and Mitrofanis Pavlidis2
(1)
Department of Ophthalmology, Uppsala University Hospital, Uppsala, Sweden
(2)
Augencentrum Köln, Cologne, Germany
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-319-20236-5_8) contains supplementary material, which is available to authorized users.
Electronic supplementary material
for this chapter is accessible online at http://extras.springer.com/ by searching via the ISBN.
8.1 Introduction
Video 8.1: 27G-Difficult PVD
Video 8.2: VMTS with many complications_no audio
In VMTS a PVD is always necessary. PVD can be performed in most cases with the vitreous cutter, but in a few cases the usage of a forceps is advisable because you may create otherwise a macular hole. The 27G vitreous cutter is superior to the 25G and 23G regarding PVD because you can place the tip of the cutter very close to the retina. We recommend a 90D lens for PVD or a good zoom on the optic disc when using a widefield lens.
Be careful in cases with a detached macula and a vitreofoveal adhesion (Fig. 8.1); you may create a macular hole when inducing a forceful PVD with the vitreous cutter. Stain in these cases the vitreous with trypan blue or triamcinolone and peel the posterior vitreous membrane with a forceps from the macula. If you do not succeed with the forceps, then create a hole with a retinal scraper (e.g. 27G retrobulbar cannula, Atkinson, Beaver-Visitec).
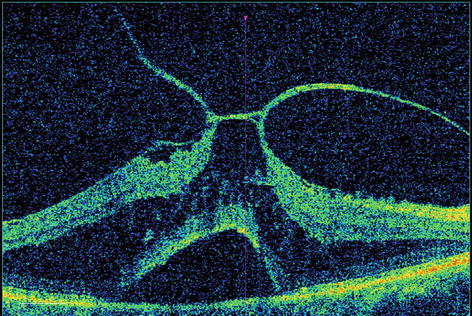
Fig. 8.1




Vitreomacular traction syndrome with a retinal schisis and subfoveal fluid. Avoid damaging the fovea when removing the posterior hyaloid
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
