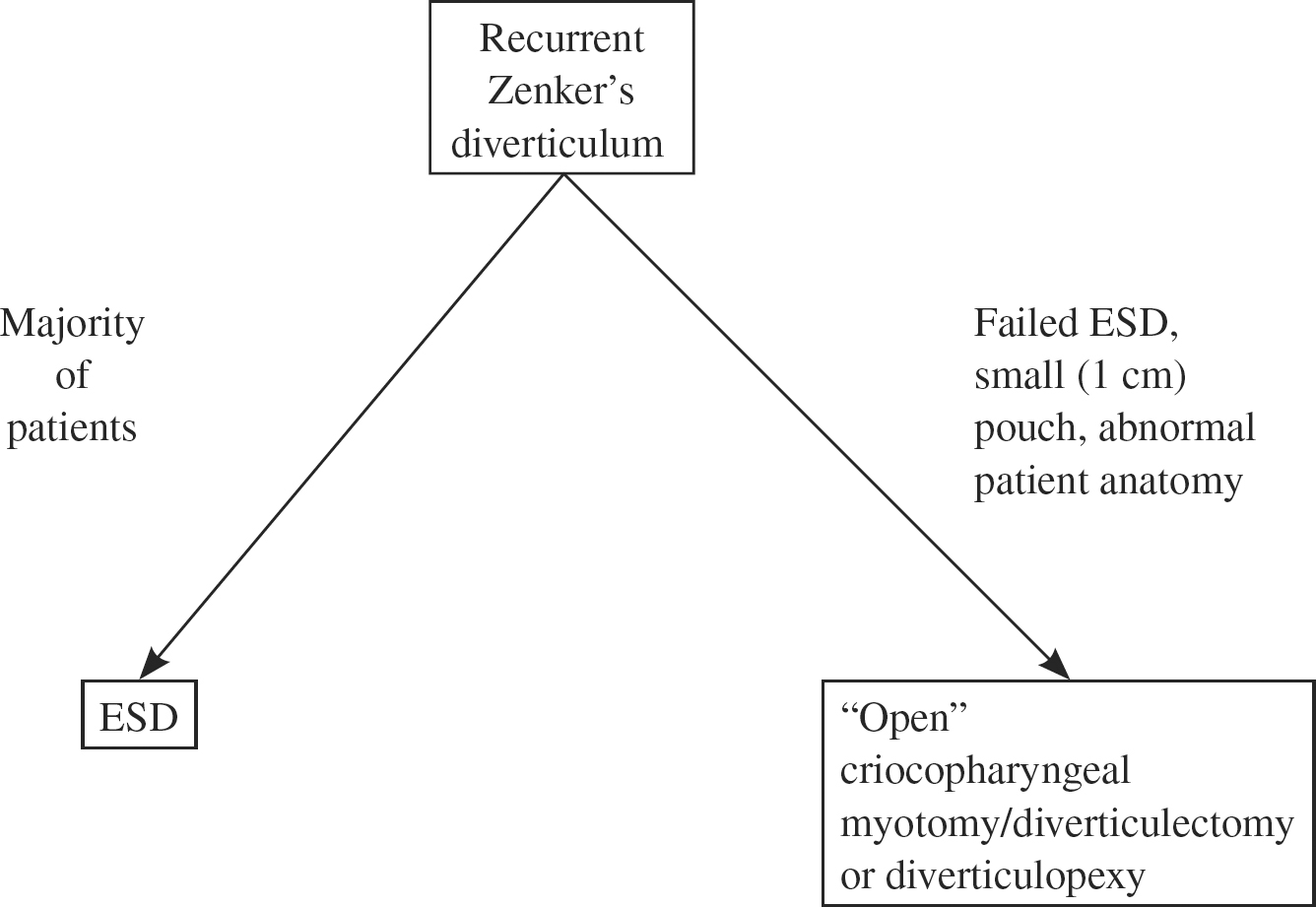
26 Zenker Diverticulum Hyphopharyngeal diverticula, to which Zenker’s name has been inextricably linked, were initially described by Ludlow in 1769.1 A clear understanding of the pathogenesis of Zenker (or Zenker’s) diverticulum (ZD) has been lacking, but most theories have focused on the structural or physiologic abnormality of the cricopharyngeal muscle and its relationship to pharyngeal and esophageal function to explain diverticular development.2 Several creative surgical approaches have been used to treat patients with ZD, including diverticulectomy,3 diverticulopexy,4,5 diverticular invagination,6,7 cricopharyngeal myotomy,8 and endoscopic diverticulotomy.9 Each of these techniques has had proponents who have reported the efficacy of their particular approach while offering evidence of low morbidity. The selection of appropriate surgical treatment has been facilitated by a clearer understanding of the pathogenesis of ZD and a continuing concern for perioperative complications in patients who are often elderly, debilitated, or have significant associated medical illnesses. Unfortunately, not as much attention has been directed to the reporting of recurrence rates following various methods of treatment for ZD, although most surgeons now advocate including some method of dealing with the cricopharyngeus muscle to produce effective relief of symptoms and minimize recurrence.8,10,11 Esophageal diverticula are classified based on anatomical location (pharyngoesophageal, midesophageal, or epiphrenic) and mechanism of formation (pulsion or traction). Of the various types of esophageal diverticula, Zenker, or pharyngoesophageal, diverticulum is the most common symptomatic esophageal form, with an annual incidence of 2 per 100,000 people per year.12 Men are affected 2 to 3 times more often than women, with peak incidence in the 7th and 8th decades of life. For those referred for an examination of the upper gastrointestinal tract, the incidence can reach as high as 1 in 1000.13,14 ZD is a pulsion-type diverticulum consisting of mucosal and submucosal membranes herniating through Killian dehiscence, an area of potential anatomical weakness located between the inferior constrictor and the cricopharyngeus muscles, first described in 1907 by Killian.15 The predominant symptom in patients with ZD is dysphagia. Other symptoms include regurgitation of food, belching, noisy deglutition, halitosis, choking, coughing, hoarseness, globus sensation, weight loss, aspiration, and pneumonia. There are often few physical findings, but these may include emaciation and only rarely Boyce sign, a swelling in the neck that gurgles on palpation.16 In those patients who have been treated for ZD, persistent or recurrent symptoms are usually similar in type to the symptoms seen before surgery, but the degree of severity may differ. Careful attention should be directed to the historical features of the patient’s complaints to ascertain whether the symptoms are similar to and as severe as those present before treatment. Other causes for the symptoms, such as gastroesophageal reflux, esophageal dysmotility, hiatal hernia, neuromuscular dysfunction, and xerostomia, not uncommonly seen in conjunction with ZD, should be kept in mind, evaluated, and treated, if possible. In all cases, diagnosis is made by barium contrast radiography of the pharynx and esophagus to confirm the presence, size, and position of the diverticulum. Endoscopic confirmation of the diverticulum should only be undertaken as part of the definitive surgical therapy, as it is otherwise unnecessary and potentially dangerous. Given the extremely low incidence of carcinoma occurring in the diverticulum, endoscopic evaluation should be done only when sufficient symptomatology and abnormality on barium esophagram exist to raise suspicion of malignancy.17 The radiographic findings of recurrent ZD depend on the surgical procedure used for initial treatment. Those patients treated with an endoscopic diverticulotomy approach will routinely demonstrate a diverticular remnant on the barium study (Fig. 26.1).18,19 The hallmark of recurrent ZD in this setting is retention of barium in the remnant after repeated swallowing, combined with persisting or recurring symptoms. Similar radiographic features, along with possible enlargement of the diverticulum, may be present in those patients treated by means other than diverticulectomy or endoscopic diverticulotomy. Those patients treated initially by diverticulectomy will demonstrate the presence of a diverticulum on barium studies, although symptoms as severe as before the initial treatment may be present even though the recurrent ZD may be smaller than the original. Radiographic signs of distal pharyngeal or proximal esophageal narrowing should also be looked for in those patients previously treated by diverticulectomy, or in whom initial surgery may have been complicated by fistula and associated infection. Decision tree for treatment of recurrent Zenker’s diverticulum Fig. 26.1 Lateral view, barium esophagram demonstrating a recurrent Zenker diverticulum after prior endoscopic staple diverticulostomy. Barium retention is noted in the diverticulum after multiple swallows. Although it was widely accepted that ZD was an acquired pulsion diverticulum, there was and still remains considerable controversy on the mechanism of formation. Ludlow1 gave the first anatomical description of a pulsion diverticulum of the hypopharynx in 1769, but it was not until 1878 that the basic pathophysiology was described by Zenker and von Ziemssen.20 In 1816 Bell21 proposed inappropriate coordination of the inferior constrictor muscle against a closed cricopharyngeus muscle as an etiology for ZD. The endoscopic observations of Jackson and Shallow22 reported in 1926 provided clinical evidence suggesting that the cricopharyngeus muscle was responsible for development of ZD. Ever since, variations on this mechanistic theme behind the formation of ZD have been proposed, including studies supportive of premature cricopharyngeal relaxation, delayed cricopharyngeal relaxation, and cricopharyngeal spasm as the responsible factors in the genesis of the diverticulum.22 Regardless of the theory, the cricopharyngeus muscle was most commonly believed to be the culprit responsible for the formation of ZD. This led to the concept of including cricopharyngeal myotomy in the surgical management of ZD, either as a primary procedure or in conjunction with diverticular resection or suspension.3,8,13,14 Even with this generally accepted concept as to causation, no such agreement was present regarding the appropriate means of treatment for patients with ZD. Proponents could be found supporting cricopharyngeal myotomy alone,8 diverticulectomy or diverticulopexy alone,4 or a combined approach of myotomy together with diverticular resection or suspension.3,5 Despite refinements in surgical techniques, no approach proved clearly superior to the others in treatment outcome. All of these techniques were reported to provide symptomatic relief in ~80 to 90% of patients, although with serious complication rates of up to 30% and mortality as high as 3%.3,9,14,23 In most cases, no direct comparisons were made by prospectively studying one treatment method against another, and long-term analysis of results was often lacking. Furthermore, none of the techniques proved to be superior to the others at preventing recurrence of the ZD, with recurrence rates reported to range from 0 to 20%.3,9,14,23 These results made it difficult to determine whether the addition of cricopharyngeal myotomy would prevent recurrence or improve symptom outcome. As a result, efforts were directed at trying to minimize the immediate morbidities associated with surgical treatment, while still incorporating management of the cricopharyngeus muscle into the overall treatment scheme. One of the first such efforts was made in 1917 by Mosher,9 who first described endoscopic esophagodiverticulostomy using a knife to divide the common wall. This technique proved successful at relieving symptoms, but it was abandoned after the seventh patient died from mediastinitis. Sieffert24 in 1937 reintroduced the endoscopic technique, but it was Dohlman and Mattson25 who popularized the procedure. In 1960 they presented the results of endoscopic management of ZD in a series of 100 patients without treatment-related deaths or serious complications, with 93% of patients reporting relief of symptoms. However, because of concern related to the “sutureless” division of the common wall between the diverticulum and the esophagus, with the potential for pneumothorax, bleeding, or mediastinitis, endoscopic management of ZD did not gain truly wide acceptance. Various refinements in endoscopic technique have been introduced in an attempt to alleviate these concerns and eliminate the severe complications Mosher9 initially experienced. Dohlman and Mattsson25 used diathermic coagulation to divide the common wall in 1958. More recent modifications to this method included the use of the microscope and carbon dioxide (CO2) laser described by van Overbeek et al26 in 1984 and potassium titanyl phosphate (KTP)/532 laser in 1992 by Kuhn and Bent.27 Gastroenterologists Ishioka et al28 in Brazil and Mulder et al29 in the Netherlands simultaneously introduced flexible endoscopic incision using electrocautery in 1995. Yet even these refinements in endoscopic technique were associated with rates of mediastinitis as high as 8 to 10%. To address this concern, a modification of the endoscopic technique was described in 1993 by Martin-Hirsch and Newbegin30 in England and Collard et al31 in Belgium, who simultaneously introduced the endoscopic stapling technique of performing an esophagodiverticulostomy for ZD. This technique was refined and introduced to the United States in 1996 by Scher and Richtsmeier32 as endoscopic staple esophagodiverticulostomy (ESED). Several advantages have been shown for the stapling technique compared with endoscopic approaches using laser or electrocautery or the open surgical techniques, including greatly reduced risks of perforation, mediastinitis, and laryngeal nerve injury, more rapid return to oral diet, and shorter operative times and hospital stays.32–34 When compared with other treatment approaches, endoscopic staple diverticulostomy (ESD) has been shown to have at least equal effectiveness at providing symptom resolution.33,34 These features have proven especially attractive in patients who are often elderly and may have coexistent significant medical illness. The results reported for ESD now support the use of this technique as the treatment of choice for all patients with ZD. Although treatment for ZD has evolved to provide predictably effective and safe treatment by the ESD technique, recurrent ZD may occur following this or any other treatment. Rates of recurrence from 0 to 20% have been reported regardless of technique.11,13,14,26,33,34 As stated, although the altered function of the cricopharyngeus muscle has received the greatest focus, and failure to adequately perform cricopharyngeal myotomy has been proposed by most surgeons as the primary reason for recurrence, neither this factor nor any others have consistently proved to be clearly associated with recurrence of symptoms from ZD following treatment. Factors such as gastroesophageal reflux and esophageal or pharyngeal dysmotility are often present in patients with ZD, and failure to address these disorders may lead to continued complaints of difficulty swallowing.12
Clinical Features

Pathogenesis and Rationale for Treatment Selection
Recurrent Zenker Diverticulum
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine