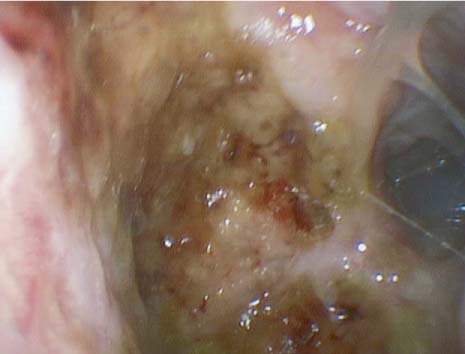
42 A 57-year-old woman is referred to the otolaryngology clinic for evaluation of chronic sinusitis. The primary physician treated the patient with multiple courses of antibiotics, nasal steroid sprays, saline irrigations, and topical decongestants over the past several years with no noticeable resolution of symptoms. On questioning in the otolaryngology clinic, the patient is complaining primarily of intermittent bilateral mucoid rhinorrhea, chronic intermittent epistaxis, aural fullness, decreased hearing, and nasal obstruction. This has been stable over the past several years. Review of systems revealed some malaise, generalized fatigue, diffuse arthralgia, and a 10-pound unintentional weight loss over the last year. She denies nasal trauma, nasal surgery, otolologic surgery or trauma, shortness of breath, stridor, hemoptysis, or skin changes. She does not abuse over-the-counter topical decongestants or cocaine. However, she is also concerned about the appearance of her nose which she feels has become less prominent recently. She attributes this to aging and is considering rhinoplasty. Physical examination reveals a thin woman who appears her stated age. She is in no distress. She has an obvious deformity of the nasal dorsum with a significant depression overlying the cartilaginous septum. Anterior rhinoscopy reveals dry nasal mucosa with several excoriated areas of crusting along the anterior septum and inferior turbinates (Fig. 42.1). There is obstructing clot and crusts in the nasal cavities bilaterally. After removing the clot, a large septal perforation is revealed. Nasal endoscopy shows no evidence of mass or anatomic obstruction of the osteomeatal complex. The nasopharynx is clear. There is a unilateral effusion in the left middle ear space. Tuning fork examination is consistent with a conductive hearing loss in the left ear. Fig. 42.1 Right nasal cavity of a patient with Wegener granulomatosis. Note the dried nasal mucus crusting to the lateral and posterior nasal wall. 1. The differential diagnosis for this middle-aged woman with a large septal perforation includes nasal trauma, sinonasal surgery, overuse or abuse of topical decongestants or cocaine, neoplasm, systemic inflamma-tory and autoimmune diseases, and infectious processes. 2. The absence of a mass on thorough nasal endoscopic examination of the nasal cavities and nasopharynx makes neoplasm unlikely. 3.
Wegener Granulomatosis
History
Differential Diagnosis—Key Points
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


