18

23-Gauge Vitrectomy
Veronica Kon-Jara  Hugo Quiroz-Mercado
Hugo Quiroz-Mercado  Fabio Patelli
Fabio Patelli  Kirk H. Packo
Kirk H. Packo
After introduction by Fujii et al. (1) of 25-gauge vitreoretinal surgical advances in recent years, Eckardt et al. (2) had shown that transconjunctival sutureless vitrectomy with 23 gauge is a newer, safer, and more effective procedure developed to improve on the reported shortcomings of 25-gauge vitrectomy vis-à-vis conventional 20-gauge vitrectomy, such as too high flexibility and poorer efficiency of the instruments as well as the associated occasional early postoperative ocular hypotony.
Tornambe considered that 23 gauge is “the Goldilocks gauge: not too big, not too small, just right” (3).
As a minimally invasive surgery, three microcannulas are inserted transconjunctivally in pars plana and after their removal from the scleral incisions, the tunnel-like wounds are so small that they self-seal; there is no surgical trauma to the conjunctiva and fewer changes in corneal topography, and rehabilitation time required is less than usual (4).
Although almost all kinds of vitreoretinal surgery can be done with 23 gauge, there are some cases in which retinal surgeons still prefer 20 gauge, such as for severe proliferative vitreoretinopathy, severe tractional diabetic retinal detachment, trauma, intraocular foreign body, or lens fragmentation (5).
INSTRUMENTATION
Currently, a complete stock of vitreoretinal instruments (disposable or autoclavable) is available to perform 23-gauge surgery, that includes:
 Microcannulas. They have a length of 4 mm (infusion cannula) or 4.5 mm (instruments cannula), with an internal diameter of 0.65 mm and external diameter of 0.75 mm. They are made of metal (steel) vs polyamide (Fig. 18-1).
Microcannulas. They have a length of 4 mm (infusion cannula) or 4.5 mm (instruments cannula), with an internal diameter of 0.65 mm and external diameter of 0.75 mm. They are made of metal (steel) vs polyamide (Fig. 18-1).
 Cannula forceps. They are designed for insertion and removal of cannula system (Fig. 18-2).
Cannula forceps. They are designed for insertion and removal of cannula system (Fig. 18-2).
 Cannula infusion line. Infusion lines are designed to fit all microcannulas. DORC (Zuidland, Holland) has a cannula with a valve that controls or prevents the loss of intraocular fluid.
Cannula infusion line. Infusion lines are designed to fit all microcannulas. DORC (Zuidland, Holland) has a cannula with a valve that controls or prevents the loss of intraocular fluid.
 Vitrectome. Two options available are:
Vitrectome. Two options available are:
Pneumatic vitrectome. Increased stiffness and optimized flow with 2500 cuts per minute, the 23-gauge vitreous cutter is a little bit slower than a 20-gauge cutter, but their slight flexibility is useful to performing difficult tasks in peripheral retina. The port of the 23-gauge vitrectome is 30% larger than 25 gauge and 50% closer to tip than 20 and 25 gauge. This is helpful to control and peeling membranes where close shaving is required (6) (Fig. 18-3).
Electromagnetic vitreous cutter.

Figure 18-1. Microcannula.
 Endoillumination probe. Three types of illumination:
Endoillumination probe. Three types of illumination:
Standard. They have a typical triple-port connector.
Wide angle (Total view). Adjustable fiber/light intensity, triple-port connector with a spatula pic tip and combined endoillumination tip (standard and total view) are available.
Spaide Total view. Combine direct (focused) and diffuse wide field illumination.
 Chandelier light. These are available for broad illumination of the fundus.
Chandelier light. These are available for broad illumination of the fundus.
 Backflush needle. A blunt needle is used for passive aspiration.
Backflush needle. A blunt needle is used for passive aspiration.
 Brush backflush needle. A brush needle is used for active aspiration.
Brush backflush needle. A brush needle is used for active aspiration.
 Plugs. They are made with titanium or steel.
Plugs. They are made with titanium or steel.
 Intraocular scissors. The radius of curvature for intraocular scissors is wider for 23-gauge scissors than 20-gauge scissors because bore size of the microcannula (3).
Intraocular scissors. The radius of curvature for intraocular scissors is wider for 23-gauge scissors than 20-gauge scissors because bore size of the microcannula (3).
Curved scissors. Sharp tipped scissors with a radius of curvature of 12 mm allows one to follow the contour of the retina for cutting membranes adherent to the retinal surface.
Straight scissors.
Vertical scissors.
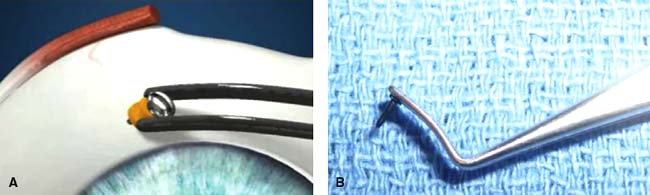
Figure 18-2. Cannula forceps are designed to easily grip and manipulate the microcannulas.
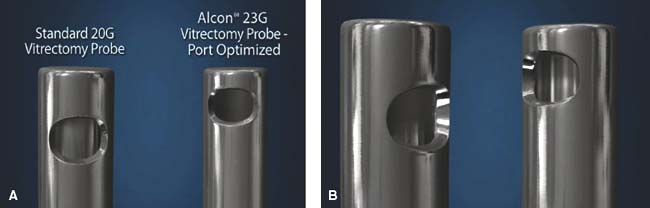
Figure 18-3. Pneumatic Vitrectome (Vitreous cutter).
 Forceps
Forceps
End-gripping. Multifunctional forceps is useful for internal limiting membrane (ILM) peeling and other macularhexis procedures. The tip is the same length as 20-gauge instrument.
Serrated jaws.
ILM forceps. Specially created for peeling of ILM in macular surgery, with smaller tips which facilitate the peeling (Fig. 18-4).
 Membrane pic. This pic is angled at 100 degrees with a sharp point. Vitreoretinal surgeons use pics to raise and dissect epiretinal membranes.
Membrane pic. This pic is angled at 100 degrees with a sharp point. Vitreoretinal surgeons use pics to raise and dissect epiretinal membranes.
 Endolaser Probe.
Endolaser Probe.
 Tano scraper. (Fig. 18-5)
Tano scraper. (Fig. 18-5)
 Endodiathermy Probe.
Endodiathermy Probe.
 Microvitreoretinal (MVR) blade. The MVR blade is angled at 45 degrees with a width: 0.72 mm.
Microvitreoretinal (MVR) blade. The MVR blade is angled at 45 degrees with a width: 0.72 mm.
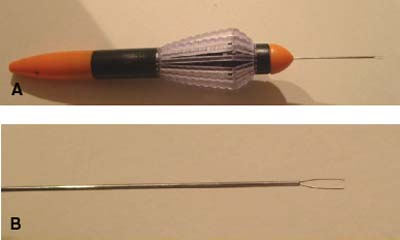
Figure 18-4. Internal limiting membrane forceps.
 Pressure plate. This is used to fixate the conjunctiva at the sclera during incision and insertion technique. A 1 mm diameter opening at the center of the plate ends laterally in a slit. The outer edge of the plate’s underside is equipped with small teeth to prevent slippage. The pressure plate performs three functions. First, it is used to press the conjunctiva firmly against the sclera to prevent it from moving as the scleral tunnel incision is made and following insertion of the microcannulas. This facilitates subsequent identification of the conjunctival and scleral incisions. Second, it is used to move the globe during the sclerotomy. Third, it aids in measuring the distance between the sclerotomy and the corneoscleral limbus. Placed directly on the corneoscleral limbus, the distance to the middle of the central opening in the plate is 3.5 mm.
Pressure plate. This is used to fixate the conjunctiva at the sclera during incision and insertion technique. A 1 mm diameter opening at the center of the plate ends laterally in a slit. The outer edge of the plate’s underside is equipped with small teeth to prevent slippage. The pressure plate performs three functions. First, it is used to press the conjunctiva firmly against the sclera to prevent it from moving as the scleral tunnel incision is made and following insertion of the microcannulas. This facilitates subsequent identification of the conjunctival and scleral incisions. Second, it is used to move the globe during the sclerotomy. Third, it aids in measuring the distance between the sclerotomy and the corneoscleral limbus. Placed directly on the corneoscleral limbus, the distance to the middle of the central opening in the plate is 3.5 mm.
 Hem-stopper.
Hem-stopper.
 Flute needle.
Flute needle.
 RON-knife.
RON-knife.
These 23-gauge instruments are very similar in design and utility to standard 20-gauge instruments.
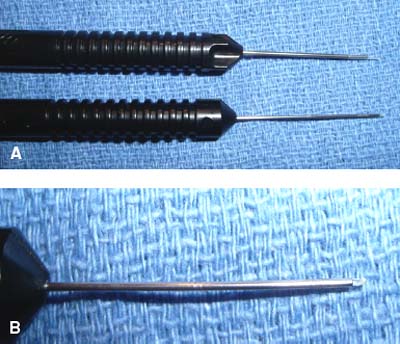
Figure 18-5. A. Tano scraper (20 gauge (top); 23 gauge (bottom). B. Note the diamond dusted silicone tip.
ADVANTAGES OF 23-GAUGE VITRECTOMY OVER 20- AND 25-GAUGE VITRECTOMY
 Flexibility. 23-gauge vitrectomy instruments are not as flexible as 25 gauge and maintain sturdiness similar to 20 gauge allowing one to perform complicated maneuvers in vitreous cavity and eye rotation.
Flexibility. 23-gauge vitrectomy instruments are not as flexible as 25 gauge and maintain sturdiness similar to 20 gauge allowing one to perform complicated maneuvers in vitreous cavity and eye rotation.
 Illumination. Illumination with 23-gauge vitrectomy is better than 20-gauge vitrectomy with uniform dispersion and a 78-degree angle of illumination.
Illumination. Illumination with 23-gauge vitrectomy is better than 20-gauge vitrectomy with uniform dispersion and a 78-degree angle of illumination.
 Lumen. It is well known that the standard wall thickness between 23 and 25 gauge is the same, but their difference is a wider inner diameter in 23 gauge which provides better flow and probably more stiffness. 23 gauge is narrower than 20 gauge with adequate fluidics during surgery and flow rates similar to 20 gauge.
Lumen. It is well known that the standard wall thickness between 23 and 25 gauge is the same, but their difference is a wider inner diameter in 23 gauge which provides better flow and probably more stiffness. 23 gauge is narrower than 20 gauge with adequate fluidics during surgery and flow rates similar to 20 gauge.
 Difficult cases. Many surgeons advocate that 23 gauge could manage a broad case selection, including difficult cases of rhegmatogenous retinal detachment or proliferative diabetic retinopathy with tractional retinal detachment.
Difficult cases. Many surgeons advocate that 23 gauge could manage a broad case selection, including difficult cases of rhegmatogenous retinal detachment or proliferative diabetic retinopathy with tractional retinal detachment.
 Sutureless. Patients feel excellent because their rehabilitation and comfort improve, and there is no residual astigmatism (4).
Sutureless. Patients feel excellent because their rehabilitation and comfort improve, and there is no residual astigmatism (4).
 Scleral closure. With newer microcannula insertion technique (angled entry), there is less hypotony than had been seen in 23-gauge cases.
Scleral closure. With newer microcannula insertion technique (angled entry), there is less hypotony than had been seen in 23-gauge cases.
 Learning curve. It is faster in transition between 20 to 23 gauge.
Learning curve. It is faster in transition between 20 to 23 gauge.
 Recovery. Faster recovery could be related to less ocular surface inflammation.
Recovery. Faster recovery could be related to less ocular surface inflammation.
INCISION TECHNIQUE WITH 23-GAUGE VITRECTOMY SYSTEM
The first step to getting a clean and comfortable incision site is holding the eye firmly with a special pressure plate (Dutch Ophthalmic Research Center [DORC], Zuidland, Holland), a Thornton ring, or cotton tipped applicator; and pushing the conjunctiva laterally 1 or 2 mm (Fig. 18-6).
One can choose between two different systems to insert the microcannulas. At the initial description of the procedure (two-step entry), a 23-gauge stiletto blade was inserted at an angle of 30 to 40 degrees, 3.5 mm (pseudophakic, aphakic) or 4 mm (phakic) from the corneoscleral limbus in three directions: posterior-anterior (7), anterior-posterior (8) or parallel to the corneoscleral limbus in the superonasal, superotemporal, and inferotemporal quadrants (7, 9). If the tunnel incisions ran an anterior-posterior course there was a risk that the tunnel’s interior opening could lie too close to the ora serrata; this risk could be lowered by locating the exterior opening closer to the corneoscleral limbus. Since the conjunctiva in this area can be displaced scarcely or not at all, the result would be a scleral incision lying directly under the conjunctival incision; so this possible shortcoming of a tunnel running parallel to the limbus is offset by the advantage of an anterior-posterior tunnel whose course runs parallel to the scleral fibers, requiring that the fibers need only be separated without cutting, facilitating postoperative closure of the sclerotomy (10, 11).
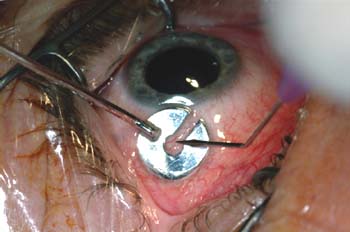
Figure 18-6. A pressure plate (DORC) is used to stabilize the eye for incision with a 23-gauge stiletto blade.
The scleral tunnel-like incisions are 0.72−0.74 mm wide and the pressure applied against them has to be constant to prevent slippage of the conjunctiva. Then the microcannulas are inserted through the conjunctiva and sclera with a special blunt inserter (DORC, Zuidland, Holland) and, subsequently, the instruments through them (2). Since the tangential position of the inserter causes the globe to rotate under pressure, pressure must be applied in the direction of the apex of the orbit. To do this, the inserter must be moved from its original tangential position to a position perpendicular to the sclera, where the resistance caused by the introduction of the microcannula can be easily overcome. Before the microcannula is inserted all the way into the sclerotomy, the pressure plate is removed. As the inserter is withdrawn from the microcannula, the cannula must be held firmly in place in the sclerotomy using a special forceps (DORC). Normally, the infusion microcannula is first placed in the inferotemporal quadrant and the adequate angle of entry allows better friction to control the cannula in place; however, there is no difference depending on whether the trocar is inserted with the bevel down or up (10) (Fig. 18-7).

Figure 18-7. Microcannulas are inserted through the conjunctiva and sclera with a special blunt inserter (DORC).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


