Carbonic Anhydrase Inhibitors
Carbonic anhydrase inhibitors (CAIs) are the only class of drugs that are used as systemically administered agents in chronic glaucoma therapy. The CAIs belong to the sulfonamide class of drugs. In 1954, acetazolamide was introduced as an ocular hypotensive drug, and most of the information in this chapter is based on experience with this drug. Methazolamide is another commercially available systemic CAI, but dichlorphenamide (available in Europe and Australia) and ethoxyzolamide are no longer available in the United States. After overcoming the challenges for topical drug delivery due to limited ocular absorption and bioavailability, both topical CAI drugs, dorzolamide and brinzolamide, have assumed a role in the management of glaucoma. The CAIs all share the same basic mechanism of action of lowering intraocular pressure (IOP) by decreasing aqueous humor flow through inhibition of carbonic anhydrase (CA) in ciliary epithelium. Side effects of the oral compounds essentially differ only in degree and are much less with the use of topical drugs.
MECHANISMS OF ACTION
CA is responsible for the catalytic hydration of CO2 and dehydration of H2CO3:

The physiologic effects of CAIs are related to ion transport, metabolic acidosis, blood flow, and fluid transport that are described in the following text. There are 14 gene forms of CA encoding for CA isoenzymes that have various cellular and tissue distributions and physiologic effects (1,2). In the eye, four CA isoenzymes, CA I through CA IV, have been identified (3). The main therapeutic target of CAIs in the ciliary processes is the cytosolic CA II isoform (formerly called type C). In patients who have CA II deficiency, acetazolamide fails to decrease IOP, suggesting that this isozyme is inhibited by the drug (4).
Based on the catalytic reaction described earlier, the two effects of ion transport and acidosis are closely related. Changes in ion transport associated with aqueous humor secretion are expected to be altered by CAIs, which is the main mechanism of action of the CAIs to decrease aqueous humor formation. Acetazolamide decreases aqueous humor formation in the human eye about 30% compared with only 18% for topical dorzolamide (5). When added to timolol, which alone reduced daytime flow by 33%, the combination of the two aqueous suppressants reduced the flow rate by 44% (6). When dorzolamide is added to timolol, there is an additive effect to suppress aqueous humor flow (7).
Acetazolamide creates a local acidic environment (8) that inhibits net chloride flux across the ciliary epithelium, but the principal ions affected by CAIs have not been established in human eyes. Metabolic acidosis is known to reduce IOP and may be another mechanism of action for oral CAIs (9). However, the ocular hypotensive effect of these drugs does not depend on alterations of pH in the blood or aqueous humor (10).
Ocular blood flow is complex and involves consideration of the various vascular beds, including the retinal, choroidal, and retrobulbar vessels located within their respective tissues (11). Acetazolamide increases blood flow and blood-flow velocity within the middle cerebral artery of the brain but not in the ophthalmic and central retinal arteries (12). In a recent review of 35 specific studies, the meta-analysis provided the evidence that topical CAIs increase ocular blood-flow velocities in the retinal circulation, central retinal, and short posterior ciliary arteries but not in the ophthalmic artery (13).
The other clinical effect of CA relates to the fluid movement from the retina toward the choroid (14). Acetazolamide has been shown to increase the rate of subretinal fluid absorption in experimental retinal detachment (15) and to increase the adhesion between retina and pigment epithelium (16). It may also be effective in the treatment of macular edema in patients with retinal pigment epithelial cell disease and uveitis (17,18). However, CAIs do not reduce macular edema associated with primary retinal vascular diseases (17).
ADMINISTRATION
Oral Carbonic Anhydrase Inhibitors
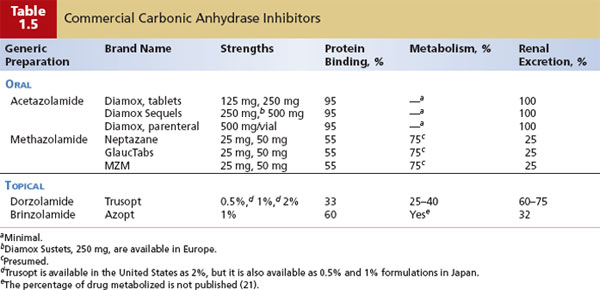
To achieve the therapeutic effect of reducing aqueous humor production, more than 90% of the CA activity needs to be inhibited (19). For this reason, the drug must be used in adequate doses (20). Because the free amount of drug determines the pharmacologic effect, understanding the protein binding of the drug (i.e., how much drug is taken up by serum proteins and blood cells) is important. Acetazolamide is highly bound compared with methazolamide, which explains why larger doses are required for acetazolamide to achieve its therapeutic effect compared with methazolamide. The drugs are not extensively metabolized and are primarily excreted in the urine (Table 31.1).
The traditional oral dose for long-term acetazolamide therapy in adults is 250-mg tablets every 6 hours or 500-mg sustained-release capsules twice each day (22). For children, the recommended dose of acetazolamide is 5 to 10 mg/kg of body weight every 4 to 6 hours (23). In tablet form, the ocular hypotensive effect peaks in 2 hours and lasts up to 6 hours, whereas that of the capsule peaks in 8 hours and persists beyond 12 hours. For more rapid action, acetazolamide may be given intravenously, which provides a peak effect in 15 minutes and lasts up to 4 hours. A useful routine for emergencies, such as acute angle-closure glaucoma, is to give 250 mg of acetazolamide intravenously if the patient is unable to tolerate oral administration of two 250-mg tablets.
An alternative oral regimen with methazolamide is to begin with 25 mg of methazolamide given twice daily, advancing to 50 mg twice daily and up to 100 mg taken three times daily (23). The advantage is that the drug can be used in smaller dosages, which cause fewer side effects, because the drug has a longer plasma half-life than acetazolamide and a lower rate of protein binding, allowing the free drug to distribute into tissues and be more active on a weight basis in reducing aqueous production (24). A 500-mg sustained-release capsule of acetazolamide had a greater ocular hypotensive effect and was better tolerated than methazolamide (25,26). Generic acetazolamide tablets and sequels are commercially available, providing significant cost savings.
Topical Carbonic Anhydrase Inhibitors
Dorzolamide
Approved in the United States in 1998, dorzolamide (Fig. 31.1) lowers the IOP by reducing aqueous humor flow by inhibiting the CA II isoenzyme in the ciliary body (27). At 2 hours after dosing, dorzolamide causes 14.7% to 27% reduction in IOP, and at 8 hours after dosing, 12.9% to 17.5% reduction in IOP (28,29). A 2% solution is the only strength available in the United States, but 0.5% and 1% formulations are available in Japan. The recommended administration is three times daily because there is greater IOP lowering compared with two times daily. It is most frequently administered twice daily for adherence.
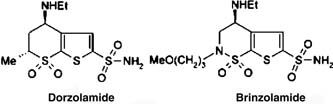
Figure 31.1 Chemical structure of dorzolamide (Trusopt) and brinzolamide (Azopt), topical CAIs.
In a 1-year trial comparing timolol, 0.5%, and betaxolol, 0.5%, both given twice daily, the mean percentage IOP reduction with dorzolamide was 23%, compared with 25% and 21% with timolol and betaxolol, respectively (30). Adjunctive therapy studies have shown that twice-daily dorzolamide provides additional IOP lowering in patients being treated with timolol, 0.5%, twice daily (31). When compared with pilocarpine four times daily as a second drug in patients whose IOP was uncontrolled with timolol, 0.5%, dorzolamide three times daily gave similar additional IOP reduction and was preferred by patients because of reduced side effects (32). When dorzolamide, 2% three times daily, was added to once-daily latanoprost, IOP was reduced by an additional 15% (33).
Several studies have reported on the use of dorzolamide in the pediatric population. In a randomized study comparing dorzolamide, 2%, three times daily with timolol gel once daily combined with placebo two times daily in children with glaucoma or elevated IOP younger than 6 years, dorzolamide lowered IOP by as much as 23.3% and was well tolerated, compared with timolol (34). In a review of published studies reported on childhood glaucoma, additive therapy of twice-daily dorzolamide to once-daily timolol appeared to be the most effective and best tolerated compared with α2-agonists and prostaglandin analogues (35).
The IOP-lowering effect of the fixed combination of dorzolamide, 2%, and timolol, 0.5%, (Cosopt) is similar to that of the same drugs dosed separately (36). In a randomized study comparing the 24-hour efficacy and tolerability of a fixed combination of dorzolamide, 2%, and timolol, 0.5%, versus timolol, 0.5%, the dorzolamide–timolol combination exhibited greater IOP lowering than timolol during the daytime but not at night (37). It is now available in generic form, providing considerable cost savings.
Brinzolamide
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


