Cholinergic Stimulators and Hyperosmotic Agents
With the introduction of newer medications that have improved efficacy and few side effects, the cholinergic stimulators and hyperosmotic agents have a limited role in glaucoma management. Introduced in the 1870s, pharmacologic agents that mimic the cholinergic effects of acetylcholine are referred to as cholinergic agonists, parasympathomimetics stimulators, or miotics because of their effect on the pupil (Fig. 32.1).Among the acetylcholinesterase inhibitors, which have limited availability, only echothiophate iodide is discussed. The hyperosmotic agents are another class of compounds administered systemically (orally or intravenously) in short-term, emergency situations, such as with acute angle-closure glaucoma or other glaucomas involving dangerously high intraocular pressures (IOPs). Although many consider these drugs of historical interest, the cholinergic stimulators and hyperosmotic agents remain useful in specific clinical situations.
Figure 32.1 Chemical structures of the direct acting muscarinic agent, pilocarpine (A), and the indirect acting muscarinic agent, echothiophate (B).
MECHANISMS OF ACTION
Cholinergic Stimulators
The cholinergic agents (Table 32.1) (1) are indicated for use in all forms of open-angle glaucoma where the aqueous outflow system is functionally intact. They share a common mechanism of action by stimulating muscarinic cholinergic receptors. Among the five receptor subtypes (2), the m3 muscarinic receptor is the predominant subtype expressed in human ciliary muscle cells and iris sphincter (3). They lower IOP by increasing facility of aqueous outflow (see the modified Goldmann equation in Chapter 2) by ciliary muscle contraction, which causes traction on the scleral spur and alters the configuration of the trabecular meshwork and Schlemm canal (Fig. 32.2). This mechanism is supported by primate and human studies. Disinserting the ciliary muscle from the scleral spur in monkeys eliminates the effect of pilocarpine on IOP and facility of outflow (4). Histologic studies of human eyes treated with pilocarpine before enucleation for malignant melanoma demonstrate a posterior, internal pull on the scleral spur, with trabecular space widening, endothelial meshwork distention, an increase in giant vacuoles, and larger, more frequent pores in the inner endothelium of the Schlemm canal (5). Primate studies suggest that the increase in giant vacuoles is a result of enhanced aqueous flow through the outflow system rather than a direct action of pilocarpine on the endothelium of the Schlemm canal (6.)
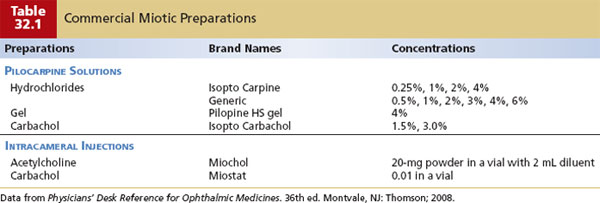
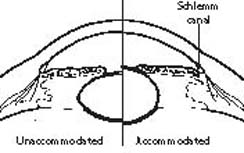
Figure 32.2 Schematic mechanism of ciliary muscle contraction on anterior segment anatomy. After applying a topical cholinergic medication, the ciliary muscle fibers contract, leading to traction on the scleral spur and altering aqueous outflow through the trabecular meshwork and Schlemm canal. An accommodative effect is also mediated by a decrease in concentric diameter of the ciliary body with “rounding” of the lens and a slight decrease in the anterior chamber depth.
Other aqueous humor dynamic effects have been investigated. Fluorophotometric studies in humans show minimal stimulation of aqueous humor formation with pilocarpine (7). Pilocarpine decreases uveoscleral outflow (8), which may have clinical significance in eyes with markedly reduced conventional or trabecular outflow. As these eyes become increasingly dependent on unconventional or uveoscleral drainage, pilocarpine may cause a paradoxical rise in IOP (9). Episcleral venous pressure does not appear to be altered by pilocarpine (10).
The miotic effect, caused by pilocarpine and related compounds, is produced by stimulating muscarinic receptors of the iris sphincter muscle. This effect “tightens” the iris and helps open the anterior chamber island, making pilocarpine a useful adjunct in the short-term management of angle closure resulting from relative pupillary block (see Chapter 12).
Hyperosmotic Agents
The most widely accepted mechanism of action for the hyperosmotic agents is reduction of vitreous volume due to a change in osmotic gradient between the blood and ocular tissues, which lowers IOP. This concept is supported by rabbit studies that demonstrate a reduction in vitreous body weight of approximately 3% to 4% after administration of mannitol (11). With time, a variable amount of the hyperosmotic agent may enter the eye, depending on the permeability of the blood–ocular barriers to the drug and the size of the drug molecules. As the compound is cleared from the systemic circulation, there may be a reversal of the osmotic gradient in some cases, resulting in a transient rise in IOP.
ADMINISTRATION
Cholinergic Stimulators
Pilocarpine solution is applied topically and is largely degraded in the cornea (12), with less than 3% entering the anterior chamber (13). The IOP-lowering effect is dose related up to pilocarpine, 4% (14,15). In darkly pigmented eyes, pilocarpine, 6%, may produce additional IOP reduction (16). Based on pharmacokinetic studies in animals and pharmacodynamic studies in humans (13,14,17), pilocarpine is given four times daily. However, one study reported that pilocarpine, 2%, administered twice daily, followed by nasolacrimal occlusion gave maximal IOP response (18).
Although not commonly prescribed, another formulation of 4% pilocarpine hydrochloride is a high-viscosity acrylic vehicle (Pilopine), which is applied at bedtime and produces a significant IOP reduction for 24 hours (19). It was comparable to pilocarpine hydrochloride drops, four times daily (20,21), with less induced myopia and impaired visual acuity.
Although not commonly prescribed, carbachol is a dual-action parasympathomimetic that produces direct muscarinic receptor stimulation and an indirect parasympathomimetic effect by inhibiting acetylcholinesterase. Carbachol has poor corneal penetration and requires an adjuvant, such as benzalkonium chloride, to achieve therapeutic levels (22). The usual dosage is three times daily. A carbachol, 1.5%, three times daily—the usual dosage—was as potent and effective as pilocarpine, 2%, four times a day (23). There appears to be no significant difference in the effectiveness of pilocarpine compared with carbachol.
Even less commonly used are the acetylcholinesterase inhibitors, and only echothiophate iodide (phospholine iodide), 0.125%, is currently available in the United States. Echothiophate had the advantage of a prolonged duration of action, with the maximum effect occurring in 4 to 6 hours and a substantial residual present after 24 hours, allowing it to be used on a twice-daily regimen.
Another route of administration is intracameral injection of either carbachol or acetylcholine to achieve miosis during surgery. After cataract surgery, intracameral carbachol has been shown to provide better IOP control in the early postoperative period, compared with intracameral acetylcholine or placebo using balanced salt solution (24,25).
Hyperosmotic Agents
The systemic administration of a hyperosmotic agent is occasionally used as an emergency method of lowering the IOP or preoperatively to minimize the “posterior pressure” effect of the vitreous in a supine position. Although not widely used, glycerin (Osmoglyn) is administered orally in a dose of 1 to 1.5 g/kg (or 2 to 3 cc/kg) of body weight of a 50% solution (26,27). The ocular hypotensive effect occurs within 10 minutes of administration, peaks in 30 minutes, and lasts for approximately 5 hours (26,27).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


