Postoperative Endophthalmitis
Summary
Intraocular inflammation within days following ocular surgery is a rare complication usually secondary to bacterial infection.
Etiology
Organisms from the periocular field gaining entry into the eye, usually through wound.
Signs and Symptoms
Decreased vision.
Pain, photophobia.
Redness.
Demographics
Incidence less than 0.1% in large series of cataract extractions.
Ophthalmic Findings
Severe: rapid, fulminant course, 3 to 7 days after surgery.
Mild: slow, indolent course; onset within 2 weeks of surgery.
Anterior chamber and vitreous inflammation.
Hypopyon.
Decreased visual acuity.
Systemic Findings
None.
Anterior chamber and vitreous tap to determine causative organism.
Treatment and Management
Vitrectomy.
Intravitreal antibiotics.
Corticosteroids.
Fortified topical antibiotics.
References
Endophthalmitis Vitrectomy Study Group. Microbiologic factors and visual outcome in the endophthalmitis vitrectomy study: the Endophthalmitis Vitrectomy Study. Am J Ophthalmol 1996; 122:830–846.
Endophthalmitis Vitrectomy Study Group. Results of the Endophthalmitis Vitrectomy Study: a randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Arch Ophthalmol 1995;113:1479–1496.
Chronic Postoperative Endophthalmitis
Summary
Chronic postoperative endophthalmitis is an indolent inflammatory condition caused by less virulent organisms such as P. acnes and fungi.
Etiology
Low-grade infection caused by organisms such as P. acnes, fungi, Staphylococcuse pidermidis, and Achromobacter.
Signs and Symptoms
Decreased vision.
Mild pain or photophobia.
Ophthalmic Findings
Low-grade anterior chamber or diffuse inflammation.
Keratic precipitates.
Waxing and waning course.
Capsular plaque or retained lens material.
Systemic Findings
None.
Special Tests
Vitreous tap and anaerobic cultures.
Capsular biopsy.
Pathology
Propionibacterium acnes: Gram-positive rods sequestered in capsular bag and in lens fragments.
Disease Course
 Fluctuating, low-grade iridocyclitis.
Fluctuating, low-grade iridocyclitis.
 May initially respond to topical corticosteroids.
May initially respond to topical corticosteroids.
Treatment and Management
Capsulectomy.
Removal of retained lens material.
Intravitreal antibiotics.
Cure rate is 7% with intravitreal antibiotics, 50% with intravitreal antibiotics + vitrectomy, 75% with intravitreal antibiotics + vitrectomy + partial capsulectomy, 100% with intravitreal antibiotics + vitrectomy + IOL removal and total capsulectomy.
Differential Diagnosis
Phacoantigenic uveitis.
UGH syndrome.
Reference
Mandelbaum S, Meisler DM. Postoperative chronic microbial endophthalmitis. Int Ophthalmol Clin 1993;33:71–79.
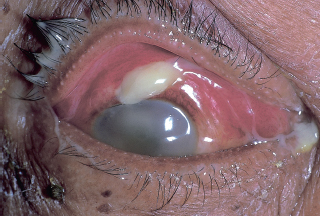
Bleb-Associated Endophthalmitis
Summary
Thin avascular glaucoma-filtering blebs may predispose patients to an increased risk of endophthalmitis. The most common organisms isolated are Streptococcus species and Haemophilus influenzae.
Etiology
 Hole in bleb → infection → endophthalmitis.
Hole in bleb → infection → endophthalmitis.
 Thin avascular blebs (such as after the use of antimetabolites) may be at higher risk.
Thin avascular blebs (such as after the use of antimetabolites) may be at higher risk.
 Inferior blebs are also at higher risk for infection.
Inferior blebs are also at higher risk for infection.
Signs and Symptoms
Redness, tearing, and discharge.
Decreased vision.
Pain.
Demographics
Glaucoma patients following trabeculectomy; incidence varies from 1% to 18%.
Ophthalmic Findings
Infiltrated bleb filled with purulent material (Figure 4.8).
Hypopyon.
Anterior chamber and vitreous inflammation.
Hypotony.
Systemic Findings
None.
Special Tests
 Anterior chamber and vitreous tap to identify organism.
Anterior chamber and vitreous tap to identify organism.
 H. influenzae and Streptococcus pneumoniae most commonly isolated.
H. influenzae and Streptococcus pneumoniae most commonly isolated.
Treatment and Management
Topical and subconjunctival antibiotics may be sufficient for localized bleb infection.
If endophthalmitis is present, treat with intravitreal antibiotics; obtain vitreous aspirate.
Repair of bleb leak.
Posttraumatic Endophthalmitis
Summary
Posttraumatic endophthalmitis is a potentially severe intraocular infection following a penetrating ocular injury.
Etiology
Penetrating ocular trauma with or without a retained intraocular foreign body allowing access of bacteria into the eye.
Signs and Symptoms
Pain.
Redness.
Decreased vision.
Demographics
Incidence up to 30% following penetrating ocular injury.
Ophthalmic Findings
Hypopyon.
Hyphema.
Vitreous hemorrhage.
Severe intraocular inflammation.
Retained intraocular foreign bodies.
Incarceration of uvea or vitreous in wound.
Leaking or gaping wound.
Systemic Findings
None.
Special Tests
 Anterior chamber and vitreous taps to determine organism responsible for infection.
Anterior chamber and vitreous taps to determine organism responsible for infection.
 Ultrasound, computed tomography (CT), or x-ray imaging to rule out foreign bodies.
Ultrasound, computed tomography (CT), or x-ray imaging to rule out foreign bodies.
Disease Course
 Bacillus cereus infection: rapidly progressive infection. Often results in extensive ocular damage and poor acuity (Figure 4.9).
Bacillus cereus infection: rapidly progressive infection. Often results in extensive ocular damage and poor acuity (Figure 4.9).
 Fungi: suspect in trauma with organic material (e.g., wood, straw).
Fungi: suspect in trauma with organic material (e.g., wood, straw).
Treatment and Management
Broad spectrum antibiotics (topical, subconjunctival, intravitreal, and i.v.).
Antifungals.
Steroids.
Vitrectomy.
Endogenous Endophthalmitis
Summary
Endogenous endophthalmitis is caused by intraocular spread of blood-borne organisms and requires systemic therapy.
Etiology
Disseminated systemic microbial infection spread to the eye.
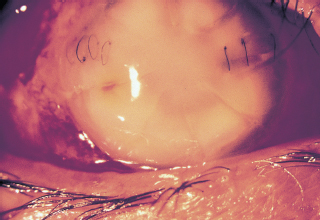
FIGURE 4.9. Severe intraocular infection caused by Bacillus cereus following a penetrating fish-hook injury in a patient with previous radial keratotomy.
Blurred vision.
Demographics
Immunosuppressed patients.
Intravenous drug abusers.
Intravenous and indwelling lines.
Chronic tissue infections (e.g., osteomyelitis).
Ophthalmic Findings
Elevated choroidal mass.
Vitritis.
Retinitis.
Systemic Findings
Infected i.v. lines.
Abscesses.
Disseminated fungal infection.
Signs of systemic infection.
Special Tests
Vitreous biopsy.
Blood cultures.
Urine cultures.
Treatment and Management
Vitrectomy.
Systemic antimicrobial treatment.
Differential Diagnosis
Intraocular lymphoma.
See Table 4.6.
Endophthalmitis Vitrectomy Study
Study Population
Patients with endophthalmitis after cataract surgery.
Entry Criteria
 Endophthalmitis within 6 weeks of cataract surgery or secondary IOL placement (acute postoperative endophthalmitis).
Endophthalmitis within 6 weeks of cataract surgery or secondary IOL placement (acute postoperative endophthalmitis).
 Acuity between 20/50 and LP.
Acuity between 20/50 and LP.
Study Design
 Multicenter randomized clinical trial.
Multicenter randomized clinical trial.
 Four subgroups:
Four subgroups:
1. Initial vitrectomy and i.v. antibiotics.
2. Initial vitrectomy without i.v. antibiotics.
3. Initial vitreous tap and i.v. antibiotics.
4. Initial vitreous tap without i.v. antibiotics.
 All patients received intravitreal antibiotics.
All patients received intravitreal antibiotics.
Table 4.6 Organisms responsible for endogenous endophthalmitis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


