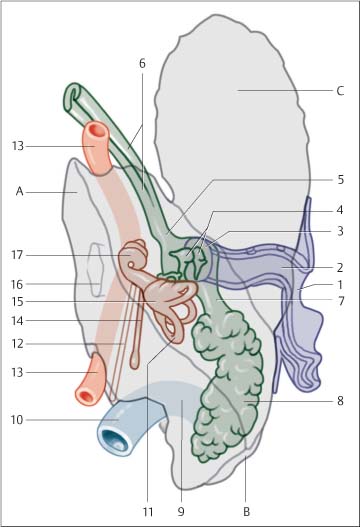
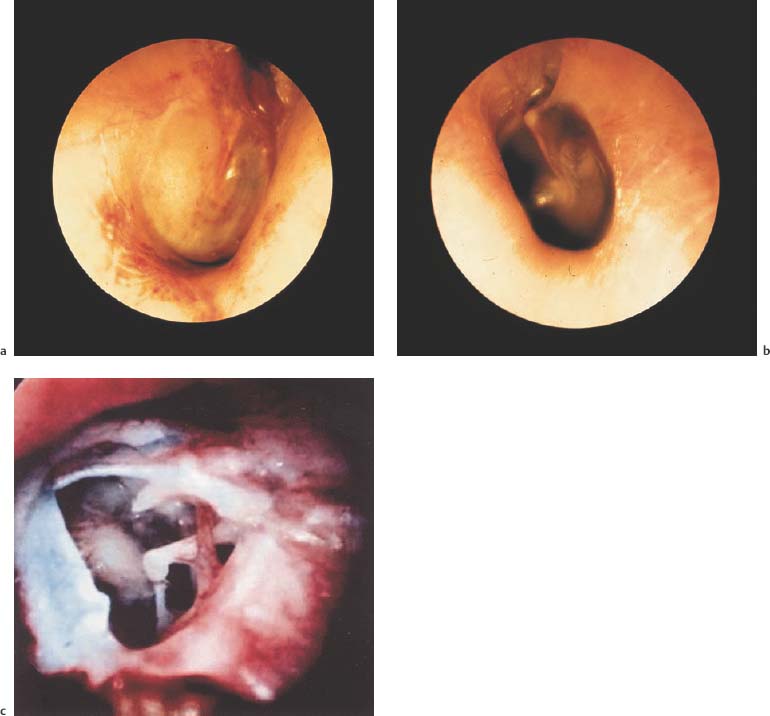
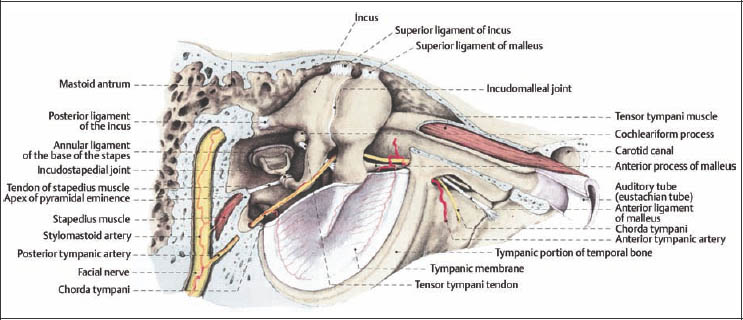
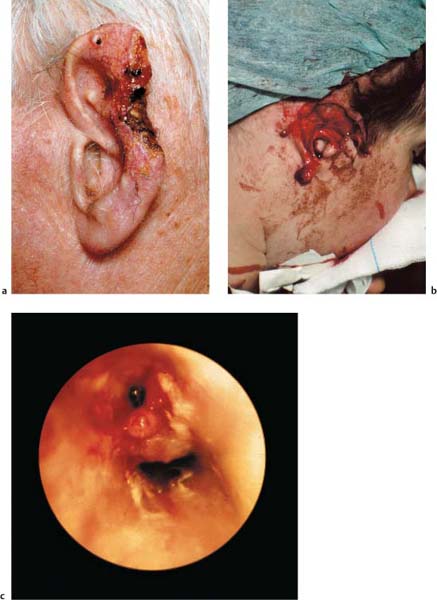
7 Diagnosing Injuries of the Ear and Lateral Skull Base The sensory organs of hearing and equilibrium (vestibulocochlear system) are enclosed within the temporal bones. The temporal bone consists of a (Fig. 7.1): The temporal line runs horizontally along the lateral aspect of the squamous portion of the temporal bone. Inferior to this line is the bony auditory canal formed by the tympanic bone; dorsal to the line is the mastoid plane with the mastoid process. Arising from the medial side of the mastoid process is the posterior belly of the digastric muscle, which serves as a type of guiding structure for the facial nerve exiting the digastric fossa. The articular fossa of the mandible lies between the root of the zygomatic arch and the anteroinferior auditory canal wall. The nerves involved in providing sensory information to the external ear are nerves V (auriculotemporal nerve), VII, X (auricular branch), IX, as well as spinal nerves C2/C3 (greater auricular nerve). The aspect of the temporal bone directed toward the brain is the petrous pyramid of the temporal bone. The pyramid divides the middle and posterior cranial fossa. The posterior surface of the sigmoid sulcus is in apposition to the pyramid and the opening to the internal acoustic meatus is directed toward the posterior cranial fossa. Temporal bone structures make up 2/3 of the floor of the middle cranial fossa. The longitudinal axis of the petrous temporal bones creates a 45 angle to the longitudinal axis of the skull, so that they form a right angle opening occipitally. The free posterior side of the pyramid between the sigmoid sinus, superior petrosal sinus, and bony labyrinth borders on Trautmann’s triangle. The sigmoid sinus runs in an S-shape through the mastoid process. Its position is influenced by the degree of pneumatization of the mastoid. Between the external ear and the labyrinth is the air-filled tympanic cavity, which is bordered by six surfaces. Opening anterior and inferior across from the antrum is the Eustachian tube (pharyngotympanic tube), which runs longitudinally to the pyramid. The tegmen tympani runs to dorsal and is continuous with the roof of the antrum, both of which form the floor of the middle cranial fossa. Fig. 7.1 Structure of the hearing organ (from Rauber/Kopsch 1987). Dark blue = external ear; brown = internal ear; green = middle ear. A Petrous (temporal) bone; B mastoid process; C temporal squama. 1 Auricle, 2 external acoustic meatus, 3 tympanic membrane, 4 auditory ossicles, 5 tympanic cavity, 6 eustachian tube, 7 mastoid antrum, 8 mastoid cells, 9 sigmoid sulcus, 10 internal jugular vein, 11 semicircular canals, 12 cochlear aqueduct, 13 internal carotid artery, 14 vestibular aqueduct, 15 vestibule, 16 internal acoustic meatus, 17 cochlea. Fig. 7.2 Structure of the middle ear (from Tillmann 1997). The dura mater, which is joined with the inner cranial periosteum, lies directly on the bone. The thickness of this dividing layer varies. In extensive pneumatization, the dura, internal carotid artery, and also the facial nerve may be covered only by connective tissue. Various forms of connecting passages have also been described through the tegmen antri and the floor of the tympanic cavity to the middle and posterior cranial fossa. On the medial wall of the tympanic cavity, which forms part of the bony capsule (osseous labyrinth), lies the promontory with the basal turn of the cochlea. Above is the oval window (longitudinal diameter ca. 4 mm). The facial nerve canal is above the oval window and further to dorsal is the ampullary end of the horizontal semicircular canal. On the posteroinferior margin of the medial wall is a bony projection, pointing toward the niche of the round window. The round window membrane itself is located rather more superiorly and has a diameter of ca. 1.3 mm. Of the three auditory ossicles—malleus, incus, and stapes—the incus is most often dislocated or fractured, the incus and stapes less often. Fracture usually involves the lenticular process protruding freely in the tympanic cavity (Fig. 7.2). The capsule of the bony labyrinth is comprised of a 2– 3-mm thick layer of bone, formed by periosteal and enchondral ossification. The capsule encloses a series of cavities comprised of the vestibule, semicircular canals (vestibular portion), and the snail-shaped cochlea (auditory portion). The membranous labyrinth is filled with endolymph, and consists of the semicircular canals, utricle, saccule, and cochlear duct. The space between the endolymph-containing labyrinth and the bony labyrinth is filled with perilymph. The subarachnoidal space and perilymph communicate via the cochlear aqueduct (perilymphatic duct). In the bony labyrinth, the vestibule is in the center, the cochlea to ventral, and the semicircular ducts to dorsal. Causes of external ear trauma include blows, penetrating wounds, or crushing force. Frostbite or chemical/thermal burn injuries are less common. The protective reflex of turning the head away from sudden danger leaves the external ear vulnerable to direct trauma. The external ear and the external auditory canal can be damaged by the following mechanisms of injury: Fig. 7.3 Injuries of the external ear and auditory canal. a Partial amputation of the external ear, which did not receive primary treatment. b Partial amputation of the upper part of the external ear. c Injury of the external auditory canal caused by a penetrating foreign body. The severity of injury depends on the extent of involvement of skin, cartilage, and muscle structures. Injuries of the tympanic membrane can arise from direct or indirect trauma: Otoscopic examination of recent injury to the ear reveals radial tears in the anterior or posteroinferior quadrants. Ruptures of the tympanic membrane without dislocation or extensive destruction tend to heal spontaneously. If perforation edges are forced into the middle ear, management with surgical splinting is necessary (Fig. 7.4). Injuries of the ossicles (injury of the ossicular chain) can be directly caused by an object or indirectly with head injury or petrous temporal bone fractures. Comprising 75 % of all injuries, incus disarticulation is the most common traumatic lesion. The second most frequent injury is isolated fracture of the crura of the stapes. Vestibular symptoms are a sign of dislocation of the stirrup in the oval window. In rare cases injury can lead to trophic damage of the lenticular process of the incus, with delayed onset of middle ear hearing impairment. Fig. 7.4 Middle ear injuries. a Visible step-off in the auditory canal in a longitudinal petrous temporal bone fracture. b Hemotympanum in a transverse petrous temporal bone fracture. c Traumatic perforation of the tympanic membrane with visible ossicles. Typical clinical signs of rupture of the round window membrane are: The mechanism of injury in ruptures of the round window membrane can be explosive or implosive; congenital or acquired defects should be also taken into consideration. Concussion or fractures of the petrous temporal bone can occur as a result of individual factors and impacting energy. Blunt cranial trauma can injure the inner ear by transmission of the pressure wave (impulse noise damage) without evidence of a fracture in lateral skull base structures. The patient usually experiences a dip in hearing ability at higher frequencies. Additional fractures or dislocations of the ossicular chain are uncommon. Hearing impairment is generally observed immediately following injury. If hearing loss is progressive, microfractures in the labyrinth capsule should be presumed (Table 7.1). Fractures of the lateral skull base are bursting basilar skull fractures. Bursting fractures occur at some distance from the site of impact and run toward the main force vector. Transverse fractures are caused by laterally directed trauma to the temporal region. Longitudinal fractures are the result of traumatic force directed to the frontal or, more often, occipital region.
 Flowchart and Checklist Injuries of the Ear and Lateral Skull Base, p. 18.
Flowchart and Checklist Injuries of the Ear and Lateral Skull Base, p. 18.
 Treatment of Injuries of the Ear, Chapter 18, p. 147.
Treatment of Injuries of the Ear, Chapter 18, p. 147.
Surgical Anatomy
 petrous portion;
petrous portion;
 tympanic portion (with middle ear components);
tympanic portion (with middle ear components);
 squamous portion.
squamous portion.
Pathomechanism and Classification
Injuries of the External Ear
 blunt trauma shearing off superficial layers of skin (seroma/hematoma of the external ear);
blunt trauma shearing off superficial layers of skin (seroma/hematoma of the external ear);
 sharp trauma with laceration or partial avulsion of the external ear (e. g., bite wounds) (Fig. 7.3a);
sharp trauma with laceration or partial avulsion of the external ear (e. g., bite wounds) (Fig. 7.3a);
 total loss of the external ear (e. g., knife wounds) (Fig. 7.3b);
total loss of the external ear (e. g., knife wounds) (Fig. 7.3b);
 thermal damage of the external ear (visual control of the skin’s surface necessary);
thermal damage of the external ear (visual control of the skin’s surface necessary);
 laceration or excoriation of the skin of the external auditory canal (Fig. 7.3c).
laceration or excoriation of the skin of the external auditory canal (Fig. 7.3c).
 Treatment of Injuries of the External Ear, Chapter 18, p. 147.
Treatment of Injuries of the External Ear, Chapter 18, p. 147.
Injuries of the Middle Ear
Injuries of the Tympanic Membrane
 Direct injury involves perforation of the tympanic membrane by a foreign object (stick, toothpick, knitting needle, cotton-tipped applicator, etc.). In welding accidents occurring overhead, molten metal can drip into the ear without injuring the skin of the auditory canal. Hot steam, tar, or oil can cause chemical or thermal burns and often leave extensive damage to the tympanic membrane.
Direct injury involves perforation of the tympanic membrane by a foreign object (stick, toothpick, knitting needle, cotton-tipped applicator, etc.). In welding accidents occurring overhead, molten metal can drip into the ear without injuring the skin of the auditory canal. Hot steam, tar, or oil can cause chemical or thermal burns and often leave extensive damage to the tympanic membrane.
 Indirect injury involves positive pressure and is caused by blasts and blows to the ear.
Indirect injury involves positive pressure and is caused by blasts and blows to the ear.
Ossicular Injuries
Rupture of the Round Window Membrane
 hearing impairment;
hearing impairment;
 nausea or vomiting with concomitant dizziness;
nausea or vomiting with concomitant dizziness;
 tinnitus.
tinnitus.
 implosive membrane rupture: transtympanic or transtubal force transmission (blast, blow to the ear).
implosive membrane rupture: transtympanic or transtubal force transmission (blast, blow to the ear).
 explosive membrane rupture: pressure increase in perilymph or cerebrospinal fluid through the cochlear aqueduct.
explosive membrane rupture: pressure increase in perilymph or cerebrospinal fluid through the cochlear aqueduct.
 traumatic deformity of the bony labyrinth can be most marked in the frame of the round window and result in fracture at this site.
traumatic deformity of the bony labyrinth can be most marked in the frame of the round window and result in fracture at this site.
 Surgical Therapy of Injuries of the Ear, Chapter 18, p. 150.
Surgical Therapy of Injuries of the Ear, Chapter 18, p. 150.
Injuries of the Petrous Temporal Bone and Labyrinth
Concussion of the Petrous Temporal Bone and Bony Labyrinth
Fractures of the Petrous Temporal Bone and Bony Labyrinth
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


