Zygomatic Arch Fractures
Zygomatic arch fractures occur from direct trauma to the side of the face. The arch is most often fractured in two or three places; the fragments are usually depressed, causing a visible flat deformity of the cheek.
38-1 Treatment of Zygomatic Arch Fractures
Indications
If a zygomatic fracture results in a cosmetic deformity or trismus, operative intervention is required. If displacement or functional deficits are not present, soft diet and observation may be used for management. Treatment should be performed following resolution of facial edema at 3–5 days.
Preoperative Evaluation
While plain film radiographs of the face can demonstrate the fracture, pediatric low-dose radiation computed tomography (CT) provides the best evaluation of the fracture and any associated injuries.
Operative Technique
1. Zygomatic arch fractures are elevated in children utilizing general nasotracheal anesthesia.
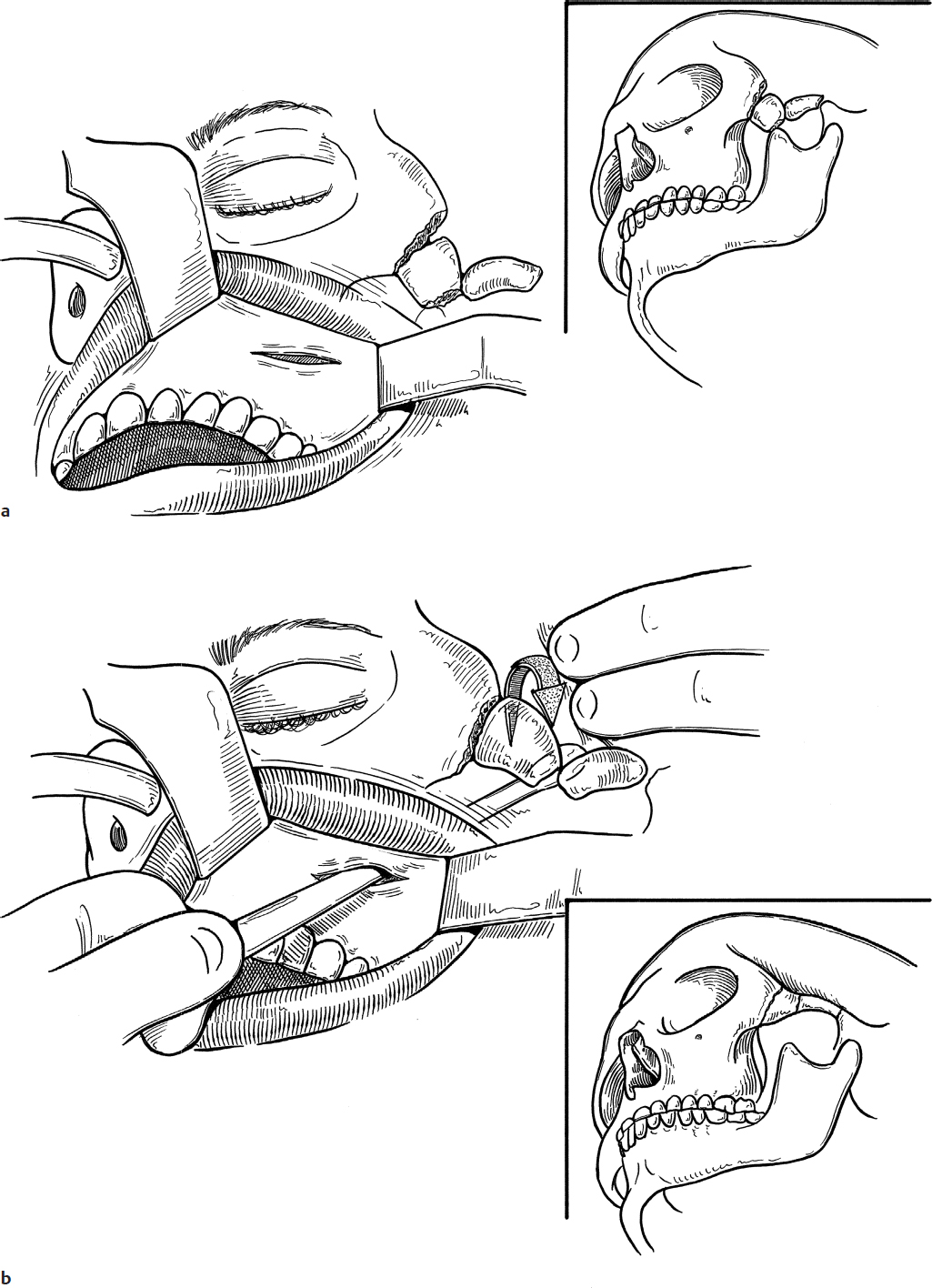
2. One percent lidocaine with 1:100,000 epinephrine is injected at the incision site to aid in hemostasis. A small incision is made in the buccal mucosa lateral to the maxilla (Fig. 38.1a).
3. An elevator or bar is inserted under the zygoma. Using the maxilla as a fulcrum, the fracture is elevated into place (Fig. 38.1b). Careful attention should be paid to avoid injury to the infraorbital nerve as it exits the maxilla.
4. No splint is needed, and two or three chromic sutures are sufficient for closure of the intraoral incision (Fig. 38.1c).
Complications
1. Insufficient reduction
2. Wound infection