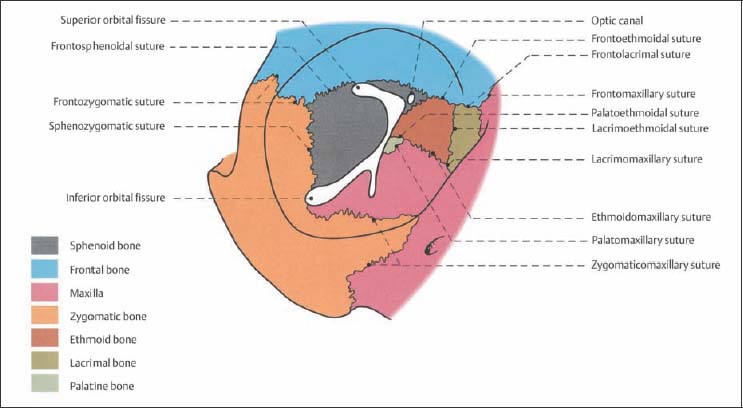
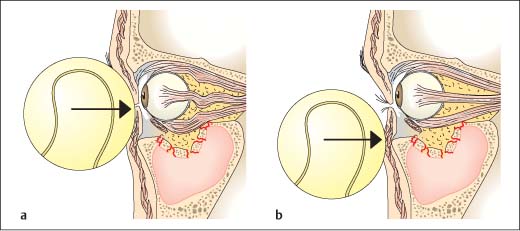
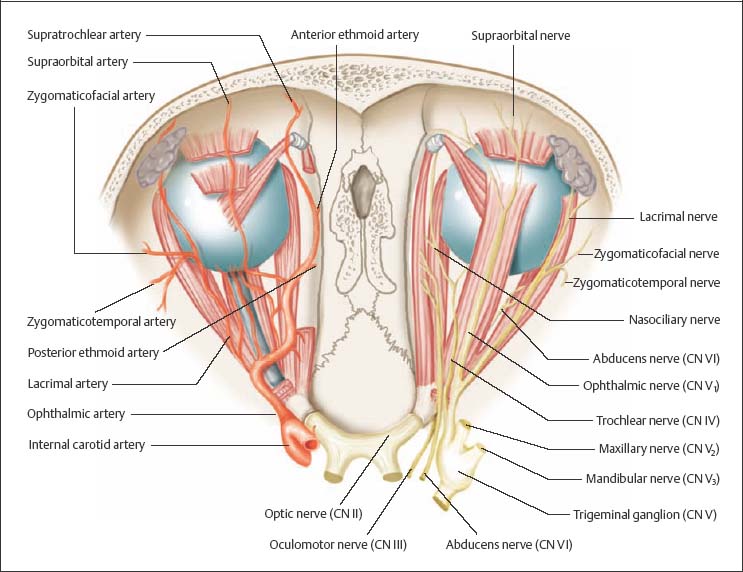
10 Diagnosing Injuries of the Orbit The structure of the orbit resembles an irregular quadrilateral pyramid (Fig. 10.1): – The orbital roof is formed by the frontal bone; – the orbital floor is made up of the zygoma and maxilla; – the posterior portion is formed by the palatine; – the medial wall by the lacrimal bone and orbital plate (lamina papyracea) of the ethmoid; – the lateral border is formed by the zygomatic bone and the greater wing of sphenoid bone; – the apex of the pyramid forms the inferior orbital fissure, which is continuous with the infraorbital canal, opening at the infraorbital foramen. The extraocular muscles arise from the common tendinous ring at the orbital apex. The common tendinous ring surrounds the optic canal and divides the orbital fissures into two components (Fig. 10.2): – abducens nerve (medial rectus muscle); – oculomotor nerve (supplies the other straight ocular muscles, inferior oblique muscle, and levator palpebrae muscle); – nasociliary nerve; – sympathetic and parasympathetic fibers to the lacrimal duct. The following nerves course outside of the tendinous ring, in the superior orbital fissure: Fig. 10.1 Anatomy of the bony orbit; osseous components (in color) and sutures (from Tillmann 1997). Fig. 10.2 Illustration of interorbital nerves, vessels, and muscles. The medial rectus muscle arises from the greater wing of the sphenoid bone. The tendon of the superior oblique muscle redirects to lateral in the trochlea, which attaches to the periosteum of the superior lateral orbital rim. The levator palpebrae muscle has its origin on the dural sheath of the optic nerve and extends to the tarsus and orbicularis oculi muscle. The ophthalmic artery, usually a branch of the internal carotid artery, lies to inferior, lateral to the optic nerve. The ophthalmic artery branches off into the anterior and posterior ethmoid arteries. In rare cases it originates at the middle meningeal artery (maxillary artery). The optic nerve is the first cranial nerve and courses in three segments: – intracranial; – intracanalicular; – orbital. Within the orbits, the optic nerve is enclosed in pia mater, arachnoid membrane, and dura mater. Osseous injuries of the orbits can be grouped into: Orbital floor fractures (blow-out and blow-in fractures) involve injury of the lamellar bone between the orbit and maxillary sinus. Orbital contents may prolapse to varying degrees into the maxillary sinus. In injury to the medial orbital wall, orbital tissue prolapses into the ethmoid cells. Both forms of injury can involve displacement of bone splinters into the orbits, impairing muscle function. Fractures of the orbital floor and medial orbital wall can result directly from a striking or crushing blow to the orbit or as an associated injury in extensive midface injury. Two pathomechanisms have been suggested in the etiology of these fractures: Patients usually present with a “monocle” hematoma, complaints of double vision, and dysesthesia in the lid and cheek area, and often in the entire distribution area of the infraorbital nerve. Fractures are generally not directly palpable. Injury may cause entrapment of the inferior rectus muscle in the orbital floor or the medial rectus muscle in the lateral orbital wall (“trap door” mechanism). Bone splinters can penetrate the ocular muscles. During clinical examination the patient reports double vision with an upward gaze (vertical diplopia; orbital floor fracture) or lateral gaze (horizontal diplopia; medial orbital wall fracture). Combinations of both patterns of injury are common (see Fig. 9.17a, Chapter 9, p. 84). Clinical examination should include asking the patient to follow the examiner’s finger with his eyes (finger perimetry) (see Fig. 2.2, Chapter 2, p. 13), as it traces a square in the air. In rare cases the globe may retract (retraction phenomenon, Duane retraction syndrome) during ocular movement. Double vision can be objectified using Kestenbaum glasses or a synoptometer. Disturbances of pupillary reflex are observed in a limited number of patients. The pupil of the affected eye is dilated while the uninvolved side retains direct and indirect light response. Fig. 10.3 Pathomechanism in orbital floor injuries (adapted from Richter 1992). a Mechanism of hydraulic force theory. b Mechanism of direct bone transmission. Exophthalmos can directly result from retrobulbar hematoma or edema in conjunction with injury. After subsidence of swelling or in the absence of hematoma and edema, the globe sinks into the widened orbital cone with enophthalmos and inferior displacement of the globe. Fractures crossing the infraorbital nerve canal can injure the nerve, causing hypesthesia in the lower lid region, maxilla, and cheek. Retrobulbar hematoma presents clinically as exophthalmus and increased intraocular pressure.
 Flowchart and Checklist Injuries of the Orbits, p. 22.
Flowchart and Checklist Injuries of the Orbits, p. 22.
 Treatment of Orbital Injuries, Chapter 20, p. 179.
Treatment of Orbital Injuries, Chapter 20, p. 179.
Surgical Anatomy
 The optic portion transmits the optic nerve and the ophthalmic artery, enclosed in dura.
The optic portion transmits the optic nerve and the ophthalmic artery, enclosed in dura.
 The neural component contains:
The neural component contains:
 trochlear nerve (supplies the superior oblique muscle);
trochlear nerve (supplies the superior oblique muscle);
 frontal nerve (providing sensation to the forehead);
frontal nerve (providing sensation to the forehead);
 lacrimal nerve (providing sensation to the lacrimal ducts).
lacrimal nerve (providing sensation to the lacrimal ducts).
Orbital Wall Fractures
 fractures of the four orbital walls;
fractures of the four orbital walls;
 injuries of the orbital apex.
injuries of the orbital apex.
Fractures of the Orbital Floor and Medial Orbital Wall
Pathomechanism
 Hydraulic force theory: orbital contents cannot escape a sudden intraorbital pressure increase, for example, caused by a blow, and thus are forced against the orbital wall, causing depression of the inferior and/or lateral orbital wall (Fig. 10.3a).
Hydraulic force theory: orbital contents cannot escape a sudden intraorbital pressure increase, for example, caused by a blow, and thus are forced against the orbital wall, causing depression of the inferior and/or lateral orbital wall (Fig. 10.3a).
 Transmission theory: traumatic force to the orbital rim is transmitted to the orbital walls, deforming them, and causing them to buckle. There is often concomitant injury of the soft tissue surrounding the orbits (Fig. 10.3b).
Transmission theory: traumatic force to the orbital rim is transmitted to the orbital walls, deforming them, and causing them to buckle. There is often concomitant injury of the soft tissue surrounding the orbits (Fig. 10.3b).
Clinical Signs and Symptoms
Diplopia
Mydriasis
 Differential diagnosis must exclude damage to the oculomotor nerve or optic nerve injury (Chapter 10, Injuries of the Orbital Apex, p. 90).
Differential diagnosis must exclude damage to the oculomotor nerve or optic nerve injury (Chapter 10, Injuries of the Orbital Apex, p. 90).
Enophthalmos/Inferior Displacement of the Eye
Sensory Disturbances
Retrobulbar Hematoma
 Retrobulbar hematomas exhibiting clinical signs (vision impairment, increased intraocular pressure) must be decompressed promptly in order to avoid lasting damage to the optic nerve.
Retrobulbar hematomas exhibiting clinical signs (vision impairment, increased intraocular pressure) must be decompressed promptly in order to avoid lasting damage to the optic nerve.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


