Anatomic Principles of Glaucoma Surgery
All laser and incisional surgical procedures for glaucoma are designed to reduce the intraocular pressure (IOP) by increasing the rate of aqueous humor outflow or reducing aqueous production. The involved anatomy, therefore, is the anterior ocular structures related to aqueous outflow and the portions of the ciliary body associated with aqueous inflow. To properly perform any of the operations that make up the armamentarium of glaucoma surgery, the surgeon must be familiar with both the internal and external aspects of these structures. In this chapter, we consider these portions of the ocular anatomy as they relate to glaucoma surgery.
AN OVERVIEW OF THE ANATOMY
The structures involved in aqueous humor dynamics—that is, aqueous production and aqueous outflow—are in immediate proximity to each other in the periphery of the anterior ocular segment. The interrelationship between these structures is considered in Chapter 1 with a stepwise construction of a schematic model that may be summarized as follows.
At the junction between the cornea and the sclera is the transitional zone of connective tissue known as the limbus. On the inner surface of the limbus, extending for 360 degrees, is a depression, referred to as the scleral sulcus. The anterior margin of this sulcus slopes gradually into the peripheral cornea, while the posterior margin contains a lip of connective tissue called the scleral spur. This spur might be thought of as the dividing point between the structures of aqueous outflow anteriorly and those of aqueous production posteriorly. The trabecular meshwork attaches in part to the anterior side of the scleral spur and extends forward to blend into the sloping anterior wall of the scleral sulcus, which converts the sulcus into the Schlemm canal. The bulk of aqueous humor in the anterior chamber flows through the trabecular meshwork to the Schlemm canal, from where it leaves the eye via intrascleral channels and episcleral veins.
The ciliary body inserts into the posterior portion of the scleral spur. This is actually the only firm attachment of the ciliary body, with the remaining surfaces between the sclera and the ciliary body creating a potential space, referred to as the supraciliary space. The ciliary processes, the actual site of aqueous production, occupy the innermost and anteriormost portion of the ciliary body. The iris inserts into the ciliary body just anterior to the ciliary processes. Consequently, a peripheral iridectomy, as performed during glaucoma filtering surgery, often allows visualization of two to four ciliary processes. The insertion of the iris is usually such that a portion of the anterior ciliary body remains gonioscopically visible between the iris root and scleral spur. This is referred to as the ciliary body band, the physical entrance to the uveoscleral outflow pathway. The remainder of the trabecular meshwork—that is, the portion not inserted to the scleral spur—attaches to this band and to the peripheral iris.
INTERNAL ANATOMY
Ciliary Body
Most of the ciliary body is located posterior to the iris (Fig. 34.1) and cannot be directly visualized except in unusual circumstances, such as with marked iris retraction or absence of portions of the iris. The anterior 2 to 3 mm of the ciliary body, the pars plicata, is thicker than the posterior portion and contains the radial ridges of the ciliary processes. The latter are the site of aqueous production and the target of cyclodestructive procedures. In those unusual circumstances in which they can be visualized directly (by using cycloscopy), direct treatment with laser transpupillary cyclophotocoagulation or endoscopic visualization may be possible. When direct visualization is not possible, an indirect, transscleral route can be used for cyclodestruction, requiring the use of external landmarks (discussed later in this chapter). The posterior 4 mm of the ciliary body is the thinner pars plana, which must also be approached by using external landmarks.
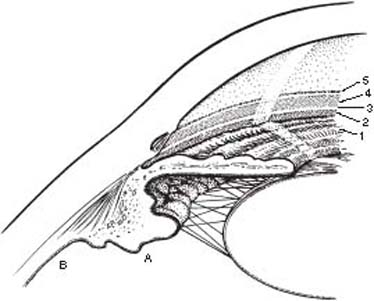
Figure 34.1 Internal anatomy. The ciliary body is located just posterior to the iris and is divided into the pars plicata (A) and the pars plana (B). The remaining internal structures can be seen by gonioscopy and include 1, iris; 2, ciliary body band; 3, scleral spur; 4, trabecular meshwork; 5, Schwalbe line.
Structures Visualized by Gonioscopy
The following structures in the anterior chamber can be visualized by gonioscopic examination and are involved in several laser and incisional glaucoma surgical procedures.
Iris
The iris is the posteriormost structure of the anterior chamber angle. It is helpful to remember that the peripheral portion of the iris is thinner than the more central iris, which makes it, among other reasons, the preferred site for a laser iridotomy. Other anatomic considerations related to optimum laser iridotomy sites are iris crypts, or thinner areas of stroma that may be easier to penetrate. In addition, areas of increased pigmentation, such as iris freckles, may improve the absorption of laser energy in lightly pigmented eyes when using argon laser. It is generally preferred to place the iridotomy so that it is fully covered by the upper lid, to minimize the side effect of intermittent glare (1). However, peripheral iridotomies can result in symptomatic glare in any position.
Ciliary Body Band
The ciliary body band is located just anterior to the root of the iris; it typically has a dark gray or brown appearance on gonioscopic examination. The width of this band varies considerably from one patient to the next. Eyes with myopia often have a wide band, and those with hyperopia a narrow band. Surgeons should avoid confusing the pigmented ciliary body band with the trabecular meshwork in patients with lightly pigmented meshwork, especially when interpreting the depth of the anterior chamber angle. This is particularly relevant when performing laser trabeculoplasty. The patient usually lets the surgeon know when the latter mistake is made, because the ciliary body contains many nerve endings and is sensitive to the application of laser energy.
Scleral Spur
The scleral spur is seen gonioscopically as a white line just anterior to the ciliary body band. In some patients, visualization of the spur may be obscured because of variable degrees of high iris process insertion (but discontinuous; continuous areas of high iris insertion are peripheral anterior synechiae) or heavy pigment dispersion. This was the principal site of surgery with a cyclodialysis procedure, an operation of historical interest, in which an aqueous outflow pathway in the suprachoroidal space was constructed by separating ciliary body from the scleral spur. In the early stages of neovascular glaucoma, new vessels may be seen extending across the scleral spur from the iris and ciliary body to the trabecular meshwork. The vessels can be obliterated at this site with laser applications in a procedure called goniophotocoagulation, which is also rarely used today.
Trabecular Meshwork
Just anterior to the scleral spur is the functional portion of the trabecular meshwork, the portion adjacent to the Schlemm canal through which the aqueous humor drains. This portion of the meshwork is demarcated gonioscopically by the presence of variable amounts of pigment. Because this pigment is presumably carried to the meshwork from uveal tissue by the aqueous humor flow, it is typically light in young individuals and varies considerably among individuals later in life according to the amount of intraocular pigment release. In some patients, especially with pathologic states such as the pigment dispersion syndrome and exfoliation syndrome, the meshwork is heavily pigmented. In other individuals, the meshwork may be so lightly pigmented that it is hard to see, which can lead to the incorrect diagnosis of a narrow, or even closed, anterior chamber angle. In some of these cases, blood reflux into the Schlemm canal or iris processes, which typically extends to the meshwork, may help identify this structure.
It is this pigmented portion of the trabecular meshwork to which the laser energy should be applied during argon laser trabeculoplasty, which delivers its energy within a 50-µm spot. However, there is another, less pigmented portion of the meshwork just anterior to the functional, pigmented portion. When performing argon laser trabeculoplasty, overlapping the laser beam between the pigmented and nonpigmented portions of the meshwork—that is, along the anterior border of the pigmented portion—may help reduce the complications of transient postoperative IOP rise and peripheral anterior synechia formation. Selective laser trabeculoplasty delivers its energy in a 400-µm spot; with this procedure, centering the spot over the entire trabecular meshwork is preferable.
When performing trabeculectomy ab interno, the scleral spur and trabecular meshwork must be clearly identified to initially penetrate through the trabecular meshwork into the Schlemm canal. If one penetrates posterior to the scleral spur, the probe will enter the suprachoroidal space, resulting in a substantially increased risk of complications.
Schwalbe Line
The Schwalbe line is the anteriormost structure in the anterior chamber angle and represents the junction between the nonpigmented portion of the trabecular meshwork and the peripheral cornea. In most individuals, a portion of this junction is represented by a small ridge. This is an important landmark when performing a goniotomy, in that the internal incision in that operation is made just posterior to the Schwalbe line. The structure may be difficult to visualize gonioscopically, unless there has been a moderate degree of pigment dispersion, in which case there may be a buildup of pigment along the anterior side of the ridge, especially inferiorly. Care must be taken to avoid confusing this pigmented line with the trabecular meshwork when performing laser trabeculoplasty. In other cases in which pigmentation is minimal, the location of the Schwalbe line can be established gonioscopically to help determine the depth of the peripheral anterior chamber. A fine beam of light from the slitlamp can be seen reflecting from both the anterior and posterior surfaces of the peripheral cornea. As the clear portion of the peripheral cornea approaches the Schwalbe line, it is replaced externally by opaque limbal tissue, which causes the two beams to converge at the Schwalbe line, providing a useful way for determining the location of this structure.
EXTERNAL ANATOMY
Anterior Limbus
On the external surface of the eye, the anterior boundary of the limbus is defined as the termination of the Bowman membrane, which is approximately 0.5 mm anterior to the insertion of the conjunctiva and Tenon capsule (Fig. 34.2). This has been referred to as the corneolimbal junction, or the apparent or anterior limbus. It is important to note that the conjunctiva inserts more anteriorly in the superior and inferior quadrants. Consequently, the limbus is wider in these quadrants, ranging between 1 and 1.5 mm, and gradually tapers to the narrowest width in the nasal and temporal quadrants, where the range is between 0.3 and 0.5 mm (2). In performing glaucoma filtering surgery, some surgeons choose to take advantage of the wider areas of the limbus by placing the surgical site at the 12-o’clock position. When performing surgery that involves the ciliary body, such as a cyclodestructive procedure or a pars plana incision, the surgeon should remember that these structures are slightly more posterior in relation to the apparent limbus in the superior and inferior quadrants.
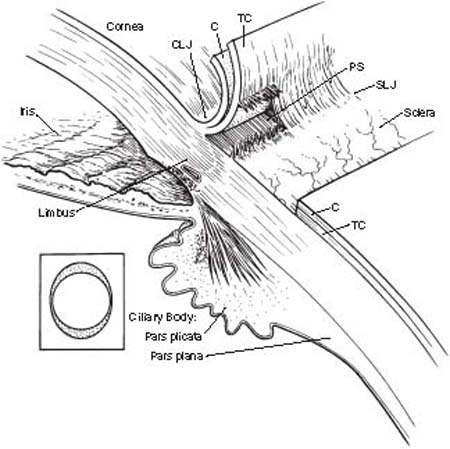
Figure 34.2External anatomy. On the external surface, the limbus is bounded posteriorly by the sclerolimbal junction (SLJ) and anteriorly by the corneolimbal junction (CLJ). The width of the limbus varies from a maximum superiorly to a minimum on the sides (inset) due to the relative insertion of the conjunctiva (C). The Tenon capsule (TC) is firmly attached to limbal connective tissue approximately 0.5 mm behind the conjunctival insertion, creating a potential space (PS). Cyclodestructive procedures should be placed over the pars plicata, usually 1.0 to 1.5 mm posterior to the corneolimbal junction, whereas a posterior sclerotomy should be made through the pars plana, approximately 3 to 4 mm posterior to the corneolimbal junction.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


