Glaucomas after Ocular Surgery
Many diverse forms of glaucomas occur as complications of various ocular surgical procedures, including glaucoma surgery, cataract extraction and related procedures, corneal transplantation, and vitreoretinal surgery.
MALIGNANT (CILIARY BLOCK) GLAUCOMA
Terminology
In 1869, von Graefe (1) described a rare complication of certain ocular procedures that was characterized by shallowing or flattening of the anterior chamber and an elevation of the intraocular pressure (IOP). He called the condition malignant glaucoma because of the poor response to conventional therapy. The concept of malignant glaucoma has been expanded to include various clinical situations, which have these common denominators: shallowing or flattening of the central and peripheral anterior chambers, elevation of the IOP, and unresponsiveness to or aggravation by use of miotics but frequent relief with cycloplegic–mydriatic therapy (2,3).
Studies of the mechanism of malignant glaucoma (considered later in this chapter) led some investigators to recommend new terms for this group of diseases. On the basis of the theory that obstruction of normal aqueous flow is caused by apposition of the ciliary processes against the equator of the lens or the anterior hyaloid, the name ciliary block glaucoma was proposed (4,5). The term aqueous misdirection is also commonly used to denote the concept of posterior diversion of the aqueous due to the ciliary block. To describe the concept that a forward shift of the lens pushes peripheral iris into the anterior chamber angle, the term direct lens block angle closure has been suggested (6). There is no universal agreement on the terminology for this group of conditions; the traditional term, malignant glaucoma, is retained for purposes of discussion in this text. When discussing this term with patients, however, the physician should be aware that the term malignant may have unintended and undesirable connotations, and it is therefore advisable to provide appropriate context when using this term or to use an alternative term.
Clinical Forms
Whether all the clinical conditions called malignant glaucoma should actually be included in a single disease category is not yet established. Nevertheless, the following disorders have been described under that name.
Classic Malignant Glaucoma
Classic malignant glaucoma is the prototype and most common form of the disease group. It typically follows incisional surgical intervention for angle-closure glaucoma and is reported to complicate 0.6% to 4% of these cases (2,3,7). Neither the type of surgery nor the IOP immediately before surgical intervention appears to be related to the postoperative development of malignant glaucoma (3). However, partial or total closure of the anterior chamber angle at the time of surgery is associated with an increased incidence of this complication (3). An acute angle-closure attack may be a predisposing factor, because when malignant glaucoma occurs, it frequently does so in an eye with previous angle closure, although the angle may have been open preoperatively (7). Conversely, the condition rarely follows a prophylactic iridectomy when the angle is open at the time of surgery (7).
The classic presentation is a unilateral disorder in the early postoperative period after incisional surgery. However, cases have been reported after laser iridotomy, and bilateral cases have been reported with both incisional and laser procedures that, although the actual mechanisms may differ, do clinically resemble classic forms of the disease (8–10). Some cases may not have an elevated IOP (11); others may occur months to years later, after the cessation of cycloplegic therapy or the institution of miotic drops (2,3,10).
Malignant Glaucoma in Aphakia
Although classic malignant glaucoma typically occurs in phakic eyes, it may persist after lens removal for treatment of the disease or develop after cataract extraction in eyes without preexisting glaucoma (3). It is important to differentiate malignant glaucoma in aphakia and in its other forms from pupillary block glaucoma and delayed suprachoroidal hemorrhage (discussed later in this chapter).
Malignant Glaucoma in Pseudophakia
Malignant glaucoma may be associated with an intraocular lens implant in the anterior chamber, presumably by the same mechanism as malignant glaucoma in aphakia (12). It has also been observed in eyes with posterior chamber implants, with or without an associated glaucoma filtering procedure (Fig. 26.1) (13). Malignant glaucoma has also occurred after implantation of an intraocular lens in the posterior chamber of a phakic eye (i.e., malignant glaucoma induced by a phakic intraocular lens in the posterior chamber of a patient with myopia) (14).


Figure 26.1 Ciliary block after cataract extraction and posterior chamber lens implantation.A: The central chamber is shallow; the peripheral chamber is flat. The intraocular lens is pushed forward, and the haptic posterior to the iris is indenting the iris surface.B: After disruption of the posterior capsule and anterior hyaloid face with Nd:YAG laser, the chamber immediately deepens; the intraocular lens is no longer pressed against the iris. (Courtesy of E. Hodapp, MD. From Werner MA, Grajewski AL. Glaucoma in aphakia and pseudophakia. In: Tasman W, Jaeger EA, eds. Duane’s Clinical Ophthalmology. Vol 3. Philadelphia, PA:Lippincott Williams & Wilkins; 2008:chap 54G.)
Miotic-Induced Malignant Glaucoma
The onset of classic malignant glaucoma may correspond to the institution of miotic therapy, suggesting a causal relationship (15). Although the precise mechanism behind this relationship is unknown, the action of miotics may produce malignant glaucoma through contraction of the ciliary body or associated forward shift of the lens with shallowing of the anterior chamber. Similar clinical pictures have been described in unoperated eyes receiving miotic therapy and in an eye treated with miotics after a filtering procedure for open-angle glaucoma (16,17).
Malignant Glaucoma Associated with Bleb Needling
A case of malignant glaucoma after needling of a trabeculectomy bleb has been reported (18). It is possible that bleb needling results in a shallowing of the anterior chamber that predisposes to malignant glaucoma.
Malignant Glaucoma Associated with Inflammation and Infection
Inflammation and trauma are also precipitating factors of malignant glaucoma (6). A form of malignant glaucoma is associated with endophthalmitis caused by fungal keratomycosis and the atypical bacterium Nocardia asteroides (19).
Malignant Glaucoma Associated with Other Ocular Disorders
Retinal detachment surgery caused the malignant glaucoma syndrome in a patient who developed choroidal detachments after a buckling procedure (20). However, the anterior chamber shallowing in this situation may be secondary to an anterior uveal effusion with forward rotation of the lens or iris diaphragm, producing a secondary angle-closure glaucoma that resembles malignant glaucoma. Several cases of malignant glaucoma–like syndrome have been reported after pars plana vitrectomy (21,22), and one case reported after diode laser cyclophotocoagulation (23). The condition has also been noted in children with retinopathy of prematurity and in a patient with corneal hydrops in keratoconus (24,25).
Spontaneous Malignant Glaucoma
Malignant glaucoma may rarely develop spontaneously in an eye without previous surgery, miotic therapy, or other apparent cause (26).
Theories of Mechanism
There is a lack of general agreement regarding the sequence of events responsible for the development of malignant glaucoma, although the following are the more popular theories.
Posterior Pooling of Aqueous
Shaffer (27) hypothesized that an accumulation of aqueous behind a posterior vitreous detachment causes the forward displacement of the iris–lens or iris–vitreous diaphragm. The concept was subsequently expanded to include the pooling of aqueous in vitreous pockets. This theory is supported by an ultrasonographic study of eyes with malignant glaucoma in aphakia demonstrating echo-free zones in the vitreous from which aqueous was reportedly aspirated (28). The mechanisms leading to the posterior diversion of aqueous are uncertain, although strong evidence supports the following possibilities.
Ciliolenticular (Ciliovitreal) Block
In cases of malignant glaucoma, the tips of the ciliary processes rotate forward and press against the lens equator in the phakic eye or against the anterior hyaloid in aphakia, which may create the obstruction to forward flow of aqueous (4,29) (Figs. 26.2 and 26.3, respectively). Studies involving ultrasonographic biomicroscopy have confirmed the anterior rotation of the ciliary processes (30,31); two studies also showed a shallow collection of supraciliary fluid (31,32). This concept led to the proposed term ciliary block glaucoma as a substitute for malignant glaucoma (4).
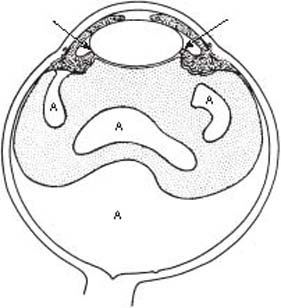
Figure 26.2 Concept of ciliolenticular block as the mechanism of malignant glaucoma. Apposition of the ciliary processes to the lens equator (arrows) causes a posterior diversion of aqueous (A), which pools in and behind the vitreous with a forward shift of the lens–iris diaphragm.
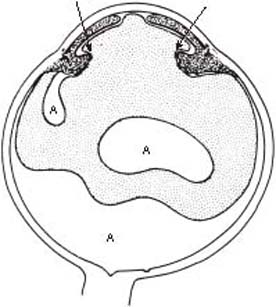
Figure 26.3 Concept of ciliovitreal block as the mechanism of malignant glaucoma in aphakia. Apposition of ciliary processes against the anterior hyaloid (arrows) leads to posterior diversion of aqueous (A), which causes a forward shift of the vitreous and iris.
Anterior Hyaloid Obstruction
The anterior hyaloid may contribute to ciliolenticular block, and breaks in the hyaloid near the vitreous base possibly allow the posterior diversion of aqueous (5) (Fig. 26.4). The hyaloid breaks, however, have a one-way valve effect, because fluid coming anteriorly closes the vitreous face against the ciliary body, preventing forward flow (5). Some investigators have observed the ciliolenticular contact but noticed that the spaces between the ciliary processes were open, with vitreous visible behind them, suggesting that the obstruction to anterior aqueous flow is the anterior vitreous face, which is compressed forward against the ciliary processes in phakic and aphakic forms of malignant glaucoma (3).
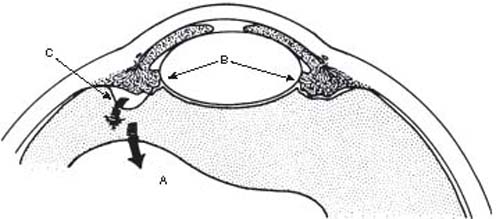
Figure 26.4 The anterior hyaloid may contribute to the ciliolenticular block (B), and breaks in the hyaloid near the vitreous base (C) may allow the aqueous (A) to be diverted posteriorly (arrows).
In perfusion studies with animal and human eyes, resistance to flow of a fluid through vitreous increases significantly with an elevation of pressure in the eye (33–35). The increased resistance might be caused by compression of the vitreous and its displacement against the ciliary body, lens, and iris, thereby reducing the available area of anterior hyaloid through which fluid could flow (34,35). These clinical and laboratory observations support the concept that an intact anterior hyaloid may be important in preventing the forward movement of aqueous as it travels anteriorly.
Slackness of Lens Zonules
Chandler and Grant (36) postulated that the forward movement of the lens–iris diaphragm in malignant glaucoma might be caused by abnormal slackness or weakness of the zonules of the lens as well as pressure from the vitreous. Others have also advocated this theory and suggested that the laxity of the zonules might be the result of severe, prolonged angle closure (7), or ciliary muscle spasm induced by surgery, miotics, inflammation, trauma, or other unknown factors (6). The concept that the lens subsequently pushes the peripheral iris into the anterior chamber angle led to the proposed term of direct lens block angle closure (6).
It seems likely that malignant glaucoma is a multifactorial disorder, in which one or more elements of the aforementioned mechanisms may be involved, depending on the clinical context.
Differential Diagnosis
The diagnosis of malignant glaucoma requires the exclusion of the following conditions (3,5).
Pupillary Block Glaucoma
Pupillary block is the most difficult entity to distinguish from malignant glaucoma but must be ruled out before the latter diagnosis can be made. During slitlamp biomicroscopy, attention should be focused on two questions. First, is the central anterior chamber moderately deep with bowing of the peripheral iris into the chamber angle, as typically noted in pupillary block, or is the entire iris–lens diaphragm shifted forward with marked shallowing or loss of the central anterior chamber, more consistent with malignant glaucoma (Fig. 26.5)? Second, and probably of more diagnostic value, is a patent iridectomy present? If the iridectomy is clearly patent, a pupillary block mechanism is unlikely. However, if patency cannot be confirmed, the diagnosis of pupillary block cannot be ruled out, and one should proceed with a definitive laser iridotomy.
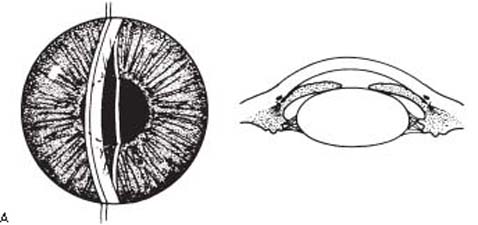
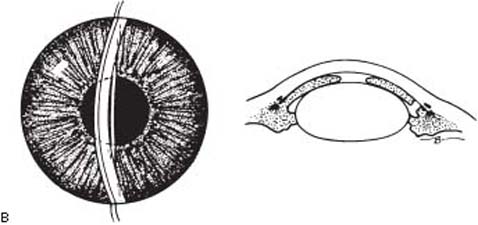
Figure 26.5 Distinctions between pupillary block glaucoma and malignant glaucoma. A: In pupillary block glaucoma, there is moderate depth to the central anterior chamber with forward bowing of the peripheral iris and absence of a patent iridectomy. B: In malignant glaucoma, the entire lens–iris diaphragm is shifted forward with marked shallowing or loss of the central anterior chamber, and a patent peripheral iridectomy may be present.
Choroidal Detachments
Choroidal separation with serous fluid is common after glaucoma filtering procedures and might be confused with malignant glaucoma because of the shallow or flat anterior chamber. These eyes typically are hypotonus. However, when the anterior chamber is flat, IOP measurements by Goldmann applanation tonometry, pneumotonometry, or a Tono-Pen are often highly inaccurate, tending to overestimate the IOP, and therefore cannot be relied on to distinguish between excessive filtration and malignant glaucoma (37). A more helpful diagnostic finding is the presence of a choroidal detachment, which is easily seen if there is adequate visibility of the posterior segment—or alternatively, the presence of choroidal fluid observed by ultrasonography.
Most serous choroidal detachments will resolve spontaneously as IOP rises. However, those that are persistent or massive with central touch can be approached surgically by making scleral incisions in the inferior quadrants. If a characteristic straw-colored fluid is obtained from the suprachoroidal space, the diagnosis of serous choroidal detachment is confirmed, and the procedure is completed by draining as much suprachoroidal fluid as possible and reforming the anterior chamber with air or saline, or both.
A case series has been reported of patients with occult annular ciliary body detachment giving rise to angle-closure glaucoma that is clinically indistinguishable from malignant glaucoma (38). Ultrasonographic biomicroscopy facilitated the diagnosis and guided subsequent management.
Suprachoroidal Hemorrhage
Suprachoroidal hemorrhage may occur hours or days after ocular surgery and create shallowing or loss of the anterior chamber, which is typically associated with pain and elevated IOP. It is often preceded by ocular hypotony. The eye is usually more inflamed than with serous choroidal detachment, and the choroidal elevation is frequently dark reddish–brown. The surgical approach is the same as that for serous choroidal detachments, with drainage of the blood from the suprachoroidal space though the sclerotomies and reformation of the anterior chamber.
Management of Malignant Glaucoma
Medical Management
Chandler and Grant (36) reported in 1962 that mydriatic–cycloplegic treatment was effective for malignant glaucoma, and the next year Weiss and colleagues (39) recommended the use of hyperosmotics to combat this condition. Cycloplegics, by virtue of stimulating contraction of the ciliary body, help pull the lens back by tightening the zonules, helping to break the ciliary block, whereas the presumed benefit of a hyperosmotic agent is to reduce the pressure exerted by the vitreous (5,36,39). These two measures, along with the use of aqueous suppressants, help reduce the flow of aqueous that perpetuates shallowing of the anterior chamber and resultant malignant glaucoma. A standard medical regimen includes the use of topical atropine two to three times daily, intravenous mannitol, topical β-blocker or α2-agonist (or both), and oral or topical carbonic anhydrase inhibitors. After the attack is broken, the patient should be maintained indefinitely on atropine therapy to prevent recurrences.
Surgical Management
Medical treatment of malignant glaucoma is effective in approximately one half of cases within 5 days (2,3). If the condition persists beyond this time, surgical intervention is usually indicated.
Laser Techniques
Argon laser photocoagulation of the ciliary processes that can be visualized through an iridectomy or transscleral diode laser cyclophotocoagulation has been reported to relieve malignant glaucoma, presumably by breaking the ciliolenticular block (40,41). Nd:YAG laser can also be effective in treating aphakic and pseudophakic malignant glaucoma by disrupting the anterior hyaloid face or the posterior lens capsule and hyaloid face (42).
Slitlamp Needle Revision
When the anterior hyaloid face is accessible in the anterior segment and an Nd:YAG laser is not accessible, performing transcorneal needling to disrupt the anterior vitreous face and reform the anterior chamber may be possible (43).
Posterior Sclerotomy and Air Injection
A pars plana incision with aspiration of liquid vitreous with reformation of the anterior chamber with an air bubble (Fig. 26.6) is felt by some to be the incisional surgical procedure of choice for classic malignant glaucoma (2,3,5). It has been suggested that the sclerotomy should be placed 3 mm posterior to the limbus to break the anterior hyaloid, thereby reducing its contribution to the blockade (5). Postoperatively, patients are generally maintained on atropine to avoid recurrence.
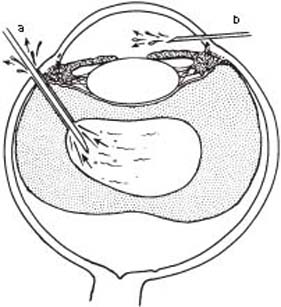
Figure 26.6 Posterior sclerotomy and air injection in the management of malignant glaucoma. Fluid is drained or aspirated from the vitreous by means of a pars plana incision (a) and the anterior chamber is deepened with air (b).
Anterior Pars Plana Vitrectomy
Other surgeons prefer a careful removal of the anterior vitreous including the anterior hyaloid with vitrectomy instruments (44–46). Failure to include the anterior hyaloid may result in recurrence of malignant glaucoma. Results with posterior sclerotomy and anterior vitrectomy techniques are favorable, but both have the potential for serious complications. The preferred method of treatment depends on the surgeon’s experience and preference.
Lens Extraction
This is favored by some surgeons as the incisional surgical procedure of choice, whereas others use this approach if the posterior sclerotomy and air injection or anterior vitrectomy fails (47). To be effective, lens extraction should be combined with an incision of the anterior hyaloid and possibly with deep incisions into fluid pockets in the vitreous (2,3).
Management of the Fellow Eye
When malignant glaucoma has already occurred in one eye, the fellow eye will also probably develop the condition if it undergoes intraocular surgery. For this reason, it is best to do a prophylactic laser iridotomy, if indicated. However, if angle-closure glaucoma is present, every effort should be made to break the attack before surgery and, if the attack cannot be broken, mydriatic–cycloplegic therapy should be used vigorously after iridotomy and continued indefinitely.
GLAUCOMAS IN APHAKIA OR PSEUDOPHAKIA
Terminology
The term aphakic or pseudophakic glaucoma is occasionally seen in the literature. It is mentioned in this text only to discourage its use because it implies that a single form of glaucoma is associated with aphakia or pseudophakia. There are many mechanisms by which cataract extraction, with or without intraocular lens implantation, can lead to glaucoma, and it is best to refer to these glaucomas in aphakia or pseudophakia by terms that describe the particular events leading to the IOP elevation.
Incidence
The IOP may be elevated transiently in the early postoperative period or may become chronically elevated at any time after cataract surgery.
Aphakia
In the days before intraocular lens implantation, a rise in IOP during the first several days after cataract extraction was not uncommon, although the frequency of this complication varied according to the surgical technique used for wound closure (48). Chronic glaucoma in aphakia was much less common than the early, transient pressure rise. In one series of 203 uncomplicated cataract extractions, persistent glaucoma occurred in 3% of the eyes (49). However, these chronic cases posed a much greater threat to vision and a much more difficult therapeutic challenge than the eyes with transient pressure elevation did.
Pseudophakia
The advent of extracapsular cataract extraction and posterior chamber intraocular lens implantation was generally associated with a reduced incidence of long-term IOP elevation (50). In one series of 373 eyes undergoing cataract surgery, those receiving intracapsular extraction and anterior chamber (133 eyes) or iris fixation (31 eyes) lenses had a late mean IOP rise of 0.8 mm Hg, whereas those undergoing extracapsular surgery with posterior chamber implants (209 eyes) had a mean IOP fall of 0.6 mm Hg (51). Eyes undergoing phacoemulsification cataract extraction also had IOP lowering of 1.1 to 2.5 mm Hg for at least 6 months postoperatively (52). However, extracapsular and phacoemulsification cataract surgeries are associated with pressure complications in the early and late postoperative periods. In eyes without preexisting glaucoma, more than one half in one series had an IOP of 25 mm Hg or more 2 to 3 hours postoperatively (53), and the IOP exceeded 23 mm Hg on the first postoperative day in 29% of eyes in another study (54). Chronic glaucoma was seen in 4% of eyes after standard extracapsular extraction in one series and in 2.1% of another large series (54,55). Postoperative glaucoma also occurred in 11.3% of eyes receiving secondary anterior chamber implants (56).
With any cataract procedure, early and late postoperative IOP elevations can occur by a wide variety of mechanisms.
Mechanism of Intraocular Pressure Elevation
Influence of Viscoelastic Substances
To protect the corneal endothelium and maintain anterior chamber depth during certain stages of cataract extraction and intraocular lens implantation, filling the anterior chamber with a viscous aqueous substitute has become common practice. The viscoelastic substance that has received the most extensive evaluation for this purpose is sodium hyaluronate (Healon). Although some surgeons have found no significant postoperative pressure rises associated with the use of sodium hyaluronate (57), others have documented high pressures in the first few days after surgery (58). Sodium hyaluronate injected into the anterior chamber of rabbit and monkey eyes caused marked pressure rises (59), and perfusion in enucleated human eyes decreased the outflow facility by 65% (60). This was not reversed by vigorous anterior chamber irrigation, but facility was restored to baseline by irrigation with hyaluronidase. The most likely mechanism of IOP elevation is temporary obstruction of the trabecular meshwork by the viscoelastic.
Alternative viscoelastic substances have also been evaluated. Chondroitin sulfate caused minimal pressure elevation when used during lens implantation in various animal eyes or when injected as a 10% concentration into the anterior chamber of rabbit and monkey eyes (59,61). A formulation of chondroitin sulfate and sodium hyaluronate (Viscoat) was compared with sodium hyaluronate and was less advantageous during cataract surgery in one study and caused IOP rises in the immediate postoperative period in many patients (62). In another study, the duration of IOP elevation was found to be shorter with formulation including chondroitin sulfate (63). A modified sodium hyaluronate viscoelastic (Healon GV), which has a higher molecular weight, viscosity, and sodium hyaluronate concentration than Healon, was associated with a similar postoperative IOP course to that of the latter agent (64). Patients receiving a newer viscoelastic, Healon 5, with special rheologic properties had a lower IOP in the postoperative period, compared with patients receiving Viscoat (65); however, in other studies, postoperative IOP spike did not differ between patients receiving Healon 5 and those receiving other viscoelastics (66,67). Use of ethylcellulose (1% to 2%) did not cause a significant postoperative pressure rise in animal or human eyes and appeared to provide good protection of the corneal endothelium (60,68). In comparative trials, hydroxypropyl methylcellulose, 2%, was found to have the same effect on corneal thickness as balanced salt solution with no rise in IOP and the same early, mild IOP elevation as with sodium hyaluronate 1% (69,70).
Inflammation and Hemorrhage
Transient postoperative inflammation occurs to some degree after every cataract extraction. When excessive, obstruction of the trabecular meshwork by inflammatory cells and fibrin may lead to IOP elevations. The inflammatory response and associated glaucoma may be particularly prominent when lens fragments are retained in the vitreous after extracapsular cataract extraction (71).
Intraocular lens implants increase the risk of serious postoperative uveitis, especially with anterior chamber lenses and, historically, with iris-supported lenses (72). This may be associated with hyphema and glaucoma, which has been referred to as the uveitis, glaucoma, and hemorrhage (UGH) syndrome (73). Uveitis was particularly common with the iris-supported lenses, apparently because of the movement of the lens against the iris and the subsequent cellular reaction (74,75). The inflammation and hemorrhage with anterior chamber lenses is thought to be caused by the contact of the rough posterior surface of the lens with the iris. This has been borne out on ultrasonographic biomicroscopy, which can help detect malpositioned haptics (especially with posterior chamber lenses) and be used to plan subsequent surgical intervention (76). The degree to which lens–iris contact liberates pigment may be related to the design and quality of the specific lens (73,77). Posterior chamber lenses are least likely to induce uveitis. Fluorophotometric studies have shown that pseudophakic eyes with a posterior chamber lens and an intact posterior lens capsule have minimal alteration in the blood–aqueous barrier (78).
In addition to hyphema associated with uveitis, bleeding in the aqueous or vitreous compartments may be seen immediately after cataract surgery or as a late or recurring complication. One source of the late hemorrhage is new vessels in the corneoscleral wound (79). Intraocular lens implantation may also be complicated by late or recurrent hemorrhage, which has been reported with anterior chamber, iris fixation, and posterior chamber implants (80–82). Posterior chamber implants usually have sulcus fixation, and the mechanism in all cases is presumably erosion into the adjacent tissue. Postoperative bleeding from any source may lead to IOP elevation by the mechanisms discussed in Chapter 24, including ghost cell glaucoma from a vitreous hemorrhage (83).
Pigment Dispersion
Variable amounts of pigment granules, primarily from the iris pigment epithelium, are dispersed into the anterior chamber with all cataract operations. Excessive pigment dispersion can lead to transiently elevated IOP in aphakic or pseudophakic eyes, with the latter occasionally leading to a chronic form of glaucoma.
Pseudophakic pigmentary glaucoma is most often associated with posterior chamber lenses (84,85). Pigment dispersion is produced by rubbing of the iris pigment epithelium against the optic and loops of the intraocular lens. This leads to the dispersion of pigment granules, which cause obstruction of the trabecular meshwork—a process similar to phakic pigmentary glaucoma. Acute pigmentary glaucoma has been reported with one-piece lenses in which one of the haptics has dislocated into the sulcus. Pigment granules on the central corneal endothelium (i.e., Krukenberg spindle) are occasionally noted. Pigment granules may be visualized circulating in the aqueous humor in the anterior chamber, especially after pupillary dilatation. The most useful diagnostic finding is iris transillumination defects at the site of contact with the lens implant. Gonioscopy typically reveals heavy pigmentation of the trabecular meshwork.
Unilateral IOP elevation and bilateral pigmentary dispersion syndrome have been reported after implantation of phakic refractive intraocular lenses (86). Acquired pigmentary glaucoma should be considered for patients with phakic intraocular lenses. These patients should be monitored for this condition.
Vitreous Filling the Anterior Chamber
Grant (87) described a mechanism of acute open-angle glaucoma in which vitreous humor fills the anterior chamber after cataract surgery; this could be cured in some cases by mydriasis to minimize pupillary block, but other eyes required miosis to draw the vitreous from the angle. Simmons (88) observed that many cases resolve spontaneously in several months. When surgical intervention is required, an iridotomy may be curative, but other eyes will require an anterior vitrectomy (89).
Pupillary Block
In Aphakia
This is a relatively rare complication of intracapsular cataract extraction (90). It is more likely to occur weeks after a transient flat anterior chamber secondary to a wound leak. The condition may also be more common after surgery for congenital cataracts. A combination of sector and peripheral iridectomies may minimize this complication (91). Modern approaches to congenital cataract surgery render these measures unnecessary, although a peripheral iridectomy is still advisable.
The pathogenesis of pupillary block in aphakia can be caused by adherence between the iris and anterior vitreous face, which increases the resistance of aqueous humor flow into the anterior chamber through the pupil or iridectomy. In these cases, the aqueous humor accumulates behind the iris, causing a forward shift of the iris and narrowing of the anterior chamber angle (Fig. 26.7). The mechanism may be dependent on an intact anterior hyaloid, because fluorescein studies have shown that aqueous will flow preferentially through spontaneous openings in the vitreous face (92). This condition may be distinguished from the much less common malignant glaucoma in aphakia by the deeper central anterior chamber and forward bowing of the peripheral iris in the eyes with aphakic pupillary block glaucoma (93) (Fig. 26.8).
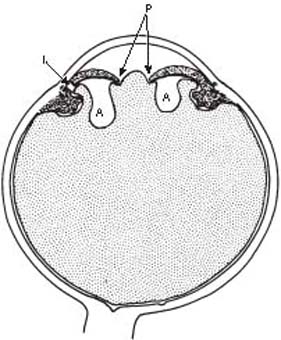
Figure 26.7 Pupillary block in aphakia. An adherence between the iris and anterior vitreous face blocks the flow of aqueous into the anterior chamber at the pupil (P) and iridectomy site (I). The posterior accumulation of aqueous (A) causes forward bowing of the peripheral iris with closure of the anterior chamber angle.

Figure 26.8 Slitlamp view of an eye with pupillary block in a patient with aphakia shows the hyaloid face (H) well back from the cornea (C) centrally but peripheral anterior bowing of the iris (I) with closure of anterior chamber angle.
In Pseudophakia
Pupillary block glaucoma in pseudophakia was once seen most often with anterior chamber and iris-supported lenses, although there are numerous reports of this complication occurring with posterior chamber lenses (94,95). It usually appears early after surgery but may rarely be delayed months or years. Many cases are asymptomatic and are discovered on routine postoperative examination. Some may even have a normal IOP, although peripheral anterior synechiae and chronic pressure elevation usually follow if the peripheral anterior chamber depth is not promptly restored. With anterior chamber lenses, the iris bulges forward on either side of the lens (Fig. 26.9), whereas the mechanism with posterior chamber lenses appears to be excessive inflammation with posterior synechiae to the intraocular lens or the anterior lens capsule (96).
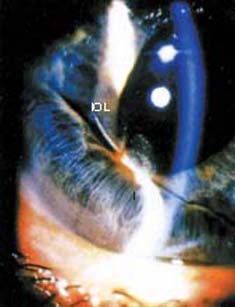
Figure 26.9 Slitlamp view of pupillary block in a pseudophakic eye shows forward bulging of the iris (I) peripheral to the margin of the anterior chamber intraocular lens (IOL).
With modern cataract techniques and intraocular lens implantation in the posterior chamber, the incidence of pupillary block glaucoma in pseudophakia is sufficiently low that a peripheral iridectomy is no longer a routine part of cataract surgery. However, when excessive postoperative inflammation is anticipated or when combined with a filtering procedure, an iridectomy is still advisable in most cases.
Peripheral Anterior Synechiae or Trabecular Damage
In most cases of chronic glaucoma in aphakia or pseudophakia, peripheral anterior synechiae are present, presumably because of a flat anterior chamber or the presence of inflammation or debris in the early postoperative period. Flat anterior chambers after cataract surgery may be caused by a wound leak with subsequent hypotony and choroidal detachments. To avoid the complication of peripheral anterior synechiae and chronic glaucoma, a flat anterior chamber should be corrected promptly. In one series of 203 uncomplicated cataract extractions, 47% had some degree of peripheral anterior synechiae, and all of those with associated glaucoma had peripheral anterior synechiae present in more than one quarter of the filtering angle (49).
In other cases of glaucoma in aphakia or pseudophakia, the angle may be open in all quadrants and appear essentially normal. The mechanism of aqueous outflow obstruction in cases of chronic open-angle glaucoma (COAG) in aphakia or pseudophakia is uncertain, but it most likely is related to alterations in the trabecular meshwork due to the surgery and possibly a preexisting reduction in outflow facility. In many of these patients, COAG may have been present but undiagnosed preoperatively.
Distortion of the Anterior Chamber Angle
Kirsch and colleagues (97) described the gonioscopic appearance of an internal white ridge resembling an inverted snowbank along the inner margins of the corneoscleral incision after routine cataract extraction. For approximately the first 2 weeks, the ridge typically obscures visualization of the trabecular meshwork and then gradually recedes over the next few months. There is some controversy regarding the pathogenesis of the internal ridge. Campbell and Grant (98) provided evidence that distortion of the anterior chamber angle is induced by tight corneoscleral sutures, whereas Kirsch and colleagues suggested that edema of the deep corneal stroma is the mechanism (97). Whatever the initiating factors may be, the ridge is known to be associated with the formation of peripheral anterior synechiae, vitreous adhesions, and hyphema. In some cases, it is likely that the white ridge contributes to the early, transient pressure elevation after cataract surgery. In one study of 95 cataract extractions, early IOP rise occurred in 23% of the eyes with limbal incisions but in none with corneal incisions, suggesting that distortion produced by the corneoscleral wound temporarily affects the adjacent trabecular meshwork and aqueous outflow (99).
Glaucoma after Congenital Cataract Surgery
Children tend to have a higher incidence of glaucoma after cataract extraction than adults do. In the United Kingdom, the overall annual incidence of postoperative glaucoma was approximately 5% and the median time to development of glaucoma was 1.3 years (range, 0.4 months to 6.7 years) (100). Younger age at detection of cataract was independently associated with the development of glaucoma. In other studies, the reported prevalence of glaucoma after congenital cataract surgery ranged from 6.1% to 24% (101–103). Although most of the reported cases have involved an open-angle mechanism, a pupillary block mechanism is not uncommon in children with aphakic or pseudophakia. This may be another situation in which an iridectomy is indicated as a part of the cataract surgery. The use of a vitrectomy instrument to aspirate the cataract, with wide excision of the posterior capsule, may reduce the incidence of postoperative glaucoma in children (101). However, even with automated lensectomy and vitrectomy in children, some studies reveal glaucoma rates of 12.5% to 24% (102,103). One study found an increased risk for glaucoma in eyes that underwent postoperative secondary membranectomy for visual axis occlusion, especially when secondary membranectomy was performed within 1 year of primary surgery (104).
Influence of α-Chymotrypsin
Glaucoma via this mechanism is rarely seen today but was common in the era of intracapsular surgery. In 1958, Barraquer (105) demonstrated the value of the enzymatic zonulolysis with α-chymotrypsin in facilitating intracapsular cataract extraction, and the enzyme was commonly used for that purpose. In 1964, Kirsch (106) reported a transient pressure rise in 75% of the eyes in which 2 to 4 mL of a 1:5000 dilution of the enzyme was used, compared with a 24% incidence of high pressures in a group without enzyme. The complication was somewhat more common in patients with preexisting COAG (107).
Nd:YAG Laser Posterior Capsulotomy
Another cause of IOP elevation after extracapsular cataract extraction or phacoemulsification is the use of Nd:YAG laser to perform a discission in the posterior lens capsule when that structure becomes significantly opacified after the initial surgery. In numerous studies, the procedure was associated with significant pressure elevation. The pressure rise may be detected in the first few hours, and the IOP usually returns to its baseline level within 1 week; in some eyes, however, the IOP elevation may last for several weeks, and several large series have revealed persistent or late-onset pressure elevations in 0.8% to 6% of the cases (108,109). Cases have been reported in which the laser-induced pressure elevation caused progressive glaucomatous visual field loss or transient loss of light perception, requiring emergency paracentesis (110,111). Other causes of visual loss after Nd:YAG capsulotomy include cystoid macular edema and retinal detachment (112). Risk factors for significant IOP elevations after Nd:YAG capsulotomy differ among studies, but they include preexisting glaucoma or a preoperative IOP greater than 20 mm Hg, large capsulotomies, a sulcus rather than capsular fixed posterior chamber lens, the absence of a posterior chamber lens, myopia, vitreoretinal disease, vitreous prolapse into the anterior chamber, and the total amount of laser energy used (113–115).
The mechanism of IOP elevation after Nd:YAG capsulotomy is not fully understood, although tonographic studies have shown that it is related to reduced aqueous outflow (115,116). Most cases have an open-angle mechanism, and the obstruction of the trabecular meshwork may be with fibrin and inflammatory cells due to a breakdown in the blood–aqueous barrier or debris from the capsule or cortical remnants (117). Other reported mechanisms of IOP elevation include pupillary block due to forward movement of the vitreous and herniated vitreous occluding a preexisting glaucoma surgical fistula (118,119). Pretreatment with topical apraclonidine, timolol, brimonidine, or topical carbonic anhydrase inhibitors is done to minimize the early postoperative rise in IOP (120).
Management
Preoperative Considerations
In preparing for a cataract operation, certain considerations may help to minimize the risk of postoperative complications related to glaucoma, particularly in eyes with preexisting glaucoma.
Pressure Reduction
Many surgeons elect to reduce the vitreous volume and IOP by applying external pressure to the globe before surgery to maintain a deep anterior chamber and to minimize the potential complications of vitreous loss and expulsive hemorrhage. The external force may be accomplished by digital pressure, a rubber ball with an elastic band around the head, or a pneumatic rubber balloon (i.e., a Honan IOP reducer). Each technique has the potential risk of optic atrophy or arterial occlusion from the excessive or prolonged application of pressure, and the Honan device may be the safest in this regard by allowing monitoring of the pressure in the balloon. Although the IOP does not correlate directly or linearly with the pressure in the Honan balloon, studies suggest that it is safe in normotensive eyes, especially when the instrument is set at 30 mm Hg for 5 minutes (121). However, the induced IOP rise is a function of the initial ocular tension, and marked pressure elevations may occur in eyes with initial levels above 30 mm Hg, indicating the need for extreme caution in these cases. Use of these approaches may be unnecessary if topical or subconjunctival anesthesia is used.
Selection of Intraocular Lens
Intraocular lens implantation in the posterior chamber in association with extracapsular cataract extraction and phacoemulsification, although not devoid of potential glaucoma-related complications, is generally associated with a slight reduction in postoperative IOP and is well tolerated even in eyes with advanced preexisting glaucoma where IOP is satisfactorily controlled. Anterior chamber lenses, however, are more problematic, and preoperative glaucoma or anterior chamber angle abnormalities are relative contraindications to their use. In one study of 18 normotensive eyes with angle-supported lenses, synechiae developed around the haptics in 12 cases (94), which can lead to aqueous outflow obstruction, especially in eyes with preexisting glaucoma. In another study, anterior chamber lens implantation in eyes with preoperative peripheral anterior synechiae was associated with corneal endothelial cell loss, fibrous endothelial metaplasia, and angle cicatrization (122).
Intraoperative Considerations
Attention to gentle handling of tissues, hemostasis, and minimal intraocular manipulation may reduce the risk of postoperative IOP rise associated with hemorrhage or excessive inflammation or pigment dispersion. One study found that the technique of wound closure (specifically, a sutureless sclerocorneal tunnel incision) and the surgeon’s experience were more important than prophylactic medications in preventing IOP elevation after phacoemulsification (123). Judicious use of intraocular agents such as viscoelastic substances and thorough irrigation to remove the material at the end of the case, especially in eyes with preexisting glaucoma, may help to minimize the risk of postoperative glaucoma complications.
The miotic agents, acetylcholine and carbachol, are often injected into the eye during cataract surgery to constrict the pupil, especially after implantation of a posterior chamber intraocular lens. Use of acetylcholine, compared with balanced salt solution, was associated with lower IOPs at 3 and 6 hours postoperatively but was not statistically significantly different at 24 hours (124). Use of the combination of preoperative acetazolamide and intraoperative acetylcholine was more effective than either drug alone in controlling postoperative IOP elevation (125). Carbachol was associated with lower postoperative pressures, compared with acetylcholine or balanced salt solution, at 24 hours, 2 days, and 3 days postoperatively (126). The intracameral use of carbachol therefore may be helpful in avoiding early IOP rises, especially in eyes with preexisting glaucoma.
Early Postoperative Period
The IOP can rise a few hours after routine cataract extraction but generally returns to normal within 1 to 3 days. A modest pressure rise (e.g., <30 mm Hg) in a nonglaucomatous eye with a deep anterior chamber is usually of no consequence and requires no antiglaucoma therapy. However, high pressures may cause pain and occasional disruption of the corneoscleral wound. Eyes with preexisting glaucoma and advanced glaucomatous optic atrophy may have further nerve damage with even short episodes of pressure elevation. Anterior ischemic optic neuropathy has occurred during these periods of elevated pressure in eyes with vulnerable optic nerve head circulation (127). If there is pain or a threat to the optic nerve head, cornea, or cataract incision, temporary medical measures should be used.
Several drugs have been evaluated for their efficacy in controlling the early IOP rise in eyes with open anterior chamber angles. Although the results from various studies are somewhat conflicting, a randomized trial showed that topical brinzolamide, brimonidine, 0.2%, timolol, 0.5%, intracameral acetylcholine, and acetazolamide, 250 mg, administered immediately after cataract surgery were more effective than use of no ocular hypotensive medication at reducing the IOP at 6 hours and 20 to 24 hours after surgery (128). Another randomized trial comparing various antiglaucoma drops found that use of a combination of timolol, 0.5%, and dorzolamide, 2%, produced the greatest IOP reduction in the first 24 hours after phacoemulsification cataract surgery (129). Steroids were ineffective in one study (130), but they may help control the pressure when inflammation is excessive. Indomethacin and aspirin have also reduced the postoperative pressure rise (131), presumably by inhibiting prostaglandin synthesis. When uveitis and glaucoma are associated with retained lens fragments in the vitreous, pars plana vitrectomy is reported to yield good results (71).
Uveitis, glaucoma, and hyphema may be managed by using mydriatic agents to minimize iris movement against the lens in mild cases. In more severe cases, steroids should be used for the iritis, and a carbonic anhydrase inhibitor or topical β-blocker or α2-agonist for the glaucoma. Argon laser photocoagulation may be effective in controlling the hemorrhage in the rare cases in which the bleeding site is visible (132). Recurrent hyphema and glaucoma is usually an indication to remove the lens implant, although this is often difficult and can lead to serious intraoperative complications. When glaucoma and hyphema are associated with vitreous hemorrhage, pars plana vitrectomy has been recommended (133). Pigment dispersion in pseudophakia can usually be controlled medically and gradually becomes easier to manage in most cases; removal of the lens implant is rarely required.
Pupillary block in aphakia may initially be treated with mydriasis to break the block, although an iridotomy is usually required. To be effective, the iridotomy must be placed over a pocket of aqueous behind the iris, rather than an area in which the vitreous is in broad apposition to the posterior surface of the iris. The laser is particularly useful in these cases, because more than one iridotomy can be made until an aqueous pocket is found as evidenced by a deepening of the peripheral anterior chamber. Suggested alternative surgical approaches include separating the iris from the vitreous adhesions with laser iridoplasty, an iris repositor, or pars plana vitrectomy.
Pupillary block in pseudophakia may be broken with mydriatic therapy by enlarging the pupil beyond the edges of an anterior chamber lens or by lysing posterior synechiae from a posterior chamber lens. Use of one or more of the following agents may also be required as an emergency measure: carbonic anhydrase inhibitor, hyperosmotic agent, β-blocker, α2-agonist. The definitive treatment is an iridotomy, which is best achieved with a laser as soon as possible. The laser may also be used to break the block by dilating the pupil (134). Closed vitrectomy has also been used to relieve pseudophakic pupillary block (135).
Late Postoperative Period
Most patients with chronic glaucoma in aphakia or pseudophakia can and should be managed medically. This is usually done with the use of drugs that reduce aqueous production, such as carbonic anhydrase inhibitors, β-blockers, and α2-agonists, although miotic therapy can also be effective. Surgical intervention is reserved for cases that are uncontrolled on maximum tolerable medical therapy. Laser trabeculoplasty may be effective in cases that do not have extensive peripheral anterior synechiae and is the initial surgical procedure of choice (136). When strict IOP and visual acuity criteria were used to define success in one study, no surgical procedure was highly effective for chronic glaucoma in aphakia or pseudophakia (137). In one series of trabeculectomies in 82 aphakic eyes, fewer than half were successful (138). Other surgeons, however, have had somewhat better results and feel that trabeculectomy with antimetabolite is the procedure of choice if trabeculoplasty fails or is not possible (136). When conjunctival scarring does not allow performance of a trabeculectomy in a superior quadrant, implantation of a glaucoma drainage device is usually indicated. Transscleral cyclophotocoagulation can also be attempted (see Chapter 41), although it should usually be reserved for patients with poor visual potential or in whom incisional surgery is not possible or thought to have a poor chance of success.
When Nd:YAG capsulotomy is required in the late postoperative period, apraclonidine (1.0% or 0.5%), timolol, or acetazolamide given 1 hour before or immediately after the procedure, or both, effectively minimizes the postlaser pressure rise.
GLAUCOMAS ASSOCIATED WITH EPITHELIAL INGROWTH AND OTHER CELLULAR PROLIFERATIONS
A group of rare but potentially devastating conditions may complicate cataract surgery, incisional glaucoma procedures, or any other incisional operation, and some forms of trauma. These conditions have as their common denominator a proliferation of cells into the anterior chamber.
Epithelial Ingrowth
Clinical Features
With this condition, also referred to as epithelial downgrowth, an epithelial membrane grows into the eye through a penetrating wound. It extends over the posterior surface of the cornea, causing corneal edema, and grows down across the anterior chamber angle and onto the iris, which may lead to a refractory form of glaucoma. It occurs in 0.09% to 0.12% of eyes after cataract surgery (139–142). The incidence appears to be declining with newer cataract techniques, although a case has been reported with a sutureless scleral tunnel incision (142). It may also occur after penetrating trauma, penetrating keratoplasty, and glaucoma surgery (143–145).
Early in the disease process, a wound leak may be present. By slitlamp biomicroscopy, the epithelial ingrowth on the cornea is seen as a thin gray translucent or transparent membrane with a scalloped, thickened leading edge (Fig. 26.10A). Specular microscopy may reveal a characteristic pattern of cell borders, which may have some diagnostic value (142). Fluorophotometry has also been reported to have diagnostic value by showing a delayed disappearance of the topically applied fluorescein in the area overlying the membrane (142). The membrane on the iris is more difficult to see, but it typically causes a flattening of the stroma and can be delineated by the characteristic white burns that result from diagnostic application of argon laser photocoagulation (Fig. 26.10B) (146). In one case with a penetrating foreign body, the membrane had a gelatinous appearance, which by histology revealed goblet cells and mucinous material (143). Gonioscopy often reveals peripheral anterior synechiae. Cytologic evaluation of an aqueous aspirate has been described as a diagnostic aid (147), although the clinical features are usually sufficient to establish the diagnosis.

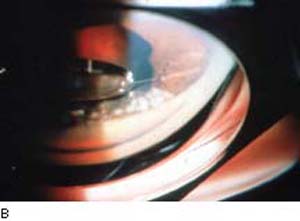
Figure 26.10 Epithelial downgrowth. A: Clinical appearance of epithelial downgrowth. Note advancing epithelial line located on the corneal endothelium. B: Gonioscopic image of white, coagulated areas of epithelium on the iris surface after confirmatory surface treatment with argon laser. (Courtesy of E. Hodapp, MD. From Werner MA, Grajewski AL. Glaucoma in aphakia and pseudophakia. In: Tasman W, Jaeger EA, eds. Duane’s Clinical Ophthalmology. Vol 3. Philadelphia, PA:Lippincott Williams & Wilkins; 2008:chap 54G.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


