3 Endoscopic Equipment
The transsphenoidal midline route represents the standard approach to the pituitary and sella and is indicated for more than 95% of surgical procedures in this region. The success of the transsphenoidal route is dependent not only on its versatility as an approach to a wide variety of lesions of the sellar area but also on the following factors: (1) it is the least traumatic route to the sella; (2) it avoids any brain retraction and visible scars; (3) it provides excellent visualization of the pituitary gland and related pathology; (4) it offers a lower morbidity and mortality rate as compared with transcranial procedures; and (5) it allows a shorter hospital stay. Based on these advantages of transsphenoidal surgery in combination with the continuous search for less invasive procedures and the development of endoscopic equipment, endoscopic endonasal transsphenoidal surgery slowly and inexorably became an accepted technique in the field of pituitary surgery during the last decade of the twentieth century.1–4
As a result of renewed anatomic interest in both the endonasal approach and the anatomy of the skull base, endoscopy has been able to contribute to a better understanding and wider application of the transsphenoidal approach. This approach can be routinely used not only for all sellar lesions but also for extrasellar lesions, based on the increased visualization it affords. The endoscopic approach to the anterior skull base has motivated several anatomical studies and led to enhancements in a variety of procedures.5–9 Modifications of the standard transsphenoidal approach that allow additional exposure of the perisellar areas have been used for various skull base lesions. Extended approaches, aimed not only at the pituitary, but also at extrasellar compartments, from the frontal sinus all the way down to the craniovertebral junction, have been successfully performed to provide access to a variety of lesions affecting the entire midline skull base.10–13 Thus, endonasal approaches, once utilized for access to sellar and intra- and suprasellar subdiaphragmatic lesions only, are used today even more frequently for lesions located beyond the sella. Previously, such lesions would have been considered accessible by only transcranial approaches. An increasing number of clinical series on these extended approaches are now appearing in the literature, and guidelines for performing these techniques are being reported.10,14–19
Nevertheless, other factors have contributed to determine the success of the endoscopic skull base surgery. The fact that the operation itself has become increasingly simple, safe, and elegant is unimaginable without appropriate instrumentation.20 Every operation, and every technique for each type of operation, requires a dedicated set of instruments. Endoscopic skull base surgery, as with any other type of endoscopic surgery, requires that all the instrumentation and tools—endoscope, camera, light source, monitor, videorecording systems, drills, etc.—be of the best quality possible and be dedicated to this type of operation. The instruments form a sort of chain, where each link must be strong enough to perform its role in the operation; otherwise the chain will break and the surgery will not be successful.
 The Dedicated Operating Room
The Dedicated Operating Room
The operating room itself can be considered a surgical instrument (Fig. 3.1). An integrated operating room helps to optimize teamwork and improve patient care.10,21 In the operating room, all of the equipment, such as the cold light source, video camera, monitor, and video recording system, are placed ergonomically behind the head of the patient and in front of the operating surgeon, who is at the right side of the patient. The anesthesiologist is positioned with his or her equipment at the left side of the patient at the level of the head. The second surgeon is at the left side of the patient, and the scrub nurse is positioned at the level of the patient’s legs.
The main characteristics of this operating room are (1) compartmentalization of sterile and nonsterile activities, (2) fluidity of the workflow during the procedure, and (3) optimal access to the patient in case of emergency. The operating room control interface is user friendly, and its use creates a great sense of camaraderie among surgeons, anesthesiologists, and nurses.
Thanks to communication technology, the operating room may become a world surgical amphitheater, in that the Internet allows the real-time, two-way transmission of digital encrypted data throughout the world.
During surgical procedures the archiving system is an efficient and inexpensive mechanism for storing and analyzing neurosurgical images. All patient data collected during the operation are transmitted and stored for future reference; they are easily accessible, strictly confidential, and manipulation safe.
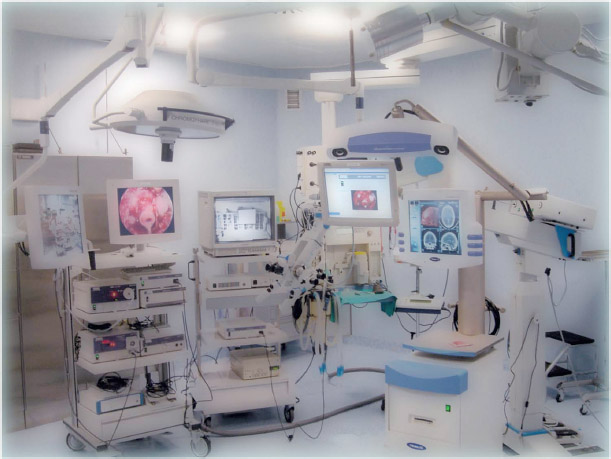
Fig. 3.1 The integrated operating room (OR1; Karl Storz, Tuttlingen, Germany) currently used at the Division of Neurosurgery of the Università degli Studi di Napoli Federico II.
 The Endoscope
The Endoscope
There could not be any endoscopic surgery without the endoscope. Such a tool permits access to deep anatomic structures in a minimally invasive manner. It enables the visualization of deep, hidden structures in the brain and transmits clear and usable images to the surgeon. It increases the precision of the surgery and permits the surgeon to differentiate tissues so that selective removal of the lesion can be achieved.20–22
In general, endoscopes are classified as either fiberoptic endoscopes (fiberscopes) or rod-lens endoscopes. Endoscopes specifically designed for neuroendoscopy can be classified into four types: (1) rigid fiberscopes, (2) rigid rod-lens endoscopes, (3) flexible endoscopes, and (4) steerable fiberscopes.20,21,23 These different endoscopes have different diameters, lengths, optical quality, and number and diameter of working channels, all of which vary with size. The choice between them should be made on the basis of the surgical indication and personal preference of the surgeon.
For endoscopic skull base surgery, the best endoscopes are rigid rodlens scopes. Their main advantage is the better quality of vision as compared with other types of scopes. They enable the surgeon to remain oriented because of the panoramic view and permit the other instruments to be inserted alongside it. Rod-lens endoscopes consist of three main parts: a mechanical shaft, glass fiber bundles for light illumination, and optics (objective, eyepiece, relay system). The angle of view of rod-lens ranges from 0 to 120 degrees, according to the objective, but an angled objective of more than 30 degrees is used only for diagnostic or visualizing purposes. The most frequently used angles are 0, 30, and 45 degrees. The 0-degree objective provides a frontal view of the surgical field and minimizes the risk of disorientation. It is used during the majority of the operation. The advantages of the 30-degree angle is that this type of endoscope, through the rotation of the lens, increases the surface area of the field of view. Moreover, visualization of the instruments is improved as they converge toward the center of image, whereas with the 0-degree objective the instruments remain in the periphery of the image.
The endoscope is used through a sheath, which is connected to a cleaning system. The irrigation system permits cleaning and defogging of the distal lens, thus avoiding the repeated insertion and removal of the endoscope from the nostril. The endoscopes used for endonasal surgery are without any working channel (diagnostic endoscopes), and the other instruments are inserted into the same nostril, slid alongside the sheath, or inserted into the contralateral nostril. The diameter of rod-lens endoscopes varies between 1.9 and 10 mm, but for endonasal surgery usually only endoscopes with a diameter of 4 mm are used (Fig. 3.2). In selected patients with narrow nostrils and in children, a 2.7-mm endoscope can be used. The endoscope in skull base surgery can be used free-hand or fixed to a scope holder. During the first step of the operation (the approach itself), it is better to use the endoscope free-hand, so that the surgeon can dynamically handle the various instruments while creating the working space for the further steps of the procedure. The endoscope can then either continue to be used free-hand or be fixed to a scope holder. For the free-hand technique, the scope is used in a dynamic fashion and the surgeon continuously receives feedback about the anatomy and depth of the operative field based on the in-and-out movements of the scope. If a scope holder is used, a variety of systems exist. Variables include a steerable or extendable arm and a rigid or jointed arm that can be straight, curved, or pneumatic. With such devices, the endoscope is fixed in a particular position, and the surgeon can use both hands to manipulate the surgical instrumentation. Another possibility is to have the endoscope held by an assistant. With this method the dynamic movements of the scope are preserved and, at the same time, the surgeon can simultaneously use two instruments either in the same nostril or in both nostrils.

Fig. 3.2 Rigid rod-lens 4-mm endoscope without working channels used during the endoscopic endonasal transsphenoidal surgery. The length of the endoscope is 18 or 30 cm (Karl Storz, Tuttlingen, Germany).
 The Video Camera and Monitor
The Video Camera and Monitor
Although the surgeon can theoretically look directly into the ocular lens (proximal lens) of the endoscope, the operation cannot be easily and safely performed in this manner.24 In fact, if the surgeon had to remain in a fixed position, surgical movements would be impaired. To properly maneuver the instruments under fine control, the endoscope is connected to a dedicated video camera, and the endoscopic images are projected onto a monitor placed in front of the surgeon. Additional monitors can be placed in varying locations in the operating room, as well as outside in the hallways or adjacent rooms, to permit other members of the team to watch the surgery.
Several types of endoscopic video cameras are available, the most common of which utilize a 3-CCD (charge-coupled device) sensor. Although the 1-CCD cameras process all three fundamental colors in one chip, the 3-CCD ones have a separate chip for each color (red, green, blue; RGB) and provide better color separation, more brilliant colors, and a sharper image with higher contrast.25 Buttons located on the camera control the focus and the zoom. Optical zoom is preferable because it enlarges the image using the same number of pixels, whereas the electronic zoom increases the size of each pixel, which degrades the definition of the image. Most modern endoscopic cameras are analogue. This means that the signal is transmitted to a central processing unit, which outputs the signals in RGB, Svideo, or Composite video formats. Digital 3-CCD endoscope cameras are available, which produce the highest quality images that can be directly connected to video recorders for highquality video reproduction.
The images produced by the endoscope camera are displayed on one or more monitors. These need to have a highresolution screen to support the signal quality arising from the camera. The monitors most commonly used in endoscopic surgery have a minimum horizontal resolution of 750 lines, to visualize all the details of the endoscopic images.
A further improvement of the resolution of both the video cameras and the monitors is represented by the high-definition television technology, which is ready for the future threedimensional (3D) endoscopes. As a matter of fact, the continuous improvements in endoscopic image quality offer excellent visualization of the operative field, of the lesion, and of its relationships with the surrounding anatomical structures. A full high-definition (HD) 16:9 flat monitor (1080p60) (Fig. 3.3A) needs to be coupled with the HD camera (Fig. 3.3B) to visualize the HD images.
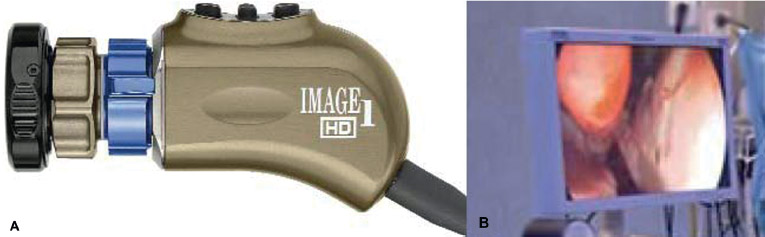
Fig. 3.3 (A) HD camera. (B) Full high-definition (HD) 16:9 flat monitor (1080p60). (Karl Storz, Tuttlingen, Germany).
 The Light Source
The Light Source
The endoscope transmits cold light, which arises from a source inside the surgical field through a connecting cable made of glass fibers. Currently in endoscopic surgery, xenon light sources are used that have spectral characteristics similar to sunlight, with a color temperature of approximately 6000 kelvin (K), which is “whiter” than the classic halogen light (3400 K).22
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


