Filtering Surgery
The incisional operation most frequently used for chronic forms of glaucoma, especially in adults, is commonly referred to as a filtering procedure. Although several variations for this surgical procedure have been described, all filtering operations share the same basic mechanism of action and general surgical principles. We first consider these aspects and then discuss specific filtration techniques and potential complications.
Mechanisms of Action
Drainage Fistula
The basic mechanism of all filtering procedures is the creation of an opening, or fistula, at the limbus, which allows a direct communication between the anterior chamber and subconjunctival space. This fistula bypasses the trabecular meshwork, Schlemm canal, and collecting channels. From the subconjunctival spaces, aqueous is absorbed by surrounding tissues or crosses the conjunctival epithelium and drains with tears through the nasolacrimal duct.
Filtering Bleb
Most, but not all, successful glaucoma filtering procedures are characterized by an elevation of the conjunctiva at the surgical site, which is commonly referred to as a filtering bleb. The clinical appearance and function of these blebs vary considerably with regard to extent, elevation, and vascularity (1,2). The blebs that are most often associated with good intraocular pressure (IOP) control have decreased vascularity with numerous microcysts in the epithelium and are either low and diffuse or more circumscribed and elevated (3) (Fig. 38.1).
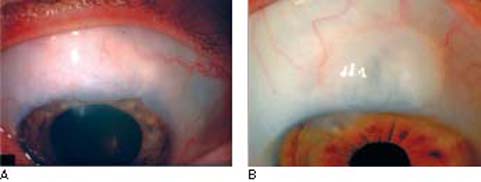
Figure 38.1 Types of functioning filtering blebs. A: Low, diffuse bleb. B: Discrete, elevated bleb. Note that both are avascular.
The histologic appearance of both functioning and failed filtering blebs consists of normal epithelium with no encircling-type junctions between the cells that would limit fluid flow (3). The subepithelial connective tissue may contain viable activated fibrocytes (4), and the histologic appearance at this level correlates better with bleb status than does that of the epithelium, in that functioning blebs have loosely arranged tissue with histologically clear spaces, whereas the failed blebs have dense collagenous connective tissue (3). Change in morphology and a decrease in the number of epithelial and goblet cells have been found in conjunctival epithelium overlying thin cystic blebs (5).
Routes of Aqueous Drainage
Studies have suggested that aqueous in the filtering bleb usually filters through the conjunctiva and mixes with the tear film or is absorbed by vascular or perivascular conjunctival tissue (6–10). Less commonly, a filtering procedure may be associated with IOP control in the absence of an apparent filtering bleb. This is more common when the fistula is covered by a partial-thickness scleral flap (trabeculectomy), and suggested mechanisms of aqueous drainage in these cases include flow through (a) lymphatic vessels near the scarred margins of the surgical area; (b) atypical, newly incorporated aqueous veins; and (c) normal aqueous veins (6,10). Preservation of the aqueous drainage route beneath the scleral flap, as seen on ultrasound biomicroscopy, appears to correlate with the development of a filtering bleb following trabeculectomy (11,12).
Basic Techniques of Filtering Surgery
The various types of filtering surgery differ primarily according to the method used to create the drainage fistula. The other aspects of the operation are basically the same for all filtering procedures and are discussed first before specific fistulizing techniques are considered.
Traction Sutures
Good surgical exposure is critical to the successful outcome of a filtering procedure. In most cases, this requires the use of a traction suture. The two most common techniques are (a) a superior rectus traction suture (Fig. 38.2) and (b) a clear cornea traction suture (Fig. 38.3). With the former technique, the globe is rotated down, and the superior rectus muscle is grasped with forceps, through conjunctiva, 10 to 15 mm behind the limbus. A 4-0 silk suture is then passed through conjunctiva and around the muscle beneath the tips of the forceps, and the suture is attached to the head of the surgical drape. With the clear cornea technique, a 7-0 polyglactin or silk suture is passed to a corneal depth of approximately three-fourths thickness, 1 mm from the limbus with a bite width of 4 to 5 mm, and is then attached to the drape over the cheek. The rectus suture has the potential disadvantages of a subconjunctival hemorrhage or a hole in the conjunctiva that may leak postoperatively. The corneal suture is preferred by most surgeons but may distort the cornea and anterior chamber during the surgery. Additional Tenon traction sutures have been suggested to help in visualization and surgical access during filtering procedures (13).
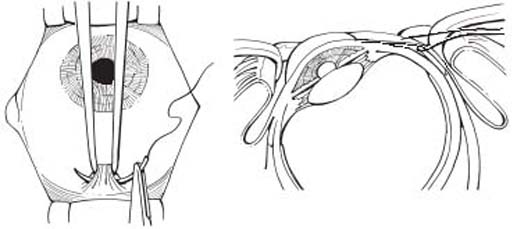
Figure 38.2 Bridle suture.
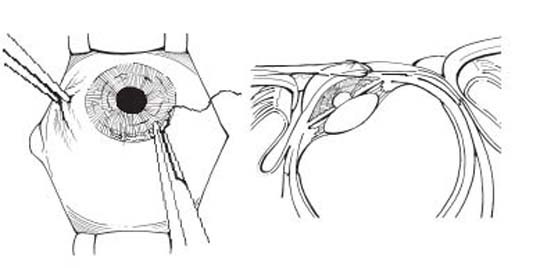
Figure 38.3 Corneal traction suture.
Limbal Stab Incision (Paracentesis Site)
Some surgeons create a paracentesis, which consists of a self-sealing, beveled incision into the anterior chamber at the limbus, usually temporally at the horizontal meridian, or in the inferior-temporal quadrant, as a route for injecting fluid at the end of the procedure. This can be done with a tapered, pointed knife, or number 75 blade before entering anterior chamber under the scleral flap. If antifibrosis agents (discussed later in this chapter) are to be used, however, it may be best to wait until after that step of the operation, to avoid a route for potential entry of the drug into the anterior chamber.
Preparation of the Conjunctival Flap
Preparation of the conjunctival flap is a critical step in all filtering procedures, in that the most common cause of failure is scarring of the filtering bleb. Although techniques differ among surgeons, meticulous detail with minimal tissue damage and bleeding is essential.
Position of the Flap
Some surgeons elect to make the flap at the 12-o’clock position to take advantage of the wider limbus in this area. Others prefer one of the superior quadrants, leaving the adjacent quadrant available for future surgery if required. The inferior quadrant was used in the past when previous ocular surgery resulted in scarring of conjunctiva in the superior quadrants (14). However, the latter technique is associated with an increased risk for endophthalmitis and should be avoided (15).
Limbus-Based versus Fornix-Based Flap
Conjunctival flaps for glaucoma filtering surgery have traditionally been limbus based—that is, with the initial incision in the fornix (Fig. 38.4). More recently, a fornix-based flap has gained favor (Fig. 38.5), particularly in association with a trabeculectomy (16–18). Several studies have compared limbus- and fornix-based conjunctival flaps in association with trabeculectomy and reported similar success rates, whether used in combination with cataract surgery or as a separate procedure (19–28). However, one investigative team found slightly better postoperative IOP control with the limbus-based flap (29), whereas others found better pressure control and more diffuse blebs with the fornix-based flaps (17,30). One retrospective study found cystic leaking blebs only in eyes with limbus-based flaps (24).
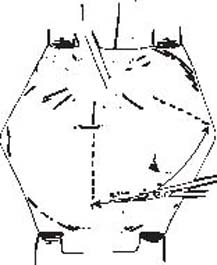
Figure 38.4 Incision through conjunctiva in preparation of a limbus-based conjunctival flap.
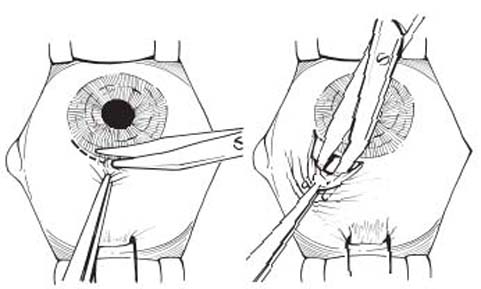
Figure 38.5 Incision through conjunctiva in preparation of a fornix-based conjunctival flap.
Surgeons differ on this aspect of filtering surgery, with some preferring the relative ease and improved surgical exposure of the fornix-based flap and others preferring the tighter wound closure that may be achieved with the limbus-based flaps. One circumstance in which a fornix-based conjunctival flap is especially useful is when such a flap was used previously, as during an extracapsular cataract or scleral buckling surgery, leaving a band of scar tissue at the limbus. In these cases, it is difficult to dissect a limbus-based flap sufficiently anteriorly without creating holes in the conjunctiva. A preferable alternative is to excise the band of scar tissue and pull the new edge of the conjunctival flap down to peripheral cornea.
Management of Tenon Capsule
There is some controversy regarding the value of removing all or a portion of Tenon capsule, the main source of fibroblasts in the area of the conjunctival flap. Two studies revealed no difference in postoperative IOP control between eyes with excision of the capsular tissue and those in which it was left partially or totally intact (31,32). For this reason, many surgeons routinely preserve Tenon capsule by dissecting between the capsule and episclera when preparing the conjunctival flap. This may be especially important when using adjunctive antifibrosis agents, to avoid excessively thin or leaking filtering blebs in the late postoperative course. Sub-Tenon space also appears to be the best cleavage plane for aqueous drainage because there is less scarring and subsequently less resistance to flow (33). Modified fornix-based techniques have been described, such as small incision trabeculectomy and microtrabeculectomy (34–36), by using 2.5- to 3-mm conjunctival peritomy within 2 mm of the limbal area and avoiding Tenon capsule. Other surgeons excise variable amounts of Tenon capsule when it appears to be unusually thick, as in young patients. This can be accomplished by dissecting between the conjunctiva and Tenon capsule and then excising the capsule from the episclera. An alternative approach is to dissect Tenon capsule from underlying episclera, strip a portion of the capsule from the conjunctiva with gentle traction, and then excise the exposed portion of capsular tissue.
With all techniques, blunt dissection is used when possible to avoid bleeding, and sharp dissection is used only when required. Gentle handling of the conjunctiva is essential at all times, and nontoothed conjunctival forceps are preferable to avoid tearing or crushing the conjunctiva. During the fistulizing part of the operation, it is important to keep the conjunctival flap moist and to minimize handling of the tissue. With a limbus-based flap, this can be conveniently accomplished by reflecting the flap over the cornea with a surgical sponge (Fig. 38.6) or nontoothed forceps. When manipulating the conjunctiva–Tenon capsule flap, it is best to grasp the capsule and avoid touching the conjunctiva.
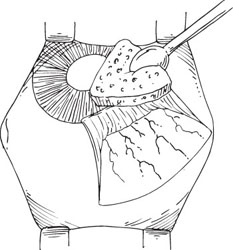
Figure 38.6 Retraction of conjunctival flap over the cornea.
Use of Viscoelastic Agents
The injection of a viscoelastic agent (e.g., sodium hyaluronate) into the anterior chamber at the completion of the filtering procedure did not reduce the incidence of postoperative flat anterior chambers in most studies (37–39). However, injecting the agent through a paracentesis incision at the outset of a trabeculectomy procedure was associated with a lower incidence of this complication (40,41), presumably by avoiding intraoperative hypotony and the subsequent suprachoroidal effusion that may initiate the cascade of events leading to a shallow anterior chamber. Others have supported this finding and noted that the technique also tends to minimize intraoperative bleeding (42) but not postoperative hyphema or postoperative corneal endothelial cell loss (43,44). Complications of intracameral viscoelastics include iris prolapse during surgery and a higher early postoperative IOP, for which the preoperative use of pilocarpine, 2%, and a slightly less tight closure of the scleral flap were recommended (41,44). Injection of dense viscoelastics, such as Healon or Healon 5, into the anterior chamber may be used as a temporary solution for postoperative flat anterior chambers (45–47).
Peripheral Iridectomy
A peripheral iridectomy is a routine part of all standard filtering procedures and is usually made after the fistula has been prepared (48). However, if the iris prolapses into the limbal wound, it is generally best to make the iridectomy and then complete the fistula. The iridectomy should extend beyond the margins of sclerectomy to avoid obstruction of the fistula by the peripheral iris. The technique for the incisional peripheral iridectomy is discussed in Chapter 36.
Complications of the surgical iridectomy itself can include inflammation, hyphema, and iridodialysis. It is preferable not to make the iris incision too close to the iris root for concern of incising the ciliary body and inducing significant bleeding. Some surgeons omit the peripheral iridectomy in patients who have pseudophakia or undergo a combined trabeculectomy with cataract surgery using a small-clear corneal incision. This is especially true in cases where there is a deep anterior chamber and the risk of iris incarceration into the sclerectomy is low. In one study, patients with and without peripheral iridectomy had similar postoperative vision and IOP control (49,50).
Closure of the Conjunctival Flap
Watertight closure of the conjunctival flap is also a critical aspect of any filtering procedure, because a leaking wound may lead to a persistently flat bleb or anterior chamber, or both. This can lead to failure of the filtering bleb to develop properly. A fine absorbable suture, such as 10-0 polyglycolic acid or polyglactin, on a tapered, vascular needle is desirable, because it minimizes leakage at the suture sites and excessive tissue reaction. For closure of a limbus-based flap, a running suture with close bites provides the tightest closure. When Tenon capsule has been preserved, a double running closure, first of Tenon tissue, and then conjunctiva, may increase the chances of tight wound closure (Fig. 38.7) (51). Alternatively, several interrupted sutures that close Tenon capsule may be used to approximate the wound edges before running closure. This is especially important when adjunctive antifibrosis agents are used.
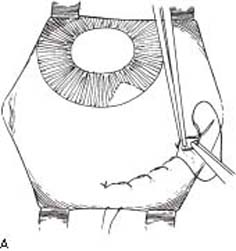
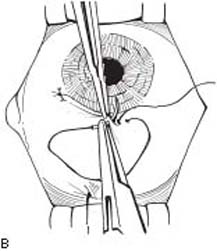
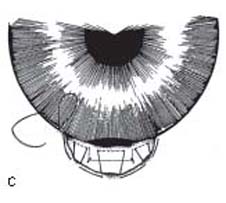
Figure 38.7 A: Closure of conjunctival flap with running suture. B: Closure of fornix-based conjunctival flap. C: Closure of fornix-based conjunctival flap—Wise closure. (From Shields MB. Trabeculectomy vs. full-thickness filtering operation for control of glaucoma. Ophthalmic Surg. 1980;11:498, with permission.) (From Ng PW, Yeung BY, Yick DW, et al. Fornixbased trabeculectomy with Wise’s suture technique in Chinese patients. Ophthalmology. 2000;107:2310–2313, with permission.)
A running suture can also be placed along the limbus for fornix-based flaps, especially when a small edge of conjunctiva is retained adjacent to the limbus (52). Various techniques have been described for placing a running mattress suture at the limbus, which provides tight wound closure and is especially useful when adjunctive antifibrosis agents are used (52–54). In other situations, surgeons find it adequate to use a single interrupted suture at one or both ends of the conjunctival flap (18,55) (Fig. 38.7), which stretches the conjunctiva tightly over peripheral cornea.
If a paracentesis is made at the outset, balanced salt solution, or a viscoelastic, by using a cannula on a syringe, may be injected into the anterior chamber via that incision at two stages during the completion of the procedure. The first of these is after suturing the scleral flap in a trabeculectomy to ensure appropriate flow around the flap. The anterior chamber should deepen and the eye should become slightly firm before fluid begins to flow around the flap edges. If the flow is too brisk and the chamber collapses, more sutures should be added. Conversely, sutures may need to be loosened if the eye remains too firm. The second stage of fluid injection is after closure of the conjunctival flap. This should deepen the anterior chamber and create a sustained elevation of the bleb, thereby demonstrating patency of the fistula and watertight closure of the conjunctival incision. Some surgeons examine the conjunctival closure for bleb leaks by coating the bleb surface with fluorescein at the end of the case.
Postoperative Management
Topical mydriatic–cycloplegics may be used for the first 2 to 3 weeks to help maintain the anterior chamber depth, particularly in patients with phakic eyes and those with postoperative hypotony. Some investigators feel that these agents may also reduce postoperative inflammation (56). Topical antibiotics are used routinely for 7 to 10 days. Use of topical corticosteroids decreases conjunctival scarring and is associated with higher success rates with trabeculectomy. They are typically used for 4 to 6 weeks, although some surgeons use low-dose topical corticosteroids indefinitely. (The effect of postoperative corticosteroid use is discussed in more detail later in the chapter.)
Fistulizing Techniques
There are two basic types of fistulas: (a) those which extend through the full thickness of the limbal tissue and (b) those which are covered by a partial-thickness scleral flap. During the first half of the 20th century, the former technique was used exclusively. The concept of a guarded fistula (trabeculectomy) began to gain popularity in the 1970s. With the advent of adjunctive antifibrosis agents and laser suture lysis, the full-thickness procedures lost favor compared with conventional trabeculectomy surgery and are now primarily of historical interest.
Partial-Thickness Fistulas (Trabeculectomy)
The standard full-thickness filtering procedures were often complicated by excessive aqueous filtration, which led to a high incidence of prolonged flat anterior chambers, associated with corneal decompensation, synechiae formation, and cataracts. In addition, the filtering blebs often became thin and were susceptible to rupture, creating the danger of endophthalmitis. One way to minimize these complications is to place a partial-thickness scleral flap over the fistula. This concept was suggested by Sugar (57) in 1961 but was popularized by the 1968 report of Cairns (58). Both authors referred to the technique as a trabeculectomy, and this remains the most commonly used technique for filtering surgery today.
Theories of Mechanism
It was originally thought that aqueous might flow into the cut ends of Schlemm canal (58). Subsequent studies, however, showed fibrotic closure of the canal at its cut ends in monkey and human (59,60) eyes, and the presence of Schlemm canal in the “trabeculectomy” specimen did not correlate with the outcome of the procedure (61–63). Furthermore, it was noted that most successful cases had a filtering bleb, and the amount of fluorescein-stained aqueous in the filtration area correlated with the success of the procedure (64), suggesting that external filtration was the principal mode of IOP reduction. The outer layers of limbus and anterior sclera do not differ ultrastructurally from the inner layers in a way that might predispose to increased passage of aqueous (65). Perfusion studies of human autopsy eyes, in which a trabeculectomy was created and the margins of the scleral flap were sealed with adhesive, did show a significant flow through the scleral flap (66). Fluorescein angiographic studies of eyes with successful trabeculectomies showed the primary route of external filtration to be around the margins of the scleral flap (67). It may be that external filtration occurs around or through the scleral flap, depending on how tightly the flap is sutured or the thickness of the scleral flap. Use of antimetabolites often leads to alterations of the scleral flap ranging from a complete melt to a minimal decrease of integrity. Other contributors to the outflow resistance are the surface area of the bleb available for diffusion and the quality of the conjunctiva overlying the bleb (i.e., thin and avascular, or thicker with only decreased vascularity) (Fig. 38.8). Other possible mechanisms of IOP reduction by trabeculectomy include cyclodialysis, if the fistula extends posterior to scleral spur (59), or aqueous outflow through newly developed aqueous veins, lymphatic vessels, or normal aqueous veins (68,69).
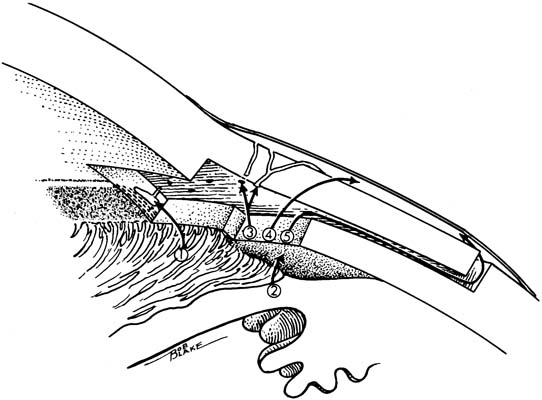
Figure 38.8 Possible routes of aqueous humor flow associated with a trabeculectomy: 1, Aqueous flow into cut ends of Schlemm canal (rare); 2, cyclodialysis (if tissue is dissected posterior to scleral spur); 3, filtration through outlet channels in scleral flap; 4, filtration through connective tissue substance of scleral flap; 5, filtration around the margins of the scleral flap.
Basic Trabeculectomy Technique
With the trabeculectomy technique (Fig. 38.9), the margins of the scleral flap, adjacent to the corneolimbal junction, are outlined first with light cautery and then with partial-thickness scleral incisions. The original technique described by Cairns involved a 5 × 5-mm square, but numerous variations in size and shape of the scleral flap have been described, as discussed later in this section. A lamellar flap, hinged at the limbus, is then dissected forward until at least 1 mm of the bluish-gray zone of the peripheral cornea is exposed. It is difficult to precisely determine the relative thickness of the scleral flap, but in general, it should be one-half to two-thirds sclera thickness.
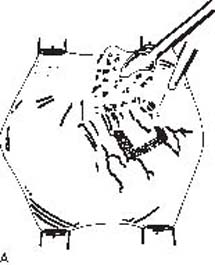
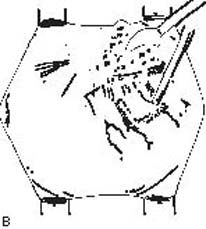
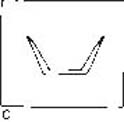

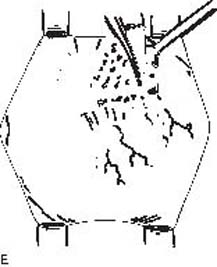
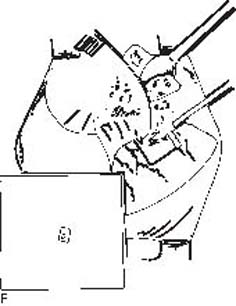
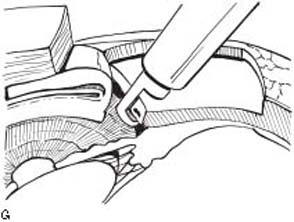
Figure 38.9 Selected steps in performing trabeculectomy. A: Cauterization of area intended for margins of scleral flap. B: Margins of scleral flap outlined by partial-thickness incisions. C: Triangular scleral flap as an alternative technique. D: Anterior chamber entered just behind the hinge of the scleral flap. E: Completion of anterior and lateral margins of deep limbal incision with scissors. F,G: Flap of deep limbal tissue excised using Kelly punch. (Portions modified from Shields MB. Trabeculectomy vs. full-thickness filtering operation for control of glaucoma. Ophthalmic Surg. 1980;11:498, with permission.)
The fistula is begun by first entering the anterior chamber with a knife just behind the hinge of the scleral flap, and then widening the incision with the knife or scissors to within approximately 0.5 mm of the scleral flap margins. Radial incisions are then extended posteriorly on either end of the initial incision for 1 mm, and the resulting flap of deep limbal tissue is reflected until the angle structures can be visualized, and the tissue is excised with scissors along the scleral spur. Today most surgeons prefer using a scleral punch (described later).
After making a peripheral iridectomy, the scleral flap is approximated with 10-0 nylon sutures. Some surgeons prefer to approximate the scleral flap loosely with two sutures at the posterior corners to promote filtration around the margins of the flap. Others prefer tighter closure at the posterior corners and sometimes use additional sutures to avoid the complications of hypotony and a flat anterior chamber. However, loose and tight closures did not differ significantly within 3 months postoperatively in one study (70). Closure that achieves mild-to-moderate resistance to aqueous flow, thus maintaining anterior chamber depth, is optimal. It is especially important when using adjunctive antifibrosis agents, because these eyes are much more susceptible to excessive filtration and hypotony. Most surgeons prefer to achieve tighter scleral wound closure, with the plan to lyse sutures postoperatively with an argon or diode laser, if necessary, using specially designed lenses (71–74). An alternative to laser suture lysis is the use of releasable sutures, which can be removed, as required, at the slitlamp. Several effective techniques for releasable sutures have been described (75–78). As noted earlier, the scleral flap can be tested for adequate flow resistance before closing the conjunctival flap by injecting balanced salt solution into the anterior chamber via a paracentesis.
Modifications in Technique
The numerous variations of the guarded filtering procedure that have been reported primarily involve modifications in the scleral flap or in the fistulizing technique.
Variations in the Scleral Flap
Rather than making a square flap, some surgeons prefer a triangular (79), semicircular (80), or trapezoid shape. There is no apparent advantage of one shape over another with regard to long-term success. Some surgeons attempt to influence the degree of postoperative filtration by modifying the scleral flap. It has been suggested, for example, that the thickness of the flap correlates with the final IOP, in that thinner flaps provide greater filtration and lower pressures (81). Other variations in surgical technique have included attempts to enhance filtration around the flap by applying light cautery to the lateral margins (67), omitting all sutures for the scleral flap (82), or excising the distal 2 mm of the flap (82). These techniques predate the era of antifibrosis agents, however, and should be avoided when such adjunctive therapy is used. Placement of amniotic membrane under the scleral flap and suturing it with 10-0 nylon has been suggested for prevention of postoperative adhesion of conjunctiva and sclera in patients with whom the risk for failure is high (83). Another variation in creating the scleral flap involves the scleral tunnel technique, as has been used with phacoemulsification (84). The sides of the tunnel are then incised with scissors to create the flap.
Variations in the Fistulizing Technique
Watson (85,86) modified Cairns’s basic technique by starting the dissection of the tissue block posteriorly over ciliary body, separating it from the underlying structure, and excising it at Schwalbe line. Other techniques to create the fistula beneath a scleral flap include trephinations, sclerectomies, thermal sclerostomies, and sclerostomies with a carbon dioxide laser (80,87–91). Most surgeons use a Kelly Descemet membrane punch or Crozafon–De Laage punch to excise limbal tissue sections from the posterior lip of the initial incision beneath the scleral flap (92,93).
Modifications for Neovascular Glaucoma
As discussed in Chapter 19, intraocular surgery in eyes with neovascular glaucoma is often complicated by intraoperative hyphema. One trabeculectomy variation to minimize this risk includes excision of a large trabecular segment, partial nonpenetrating cyclodiathermy in the scleral bed, and partial ablation of abnormal iris vessels with a wide sector iridectomy (94). Glaucoma drainage-device surgery and diode laser cyclophotocoagulation are increasingly considered to be the treatments of choice for this disorder (95), and they are discussed in other chapters.
The optimum approach to filtering surgery in eyes with neovascular glaucoma, however, is to precede it with an intravitreal injection of anti–vascular endothelial growth factor (anti-VEGF) agent or panretinal photocoagulation, when possible, which often reduces neovascularization, decreasing the likelihood or degree of postoperative hyphema regardless of the surgical treatment used.
Trabeculectomy for neovascular glaucoma often fails because of scarring of the filtering bleb; therefore, the use of mitomycin C (MMC) and 5-fluorouracil (5-FU) has been advocated in those eyes. One study classified two thirds of eyes after panretinal photocoagulation followed by trabeculectomy with MMC as surgical success after 2 years of follow-up (96). Another study did not find that differences in the MMC concentration or application time affected postoperative IOP or complication rates (97). The number of successful surgeries was 71% at 1 month and decreased to 29% after 1 year. Postoperative needling, in conjunction with intraoperative MMC use and postoperative intrableb 5-FU injection, was found efficacious and saved further surgery in some intractable cases (98). Regression of rubeosis, sometimes seen after trabeculectomy with MMC, has been suggested to be a pharmacologic side effect of MMC and not necessarily the effect of IOP lowering alone (99). In a preliminary study, trabeculectomy 1 month after use of intravitreal bevacizumab resulted in a decrease in anterior segment neovascularization and fewer complications (100). Even if an anti-VEGF agent is used, the effects of these agents are temporary, and further injections or panretinal photocoagulation may be needed for long-term control of neovascularization.
Modifications for Previous Intraocular Surgery
The fornix-based conjunctival flap, as previously discussed (16–18,26), is particularly useful in eyes that have had previous intraocular surgery involving the conjunctiva—for example, when a fornix-based conjunctival flap has been used during a cataract procedure. The conjunctiva in these eyes is usually tightly scarred down to episclera near the limbus, making preparation of a limbus-based flap difficult. When using a fornix-based flap, it is probably best to suture the lateral margins of the scleral flap to promote drainage posteriorly. An anterior vitrectomy may also be required if loose vitreous is in the anterior chamber or presents at the iridectomy site. Nonpenetrating trabeculectomy was once advocated for glaucoma in aphakia (101). However, early results from the Tube versus Trabeculectomy study indicate that implantation of glaucoma drainage devices may be a better alternative for these cases (102).
Use of antimetabolites for trabeculectomy in pseudophakic eyes may improve the success rate. However, in aphakic and pseudophakic eyes of children, after congenital cataract surgery, trabeculectomy was successful in only one third of patients, regardless of whether MMC was used during the surgery (103). Implantation of glaucoma drainage devices has been gaining broader acceptance in these challenging cases.
Adjunctive Devices
The Ex-PRESS mini glaucoma shunt (Fig. 38.10) is a stainless steel device that was originally developed to be implanted subconjunctivally through the limbus, providing direct communication between the anterior chamber and subconjunctival space, resembling a full-thickness procedure, relying upon the intrinsic resistance of the device. Although successful in lowering IOP, procedures using this device had high complication rates, and as a result, surgeons began implanting the shunt device beneath a partial-thickness scleral flap (104,105). The technique of implantation and indications of use resemble those of trabeculectomy (i.e., a guarded filtration procedure), aside from the absence of an iridectomy. In a retrospective comparison with trabeculectomies, implantation with Ex-PRESS mini glaucoma shunts achieved similar IOP control but had a lower rate of early postoperative hypotony (106).
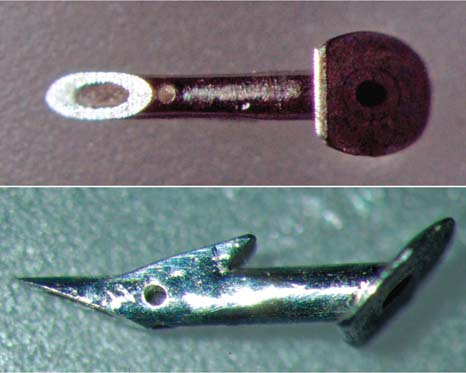
Figure 38.10 R-50 model of Ex-PRESS mini glaucoma shunt (actual length, approximately 400 microns.
Wound Healing
The most common cause of failure in glaucoma filtering surgery is scarring of the filtering bleb (107). The increased amount of collagen in the failed blebs suggests that proliferation of fibroblasts with associated production of collagen and glycosaminoglycans is important in the response to filtering surgery (3). However, as discussed in Chapter 37, wound healing is a complex process with several phases, and it is likely that bleb failure in filtering surgery involves many of these factors and certain unique characteristics of the glaucomatous eye. Newer antifibrotic agents and drug delivery systems are under development in an effort to improve efficacy and safety.
Influence of Aqueous Humor on Wound Healing
Aqueous humor normally slows or fails to support the growth of conjunctival fibroblasts in tissue culture (108–110). A possible explanation is that aqueous contains one or more inhibitory factors for fibroblast proliferation. Cell culture studies have shown that the high concentration of ascorbic acid, normally present in aqueous humor, is cytotoxic to dividing human Tenon capsule fibroblasts, which may contribute to the development of a successful filtering bleb (111). Aqueous humor also contains a wide variety of growth factors, which maintain the normal function of ocular tissues in health and have a significant role in abnormal states and wound healing (112). Transforming growth factor-β (TGF-β), a potent modulator of tissue repair, is in human aqueous and plays a role in the healing process after glaucoma filtering surgery (113). Contrary to the influence of primary aqueous humor, aqueous obtained shortly after intraocular surgery or mixed with 20% desiccated embryo extract does promote proliferation of fibroblasts (110,114). Secondary aqueous humor has also been shown to stimulate the proliferation of cultured corneal endothelial cells (115). In addition, aqueous humor has chemoattractant activity for ocular fibroblasts, and this activity is significantly greater in eyes with previously failed glaucoma surgery (116). Therefore, components of normal aqueous humor and alterations in some glaucoma patients are likely to influence both success and failure of the filtering bleb.
Other Factors Affecting Wound Healing
Numerous studies have suggested that young age and African heritage adversely influence the outcomes of glaucoma filtering surgery. The explanation for these observations is not clear. Histologic studies of conjunctival specimens obtained before trabeculectomy in patients with chronic open-angle glaucoma (COAG) showed no significant influence of age or ethnicity on conjunctival factors that might relate to surgical outcome (117,118). A more significant influence may be chronic topical glaucoma medical therapy before trabeculectomy. Some studies have identified long-term topical combination therapy as a risk factor for failure of trabeculectomy (119,120), although one study that compared success rates before and after the introduction of topical β-blockers did not indicate that the preoperative use of topical medication influenced the outcome of surgery (121). Histologic studies of conjunctiva from patients after long-term topical glaucoma medical therapy revealed a significant degree of subclinical inflammation (122,123), although one study could only correlate the number of goblet cells with successful outcomes (124). Conjunctival impression cytology correlated significant degrees of metaplasia with the number of glaucoma medications used (125). One clinical study, however, indicated that stopping topical adrenergic therapy and adding use of topical corticosteroids 1 month before surgery was associated with a decrease in the number of conjunctival fibroblasts and inflammatory cells and an improvement in the success rate of trabeculectomy (126). Another study suggested that a high number of conjunctival goblet cells may be a predictor of lower IOP after trabeculectomy without use of antimetabolites (127). The number of conjunctival fibroblasts and inflammatory cells increases after previous ocular surgery involving the conjunctiva, possibly causing an increased risk of trabeculectomy failure (128).
Antifibrotic Agents
Corticosteroids
Considerable attention has been given to measures—primarily medication use—that may prevent bleb failure by modulating the wound healing process. The first of these to be used clinically were the corticosteroids. Tissue culture studies of human Tenon capsule fibroblasts have shown that both corticosteroids and nonsteroidal anti-inflammatory drugs inhibit cell attachment and proliferation (129,130). Clinical investigations have confirmed the efficacy of topical corticosteroids, although no additional benefit was achieved with systemic steroids (131,132). It has also been suggested that subconjunctival triamcinolone before filtering surgery may improve the success rate (133). Despite the benefit of corticosteroids, the incidence of bleb failure remains high with certain types of glaucoma (e.g., glaucoma in aphakia and pseudophakia and neovascular glaucoma), which has prompted the search for additional agents to modify wound healing.
5-Fluorouracil
5-FU was the first drug to be studied extensively as an adjunct to corticosteroids in the control of wound healing following trabeculectomy. This pyrimidine analog antimetabolite, which blocks DNA synthesis through the inhibition of thymidylate synthesis, has been shown to inhibit fibroblast proliferation in cell cultures (134,135). The subconjunctival injection of 5-FU after filtering surgery significantly improved bleb formation in monkeys and improved the rate of success in difficult clinical cases (136–138). A subsequent multicenter, randomized clinical trial of 213 patients with glaucoma in aphakia or pseudophakia or a previous failed filter in a phakic eye confirmed the ability of 5-FU to improve the success rate of filtering surgery in these high-risk cases (139,140). However, the protocol required twice-daily subconjunctival injections of 5-mg 5-FU for 7 days and then once daily for 7 more days. In addition, serious complications included conjunctival wound leaks and corneal epithelial defects in the early postoperative course, plus an increased risk for late-onset bleb leakage (139,140). Therefore, lower effective doses, alternative delivery systems, and alternative agents have been sought.
Success has been reported with daily injections of 5-mg 5-FU for 7 to 14 days (141–143), which probably represents the most common range of dosages in current use. In one study of patients with COAG and “secondary” glaucoma or refractory glaucoma, the average total dose of 5-FU was 36.5, 36.0, and 49.5 mg, respectively, and the probability of IOP control below 16 mm Hg with 5-year follow-up was 77.9%, 66.8%, and 26.9%, respectively (143). Adjunctive use of 5-FU increases the success rate of trabeculectomy in eyes undergoing initial filtering surgery, patients younger than 40 years, infants, and patients requiring extremely low IOPs (144–148). However, the complication rate is higher than in trabeculectomy without 5-FU, and caution is advised, especially with initial surgery (140). There is a high risk of failure in patients with neovascular glaucoma (149). The treatment is believed to be most effective if started prophylactically on the first postoperative day, although success has been reported with starting 3 to 15 days postoperatively when signs of impending bleb failure are noted (150,151). Several clinical trials have shown that 5-FU is also beneficial when used intraoperatively, usually on a surgical sponge soaked in 25 to 50 mg/mL of the drug and applied to the surgical site for 5 minutes (152–156). The type of sponge can also affect the intraocular tissue levels of 5-FU delivered (157).
Mitomycin C
Use of MMC was reported by Chen (158) in 1983 to enhance the IOP-lowering efficacy of trabeculectomy when applied intraoperatively in eyes at high risk for surgical failure. MMC is an antineoplastic antibiotic isolated from Streptomyces caespitosus. Tissue culture studies of human Tenon capsule fibroblasts revealed almost complete inhibition of fibroblast proliferation (159), the degree of which correlated with the outcome of filtering surgery (160). When compared with 5-FU, the effect on rabbit fibroblast proliferation was much more prolonged with MMC (161). 5-FU was toxic to cultured mouse fibroblasts while sparing bovine vascular endothelial cells, whereas MMC was cytotoxic for both cell types (162). Intraoperative application of MMC in rabbits significantly prolonged bleb duration after glaucoma filtering surgery (163). Subsequent clinical trials supported the benefit of MMC use as an adjunct to trabeculectomy (164), and randomized comparisons with postoperative use of subconjunctival 5-FU generally showed intraoperative use of MMC to have superior IOP-lowering efficacy after trabeculectomy (165–169). MMC has been shown to enhance the success rate of trabeculectomy for refractory glaucoma in black patients, in glaucoma associated with uveitis, in congenital and developmental glaucoma, in normal-tension glaucoma, and in primary, uncomplicated trabeculectomies (170–176). A retrospective study has shown that primary trabeculectomy with MMC maintained an IOP level of 15 mm Hg or less in more than 80% of patients after 1 year and in 60% after 6 years, suggesting that the use of MMC may be justified in primary trabeculectomies in patients with severe glaucoma (177). However, care must be exercised with the use of adjunctive MMC, especially in the primary, uncomplicated cases, because of the significant incidence of serious complications.
Although adjunctive use of MMC is less likely to cause the postoperative complications that are typically associated with 5-FU, such as corneal epithelial toxicity and wound leaks (165–168), it is associated with other complications that can be even more serious. The most significant of these is hypotony maculopathy, in which prolonged IOP reduction is associated with disc edema, vascular tortuosity, and chorioretinal folds in the macular area, potentially producing marked reduction in visual acuity (178). The main cause of the hypotony is excessive filtration, and histologic studies of excised overfiltering blebs have revealed an irregular epithelium and a largely acellular subepithelium of loosely arranged connective tissue (179–181). However, another mechanism of hypotony may be aqueous hyposecretion, in that one enucleated human eye revealed disruption of the ciliary body epithelium beneath the site of MMC application (181). Other potential complications, as suggested by animal studies, include anterior chamber reaction and corneal endothelial toxicity if the MMC gains entry into the eye (182,183). (The management of these complications is discussed later in the chapter.) The following modifications in technique may minimize the complications.
In early protocols, a sponge soaked in MMC, 0.5 mg/mL, was applied to the subconjunctival tissues for 5 minutes. Subsequent attempts to reduce the risk of hypotony have included reduced concentrations and exposure times (179,184). It has also been suggested that adjustment of exposure time according to each patient’s risk of excessive fibrosis may enhance the balance between successful IOP control and incidence of complications (179). Some retrospective studies suggested that MMC, 0.2 mg/mL, applied for 2 minutes may be as effective as higher doses but may be associated with few complications (184,185). However, the optimum protocol has yet to be established.
Various sponges have been advocated as vehicles for MMC, including Merocel and various microsurgical sponges, and it may be that manipulating the size or shape of the sponge can influence the effect of the MMC (186–188). One study suggested that placing the sponge beneath the scleral flap rather than over intact episclera may improve the success rate without increasing complications (177,189). In rabbits, irrigating the ocular tissues with balanced salt solution after removal of the sponge substantially reduced intraocular diffusion of MMC (190).
In an experimental model, irrigation reduced the MMC concentration only in the external half of the sclera, leaving the deep intrascleral concentrations unchanged (191), suggesting that a lower-dose MMC application without irrigation may be a rational approach (192). Intraoperative application of MMC without touching the conjunctiva or Tenon capsule was ineffective in inhibiting the development of thin, avascular blebs in eyes undergoing primary trabeculectomy (193).
Other Antifibrotic Agents
Alternative agents that have been evaluated as antiproliferative drugs include cytosine arabinoside, bleomycin, rapamycin, doxorubicin, daunorubicin, 5-fluorouridine, 5’-monophosphate, 5-fluoroorotate, heparin, Taxol, cytochalasin-B, colchicine, immunotoxins, and interferon-α-2b (134,194–207). Suramin, a substance that inhibits the action of growth factors, was evaluated in rabbits and in humans in a prospective study (208,209). The use of suramin had fewer complications, compared with use of MMC, with similar success rates, suggesting that it may become an alternative to antimetabolite therapy in glaucoma surgery (209). Beta irradiation also inhibited fibroblast proliferation in tissue culture and delayed wound healing in rabbits (210–212). In a preliminary clinical trial, beta irradiation did not improve the results of trabeculectomies (213), although a study of patients aged 18 years or younger with congenital glaucoma suggested a beneficial effect on the prognosis of trabeculectomy (214). Amniotic membrane transplantation or subconjunctival perfluoropropane (C3F8) gas has been suggested as a safer alternative to MMC (215–217).
In addition to drugs that influence fibroblast proliferation, agents have also been evaluated that will alter other phases of the wound healing process. For example, tissue plasminogen activator, which causes localized fibrinolysis, γ-interferon and calcium ionophores, which inhibit collagen biosynthesis, and β-aminopropionitrile and d-penicillamine, which inhibit cross-linking of collagen, have shown promise in in vitro and in vivo studies (218–227). Perioperative injection of bevacizumab has also shown promise to decrease conjunctival scarring and vascularity (228,229).
TGF-β is a potent stimulant of scarring, and it has been identified as an important component of wound healing, particularly in the conjunctival scarring response (230). It has been found in human aqueous and appears to play a role in the healing process after glaucoma filtering surgery (113). Inhibition of TGF-β appears to be a more physiologic approach to wound healing modulation (231,232).
Although subconjunctival administration of a TGF-β2 antibody in the postoperative period improved the outcome of glaucoma surgery in an animal model and appeared more efficacious than 5-FU without some of the side effects (233), a randomized, controlled trial of CAT-152, a monoclonal antibody against TGF-β2, was no more effective than placebo and required frequent subconjunctival injections in the postoperative period (234). Tranilast (N-3′,4′-dimethoxycinnamoyl-anthranilic acid), a drug with antikeloid and antiscarring properties, inhibits TGF-β1 secretion and therefore could be a promising drug to prevent scarring after glaucoma filtration surgery (235–237).
In the future, combinations of agents may be administered according to the various phases of the wound healing process to prevent bleb failure.
Earlier Full-Thickness Fistulas
Sclerectomy
The original type of limbal fistula, which has been largely replaced by trabeculectomy with or without adjunctive use of antifibrosis agents, involves the creation of a direct opening through the full thickness of the limbal tissue. The fistula may be created by using various techniques.
In 1906, LaGrange (238) described a technique in which a full-thickness limbal incision was made, and a piece of tissue was then excised from the anterior lip of the wound to create a limbal fistula. Holth (239) modified this procedure 3 years later by performing the sclerectomy with a punch. However, the sclerectomy technique that became most popular in the mid-20th century was the posterior lip sclerectomy described by Iliff and Haas (240).
Trephination
In 1909, Elliot (241) and Fergus (242) described a glaucoma filtering procedure in which the fistula was created with a small trephine placed just behind the corneolimbal junction. Elliot (243) later modified the technique by splitting the peripheral cornea and placing the trephine more anteriorly (sclerocorneal trephining). However, this modification produced a thinner filtering bleb with an increased chance of late infection, and Sugar (244) advocated a return to the original, more posterior placement of the trephine, which he called limboscleral trephination (or trepanation) (245) (Fig. 38.11).
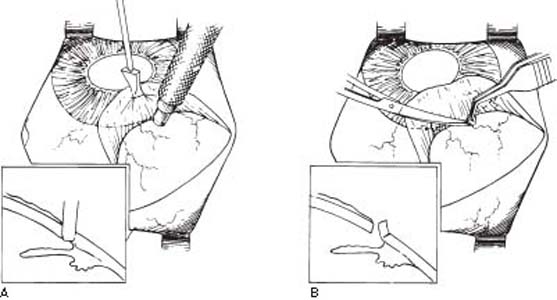
Figure 38.11 Limboscleral trephination. A: Trephine button partially excised by tilting the trephine anteriorly. B: Completion of excision by cutting posterior attachment with scissors.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


