CHAPTER 11 Wound construction

ECCE
Scleral ECCE wound
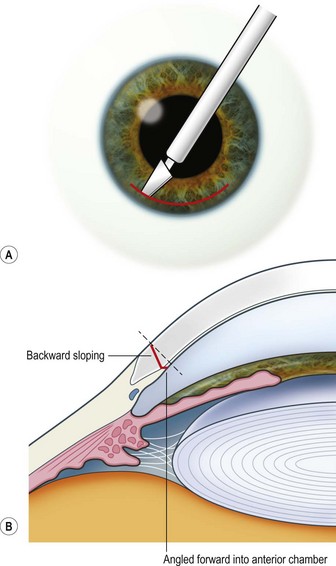
The scleral wound is made around 120°, initially backward sloping and then, when the deeper tissues are reached, a forward entry into the eye is made (Fig. 11.1). More bleeding is likely because of perforating scleral vessels and diathermy is a prerequisite. Careful wound construction and suturing can be rewarded by very little surgically induced astigmatism because of the distance from the optical centre of the cornea and the ability to leave the sutures at the desired tension.
Corneal ECCE wound
This should be made approximately 1 mm into clear cornea and sloped gently backwards. This ensures that the sutures when placed to close the wound will enter and exit corneal tissue and avoid the need for reflecting the conjunctiva (see Fig. 11.1).
The relative advantages and disadvantages of scleral and corneal ECCE wounds are summed up in Table 11.1.
Table 11.1 Comparison of corneal and scleral section
| Section |
|---|



