Glaucomas Associated with Ocular Trauma
CONTUSION INJURIES
General Features
Blunt injuries involving the eye are not uncommon; fortunately, many can be prevented with the use of appropriate protective eyewear. A survey of data derived from hospital discharge abstracts in the United States between 1984 and 1987 revealed a rate of 13.2 cases per 100,000 for any ocular trauma as a principal diagnosis, of which approximately 40% were coded as contusion of the eyeball or adnexa or orbital blowout fracture (1). Young men appear to be most prone to such trauma. In a series of 205 patients with ocular contusion injuries, 85% were males and 75% were younger than 30 years (2). Sporting and domestic accidents accounted for almost two thirds of these injuries, with the remaining known causes divided between unintentional industrial injuries and malicious acts. Among 32 patients hospitalized for sport-related ocular contusion, ball games were the most common cause (3). Boxing is an especially high-risk sport for ocular trauma; in one series of 74 asymptomatic boxers, 66% of the men evaluated had one or more ocular injury (4). An increasingly common source of severe ocular trauma is air bag inflation in a motor vehicle accident (5).
Data from the U.S. Eye Injury Registry on 6021 patients with blunt ocular contusion suggest that the 6-month incidence of posttraumatic glaucoma is 3.4% (6). The same study identified several independently predictive factors associated with the development of posttraumatic glaucoma, including poor initial visual acuity, advancing age, lens injury, angle recession, and hyphema. Another study compared 40 consecutive eyes with closed globe injury and a chronically elevated intraocular pressure (IOP) for a minimum of 3 months with 52 eyes that had closed globe injury and no evidence of glaucoma. Increased pigmentation at the angle, elevated baseline IOP, hyphema, lens displacement, and angle recession of more than 180 degrees were associated with the occurrence of chronic glaucoma after closed globe injury (7).
Clinical Findings
The anterior segment is the portion of the eye most frequently damaged by blunt trauma, and hyphema is the most common mode of clinical presentation (Fig. 25.1), occurring in 81% of the 212 eyes in one series (2). A late sign that is almost pathognomonic of hyphema is pigment clumps on the trabecular meshwork (Fig. 25.2). (The management of traumatic hyphema is discussed in Chapter 24.) As the blood clears, ruptures in various structures of the anterior segment may be found (Fig. 25.3). The most common of these is angle recession (Fig. 25.4A–C), which is seen by gonioscopy as an irregular widening of the ciliary body band. Histologically, this represents a tear between the longitudinal and circular muscles of the ciliary body. The reported prevalence of angle recession in eyes with traumatic hyphemas ranges from 60% to 94% (8–12). Angle abnormalities occurred in more than one half of the 32 patients with sports-related ocular contusions and in 19% of the 74 boxers (3,4). When gonioscopic examination was included in a population-based glaucoma survey, some degree of angle recession was found in 14.8% of the people studied, 5.5% of whom had glaucoma (13). Other associated injuries include iridodialysis, a tear in the root of the iris (Fig. 25.5), and cyclodialysis, which is a separation of the ciliary body from the scleral spur (Fig. 25.4D). Another finding associated with recurrent trauma, angle recession, and glaucoma is iridoschisis, or separation of layers of iris stroma, which is different from that seen in older adults, because it is more patchy and involves the superior and inferior quadrants (14). Patients with blunt ocular trauma may also present with iritis, cataracts, dislocation of the lens, or chorioretinal trauma.

Figure 25.1 An eye with a traumatic hyphema. Slitlamp view reveals layered blood in the anterior chamber. (Courtesy of Joseph A. Halabis, OD.)
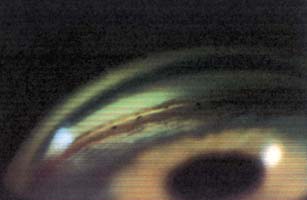
Figure 25.2 Gonioscopic view of an angle demonstrates pigment balls or clumps on the trabecular meshwork. These are virtually pathognomonic of previous traumatic hyphema.
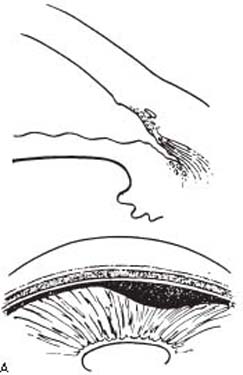

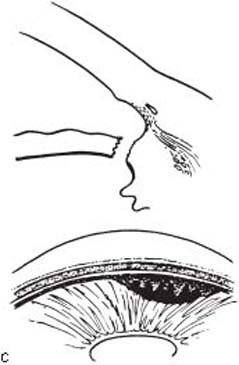
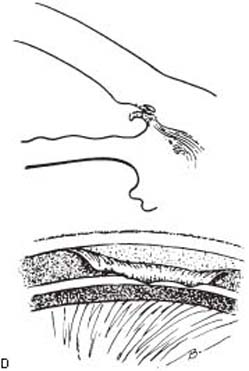
Figure 25.3 Forms of anterior chamber angle injury associated with blunt trauma, showing cross-sectional and corresponding gonioscopic appearances. A: Angle reces sion (i.e., tear between the longitudinal and circular muscles of the ciliary body). B: Cyclodialysis (i.e., separation of the ciliary body from the scleral spur, with widening of the suprachoroidal space). C: Iridodialysis (i.e., tear in the root of the iris). D: Trabecular damage (i.e., tear in the anterior portion of the meshwork, creating a flap that is hinged at the scleral spur).

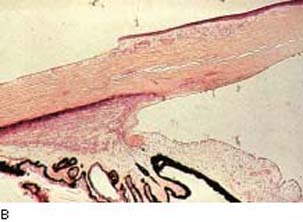


Figure 25.4 Ocular trauma to angle structures. A: Gonioscopic view of an eye with angle recession, characterized by the irregular widening of the ciliary body band and pigment clumps. (Courtesy of Joseph A. Halabis, OD.) B: Histologic section through the anterior chamber angle of an eye with angle recession shows the deep tear into the face of the ciliary body. The trabecular meshwork, which is considerably anterior to the recessed ciliary body, is partly hyalinized and is covered on its inner aspect by an abnormal proliferation of Descemet membrane, another mechanism of glaucoma associated with trauma. (Courtesy of Ramesh C. Tripathi, MD, PhD.) C: Ultrasonographic biomicroscopy shows angle recession. D: Ultrasonographic biomicroscopy reveals a cyclodialysis cleft. (From Corrêa ZM, Augsburger JJ. Ultrasound biomicroscopy of the anterior ocular segment. In: Tasman W, Jaeger EA, eds. Duane’s Foundations of Clinical Ophthalmology. Vol. 2. Philadelphia, PA: Lippincott Williams & Wilkins; 2008: chap 31.)

Figure 25.5 Gonioscopic view of an eye with iridodialysis. The ciliary processes are easily viewed through the opening in the iris. (Courtesy of Joseph A. Halabis, OD.)
Severe blunt ocular injuries can occur with air bag deployment in adults and children (5). In one report of seven children who sustained air bag injuries, serious injuries included corneal edema in one patient and traumatic hyphema with secondary glaucoma and cataract in another. Fortunately, there were no permanent visual sequelae among these children (15). The investigator, however, recommended that infants and children travel in the rear seat of automobiles to minimize their risk of injury.
Ultrasonographic biomicroscopy should be kept in mind for evaluating mechanisms of trauma (see Chapter 3). In some cases, there may be a traumatic cyclodialysis cleft or weak zonules that can be detected with relative ease by using this technology (16).
Mechanisms of Glaucoma
Early Postinjury Period
A patient with a recent blunt ocular injury may present with a slightly reduced IOP. This may result from a reduction in aqueous production due to the associated iritis or possibly a temporary increase in outflow facility because of the disruption of structures in the anterior chamber angle.
Other patients may have an elevated IOP during the early postcontusion period. In some cases, this may be a transient elevation, which lasts up to several weeks and occurs in the absence of any other obvious damage to the eye. However, there is usually an associated traumatic iritis, hyphema, or dislocation of the lens, the mechanisms of which are discussed elsewhere in this textbook (in Chapters 22, 24, and 18, respectively). Other reported mechanisms of elevated IOP associated with blunt trauma to the eye include shallowing of the anterior chamber due to uveal effusion, vitreous filling a deep anterior chamber, and Schwartz–Matsuo syndrome, which may include fluctuations in IOP in association with retinal detachment accompanied by tears of the nonpigmented epithelium of the ciliary body (17–20).
Late Postinjury Period
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


