Chapter 23
VITREOUS AND RETINA

The incidence of seriousa ocular injuries shows no sign of abating. This is despite intensive efforts to heighten public awareness through robust educational campaigns and explicit warnings directed at prevention in the home, at the workplace, and during recreation (see Chapters 4 and 27). The physical, psychological, and socioeconomic suffering of individuals afflicted with severe ocular trauma can last a lifetime, and the financial implications, both personal and in terms of national productivity and health care maintenance, are incalculable.
In the last decade, refined microsurgical techniques and instrumentation, the availability of intraocular antibiotics, and a better understanding of the pathophysiology of the severely injured eye have resulted in the improvement of the visual outcome in patients with severe ocular trauma (see Chapters 8 and 24). Even in cases with a discouraging visual prognosis, the benefits in terms of good cosmetic reconstruction and repair should not be underestimated (see Chapters 25 and 31).
This chapter deals with the clinical features, pathophysiology, and management of closed and open trauma involving the two structures of the posterior segment that are most commonly injured. Trauma involving the choroid, IOFBs, and the optic nerve are discussed in Chapters 22, 24, and 37, respectively; Chapters 16 and 26 address additional issues related to the vitreous and the retina.
EPIDEMIOLOGY AND PREVENTION
Recent epidemiological data confirm the disturbing trend in the prevalence of severe ocular trauma.1 The home has now surpassed the workplace as the most common site for serious ocular injury, testament perhaps to the huge growth of the “do-it-yourself” home enthusiast and/or a decrease in work-related injury (see Chapter 4). They also confirm that most eye injuries are preventable, occurring in people who wear no eye protection.1–4,b
Traumas from blunt and sharp objects are the two major causes of severe ocular injuries, and in the USEIR, the retina and vitreous are second only to the cornea as the most frequently involved ocular tissues.1 It is no coincidence, therefore, that the posterior segment manifestations of severe ocular trauma are foremost as the cause of severe and permanent visual morbidity (Fig. 23–1).
Retinal detachment following contusion is not uncommon5,6 and is observed primarily in males,4,7–10 especially in the younger age groups.1,2,8–10 The USEIR found the following information.
Rate of retinal involvement among all serious injuries: 31%.
• Among closed globe injuries: 34%.
• Among open globe injuries: 29%.
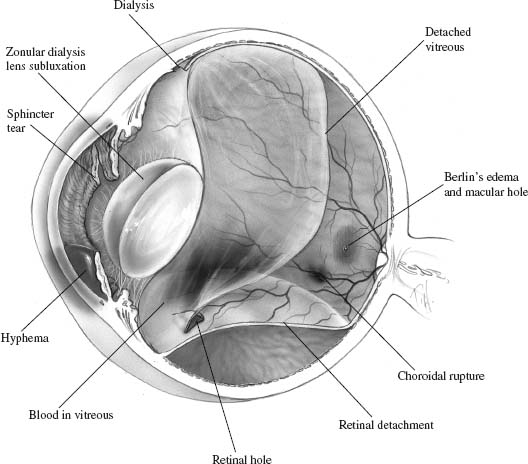
FIGURE 23–1 Various intraocular injuries involving both the anterior and posterior segments can result from trauma by blunt objects. (From Aaberg TM and Sternberg P. Blunt and penetrating ocular injuries. In: Regillo CD, Brown GC, Flynn HW, ed. Vitreoretinal Diseases: The Essentials. New York: Thieme; 1999:515.)
Rate of vitreous involvement among all serious injuries: 31%.
• Among closed globe injuries: 22%.
• Among open globe injuries: 40%.
Rate of vitreoretinal involvement among all serious injuries: 44%.
Age (years):
• range: 0–103;
• mean: 30;
• ≤15: 25%;
• 20 to 39: 49%;
• ≥60: 8%.
Sex: 82% males.
Place:
• Home: 41%;
• Place for recreation and sport: 15%;
• Industrial premises: 14%;
• Street and highway: 11%.
Cause:
• blunt object: 32%
• sharp object: 14%
• BB/pellet gun: 9%;
• gunshot: 8%;
• hammering: 7%
• MVC: 7%;
• fireworks: 6%;
• nail: 6%.
Among retinal injuries (= 100%):
• hemorrhage: 35%;
 macular: 5%;
macular: 5%;
• defect: 20%;
 macular hole: 0.07%; among eyes with contusion:c 1.4%; among eyes with open globe injury:d 0.15%;
macular hole: 0.07%; among eyes with contusion:c 1.4%; among eyes with open globe injury:d 0.15%;
 macular commotio: 4%;
macular commotio: 4%;
• retinal detachment: 26%;
 hemorrhagic: 7%;
hemorrhagic: 7%;
 rhegmatogenous: 8%;
rhegmatogenous: 8%;
 macular: 2%.
macular: 2%.
Despite tremendous advances in therapy, the mainstay of tackling the global problem of ocular trauma (see Chapter 4) remains prevention. Time and again, it has been shown that regardless of the setting, the correct ocular protection not only prevents injuries11–14 but also markedly reduces the severity of injury.
RETINA
Closed Globe Injury
Pathophysiology
High-speed cinematography was used to study experimentally the effects of contusion resulting from high-speed pellets.15 The ocular damage resulting from the impact could be explained in four phases of globe deformation:
1. compression;
2. decompression;
3. overshooting;
4. oscillations.
It appears that both retinal dialysis and peripheral retinal tears occur secondary to tractional forces generated at the vitreous base as the equatorial diameter of the globe increases rapidly.16
PEARL… The vitreous body is relatively inelastic and cannot stretch when the eye is rapidly compressed.
Retinal breaks can occur via the following mechanisms:
• Vitreous base avulsion. Extreme traction on the vitreous base may cause its anterior border to be ripped from either the retina or pars plana.16 The distribution of the retinal tears in this model mirrors closely the retinal changes seen clinically.17,18
• Abnormal sites of vitreoretinal adhesion (e.g., lattice degeneration).
• Coup injury. Local trauma at the site of scleral impact19 induces a direct, concussive, full-thickness necrosis of the overlying retina.20,e
• The induction of sudden posterior vitreous detachment.Evaluation
PEARL… It is probably the site of the initial impact that determines the exact distribution of the consequent retinal abnormalities.16
Evaluation
Fundamental in the evaluation of any patient presenting with ocular trauma is a comprehensive history and a careful physical examination (see Chapters 8 and 9).
The precise circumstances surrounding the injury must be thoroughly elucidated and the exact mechanism of the injuryf must be ascertained; this helps predict whether vitreoretinal involvement must be anticipated. It is essential to establish the shape of the agent, that is, blunt versus sharp.
PEARL… In cases of a projectile causing ocular trauma, the foreign body must be assumed intraocular until proved otherwise (see Chapter 24).
The importance of examining both eyes cannot be overemphasized.
PEARL… “In the heat of moment” the physician is often preoccupied with ascertaining the full extent of damage to the eye the patient is referring to or the eye obviously involved, while the other eye may also harbor serious disease.g
PITFALL
The possibility of bilateral ocular injury should always be excluded despite a unilateral presentation.2
• Regardless of how mild or severe an ocular injury first appears, a baseline visual acuity for both eyes should be recorded (see Chapter 9).
• The presence or absence of an APD should be documented as this provides vital prognostic information for the visual outcome (see Chapter 3).21
• It is imperative to comment on the integrity of each ocular structure in turn.
• Media opacities (e.g., corneal edema, hyphema, cataract, vitreous hemorrhage) can make thorough evaluation of the posterior segment extremely difficult or even impossible.
PEARL… In the absence of a clear IBO view of the ocular fundus, B-scan ultrasonography is an excellent alternative (see Chapter 9). It should be repeated periodically until the view improves or intraocular pathology requiring surgical intervention is detected.
PITFALL
The presence of an anatomically normal anterior segment, normal vision, or lack of pain should not deter the examiner from seeking the possibility of serious and sight-threatening posterior segment pathology.10
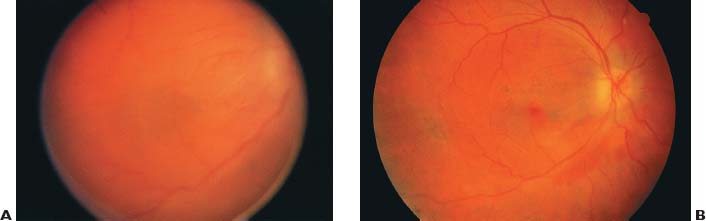
FIGURE 23–2 (A) Patient presents following severe contusion to eye. Examination discloses retinal whitening in the posterior pole and in the periphery consistent with commotio retinae. (B) Within a few days, the retinal whitening has subsided and RPE pigmentary disturbance in noted in the macula.
It must be remembered that retinal tears and detachment may develop years after the original trauma.
PEARL… All patients with a history of contusion should be followed at least until the ora serrata can be viewed for 360°.17,18,22,23
Clinical Conditions
Commotio Retinaeh is a relatively common consequence of contusion.
CLINICAL FEATURES First described in 1873,24 this injury is typically caused by contusion and is characterized by transient gray-white discoloration or opacification of the outer sensory retina. The opacification may be confined to the macula or may involve extensive areas of the peripheral retina.25
When the posterior pole is affected, a cherry-red spot at the fovea mimicking that in acute central retinal artery occlusion may be seen. There may be associated hemorrhage (preretinal, retinal, subretinal) and choroidal rupture (Fig. 23–2).25
The symptoms are determined primarily by the location of the lesion, for example, its relation to the macula. The patient may have no visual complaints if only the peripheral retina is involved or severe visual impairment if extensive macular lesions are present. As the retinal opacification resolves, vision may return to normal and there may be no ophthalmoscopic findings after the resolution.
Pigmentary disturbance may occur following commotio retinae; with resolution of the edema, it may mimic retinitis pigmentosa.26,27
PATHOPHYSIOLOGY The pathophysiology of commotio retinae has been the subject of much controversy. It was originally postulated that the retinal opacification was due to extracellular edema.24 Later experimental studies, however, identified disruption of the photoreceptor outer segments as the main histopathologic findings.28–30 One experimental study28 found the following.
• Disruption of photoreceptor outer segments occurred immediately after injury.
• Phagocytosis of the fragmented outer segments by RPE cells developed at 24 hours.
• Within 48 hours after the injury, RPE cells had begun to migrate among the outer segment fragments and into the outer retina. This migration reached as far as the ganglion cell and inner plexiform layers.
• The RPE became a multilayered, disorganized structure on Bruch’s membrane with atrophy of the overlying photoreceptor outer segment.
• In areas of severe atrophy, the photoreceptor outer segment could not be detected at all, resulting in direct apposition of the inner segment with the RPE.
• There was no evidence of intracellular or extracellular retinal edema in this animal model, which appears clinically similar to patients with this condition.
 No leakage of fluorescein from retinal capillaries could be demonstrated at any time after injury.
No leakage of fluorescein from retinal capillaries could be demonstrated at any time after injury.
PEARL… Commotio retinae is associated not with extracellular edema but with disruption of photoreceptor outer segments.28
PEARL… Commotio retinae is associated not with extracellular edema but with disruption of photoreceptor outer segments.28
An FA study30 found the following.
• No fluorescein leaked from the retinal vessels 30 minutes after injury, but there was progressive staining of the RPE in the posterior pole.
• Following severe ocular contusion, the RPE underlying the opacified retina undergoes significant anatomic and functional changes.
• These changes range from cellular disruption immediately after the injury to rounding up and migration of RPE cells into the outer layers of the neurosensory retina.
• Eventually, hyperplasia of the RPE occurs.
A histopathologic study31,i in humans found the following.
• Photoreceptor outer segment disruption and damage to the RPE.
• Only a minimal amount of albumin around retinal vessels was detected by immunohistochemistry, indicating the minimal role of the blood-retinal barrier defect in the pathogenesis of commotio retinae.
Disruption of the blood-retinal barrier at an average of 16 hours after injury was confirmed in a clinical study using FA and vitreous fluorophotometry.32
PEARL… There is no treatment of proven benefit for commotio retinae. Visual acuity tends to recover in the majority of cases, except in those with severe macular involvement or other associated intraocular damage.33
MANAGEMENT AND PROGNOSIS In a prospective study:33
• 60% of patients with commotio retinae affecting the macular region had recovery of visual acuity within 2 weeks of injury;
• 40% were left with permanent macular damage and varying degrees of visual loss.j
Chorioretinitis Sclopetaria is an uncommon consequence of trauma by a blunt object.
PEARL… Chorioretinitis sclopetaria is a distinct closed globe injury typically caused by transmitted shock waves from a high-velocity missile penetrating the orbit and grazing, but not perforating, the sclera.
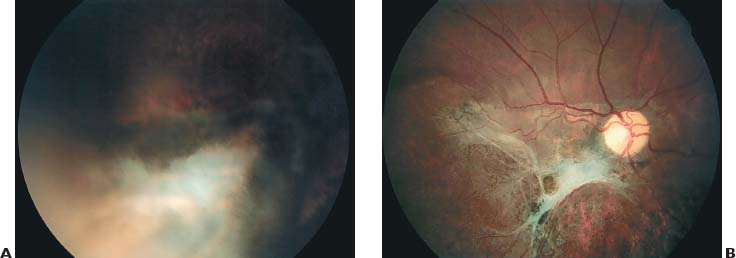
FIGURE 23–3 Chorioretinitis sclopetaria. (A) Inferior part of the posterior pole in a 15–year-old boy after he was shot with an air gun from a distance of 15 meters. The bullet penetrated his right lower eyelid and was lodged in the inferior part of the orbit. He noted immediate loss of vision in the right eye. IBO on the day of the injury disclosed a radially oriented chorioretinal break in the inferior part of the fundus with overlying vitreous hemorrhage and a preretinal hemorrhage over the macula. (B) Six weeks following the injury, note the bare sclera visible through the defect of the choroid, Bruch’s membrane, and retina, with surrounding hyperpigmentation, as a result of direct injury to the inferior retina adjacent to the path of the high-velocity missile. Note the irregular pigmentary disturbances and the preretinal gliotic membrane involving the optic disk and macula as a result of indirect injury of the posterior pole. The macular lesion is not contiguous with the inferior lesion. Visual acuity is counting fingers. (From Beatty S, Smyth K, Au Eong KG, Lavin MJ. Chorioretinitis sclopetaria. Injury. 2000;31:55–60. Reprinted by permission from Elsevier Science.)
HISTORY AND EPIDEMIOLOGY Although the term was first used in the German literature in 1901,34 the earliest description of the condition was in a book on war injuries published in 1872.35,k
Chorioretinitis sclopetaria is relatively rare,36 especially during peacetime; the largest published series includes only eight cases.37 It is typically caused by gun injuries37–39 but has been described in association with injuries from objects such as the nozzle of a high-pressure water hose,37 metal rod,37 and fishing line sinker.40
PATHOPHYSIOLOGY There are typically two distinct areas of injury in chorioretinitis sclopetaria (Fig. 23–3).
1. The first site is the area adjacent to the path of the missile; the injury is caused directly by the concussive force of the missile.
• Rapid deformation of the globe by a high-velocity missile or its shock waves causes a sudden increase in stress in the sclera, choroid, retina, and posterior vitreous cortex.37
• These tissues rupture in areas where the induced tensile stress is greater than the tensile strength of the tissue.
• Typically, there is full-thickness rupture of the choroid, Bruch’s membrane, and retina. This is accompanied by retraction of these tissues to expose the underlying sclera.
• The chorioretinal rupture is oriented radially if the missile has come to rest deep in the orbit.37
2. The second area of injury is remote from the path of the missile and typically involves the macula.
• The injury is believed to result indirectly from transmission of shock waves through the wall of the eye (see Chapter 22).
• When the force is severe, there may be only one large lesion involving both areas.41
CLINICAL FEATURES include the following.
• Immediately following the injury, acute loss of vision.
 Visual acuity in the range of counting fingers is not uncommon because of the severity of the force.37,39
Visual acuity in the range of counting fingers is not uncommon because of the severity of the force.37,39
• There are usually extensive retinal and choroidal hemorrhages as well as tears in these layers.
• The sclera remains intact.
• Preretinal and vitreous hemorrhages are often present.39
• The vitreous hemorrhage may obscure the view of the fundus, and only after the blood has cleared can the typical pigmentary disturbance and retinal scarring be seen (Fig. 23–4).
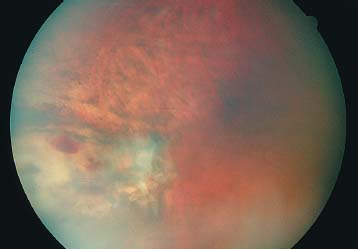
FIGURE 23–4 Within weeks of orbital missile injury an area of healing sclopetaria is present in the periphery. As the blood clears, fibrous proliferation as well as RPE proliferation and mottling are present. In some areas, bare sclera may be evident.
• The lesion heals with the development of white, fibrous scar tissue with pigment at its edges.41,42
• Acute retinal detachment is rare.
PEARL… That acute retinal detachment is so uncommon in chorioretinitis sclo-petaria may be explained by the fact that the retraction of the choroid and retina as a single unit and the typically intact posterior hyaloid face prevent the access of fluid to the subretinal space.37 In addition, patients tend to be relatively young and have formed vitreous, thus lowering the risk of retinal detachment.37
• In the later stages, the resultant spontaneous “retinopexy” usually does not allow a retinal detachment to occur in areas of pigmentary retinal changes.
PITFALL
Late retinal detachment has been reported in one fourth of patients in one study, due to retinal breaks at a site distant from the original chorioretinal rupture.37
MANAGEMENT The clinical findings of a large retinal break with surrounding retinal edema may prompt surgical intervention for treatment of a presumed retinal detachment.
SPECIAL CONSIDERATION
Despite the lesion’s striking appearance, observation, not surgical intervention, is the appropriate initial management for these injuries because acute retinal detachment is so rare.37
• Pars plana vitrectomy may be necessary for non-clearing vitreous hemorrhage, which is more common in young patients with formed vitreous gel.
• It is important for ophthalmologists to be familiar with the clinical features of this condition so that an accurate diagnosis can be promptly established and unwarranted surgical intervention avoided.39
PROGNOSIS The visual prognosis of chorioretinitis sclopetaria is variable. If there is severe scarring of the macula, the visual prognosis is poor. However, cases with return of vision to 20/20 have been reported.37
PEARL… The physician’s primary goal with chorioretinitis sclopetaria is to make a prompt and accurate diagnosis so that unwarranted surgical intervention is avoided.39
Traumatic Macular Hole is a relatively common complication of contusion, and may occur within hours of the incident.
CLINICAL FEATURES The fovea, devoid of the inner retinal layers or blood supply, is vulnerable to fullthickness hole formation following contusion.
• Traumatic macular hole is believed to account for fewer than 10% of all macular holes.43
• Macular hole is most commonly caused by contusion44–47 but has also been reported in association with accidental laser injury48,49 and retrobulbar needle globe perforation.50
• Atraumatic macular hole typically ranges in size from 0.2 to 0.5 disk diameter and may be oval or round.51
• Patients with traumatic macular holes tend to be young, and posterior vitreous detachment is typically absent in these eyes.51,52
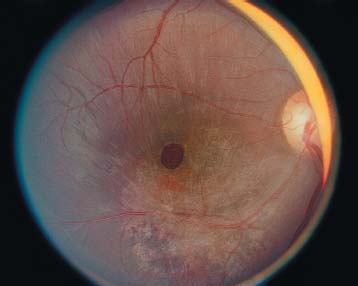
FIGURE 23–5 Traumatic macular holes often have associated macular findings that result from the contusion injury. In this patient, in addition to the large central full-thickness hole, adjacent RPE disturbances can be seen. Some epiretinal proliferation is also present.
• In one series, the traumatic macular holes were associated with other injuries including:
 commotio retinae in 35%;
commotio retinae in 35%;
 massive vitreous hemorrhage in 25%;
massive vitreous hemorrhage in 25%;
 hyphema in 25%; chorioretinal atrophy in 25%;
hyphema in 25%; chorioretinal atrophy in 25%;
 choroidal rupture in 20%;
choroidal rupture in 20%;
 angle recession in 20%;
angle recession in 20%;
 peripheral retinal tears in 10%; and
peripheral retinal tears in 10%; and
 retinal dialysis with retinal detachment in 5% (Fig. 23–5).51
retinal dialysis with retinal detachment in 5% (Fig. 23–5).51
PATHOPHYSIOLOGY The exact mechanism by which traumatic macular hole develops is not well understood. Possible mechanisms mentioned earlier were contusion necrosis, subfoveal hemorrhage, and vitreous traction.25 In one documented case the macular hole enlarged from a tiny dehiscence in the fovea after trauma.47 Based on recent data, surface traction has been identified as a major component in the etiology of traumatic macular holes.53 Rigidity of the ILM may play an important role (R. Morris, F. Kuhn, J. Dalma, personal communication).
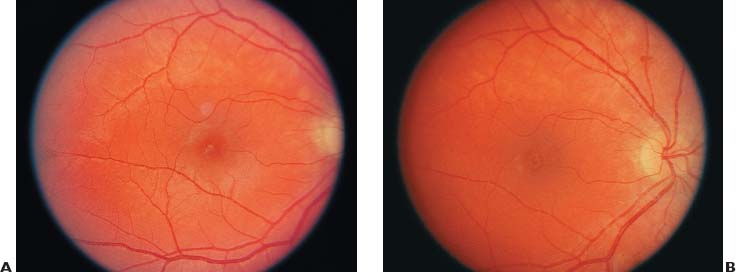
FIGURE 23–6 (A) Following an MVC and contusion to the eye, a small, full-thickness macular hole developed with 20/100 vision. (B) Over the next 4 months, there was gradual closure of the hole without surgery, and vision returned to 20/30.
Vision is usually in the range of 20/100 to 20/400 following the development of a full-thickness macular hole. Occasionally, the hole may spontaneously close,54,l with or without full recovery of the visual acuity (Fig. 23–6).
MANAGEMENT Until recently, there was no treatment for macular hole.6 Based on a theory regarding pathogenesis for idiopathic macular holes55 and the success with surgery for idiopathic and traumatic holes,47,49,50,52,53,56–61 it is now more difficult for the surgeon to justify foregoing intervention.
CONTROVERSY
Spontaneous closure of traumatic macular holes does occur in a few cases, especially in young patients. However, observation is a dubious initial treatment option, since most holes are not expected to close without surgical intervention and may lessen the chance of a good anatomical and functional recovery.53,m
l Glial cell proliferation may play an important role in spontaneous closure of the macular hole.
The current standard treatment includes a three-port pars plana vitrectomy, peeling of the posterior hyaloid face from the posterior pole, intravitreal gas tamponade, and postoperative face-down positioning for about up to 2 weeks. ILM removal is becoming increasingly popular.
PEARL… As with surgery for idiopathic macular holes, removal of the macular ILM appears to increase the anatomical and functional success rates in patients with traumatic macular holes.53 It also seems from published data that early intervention has distinct advantages, possibly even more so than for an idiopathic macular hole.
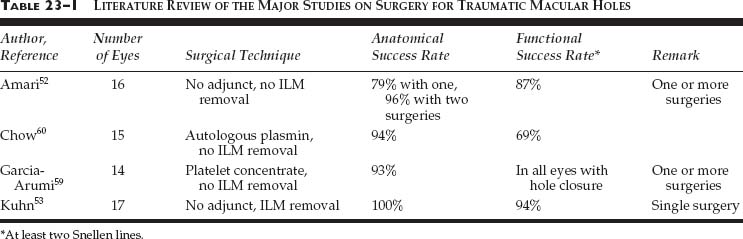
PROGNOSIS Vitreous surgery, with or without adjuvant therapy or ILM peeling, can lead to hole closure and visual improvement in most eyes. The favorable results may be due to the younger age of these patients and the shorter duration of the macular hole.52 Table 23–1 provides an overview of the major studies.
Vitreous Base Avulsion is rare.
CLINICAL FEATURES Avulsion of the vitreous base per se does not cause retinal detachment and usually does not require intervention other than observation.
The symptoms may be minimal.n
PEARL… It is the presence of avulsion, recognized as part of the vitreous base draped over the peripheral retina (the so-called bucket-handle) sign, that confirms the history of significant contusion.
The pathognomic presence of vitreous base avulsion should alert the clinician to the likely possibility of severe underlying ocular pathology (e.g., retinal dialysis, peripheral [giant] retinal tears, angle recession).
MANAGEMENT No surgical intervention is necessary. However, close follow-up is recommended until the ora serrata and pars plana area can be adequately visualized to rule out retinal dialysis or tears of the pars plana.62
Retinal Dialysis is probably more common than generally perceived.
CLINICAL FEATURES Retinal dialysis is the most frequent traumatic retinal break.5 It almost always occurs at the time of the injury.16,18 It may be defined as a break or separation occurring at the anterior edge of the ora serrata and, unlike tears secondary to posterior vitreous detachment with or without a history of trauma, the vitreous remains attached to the posterior edge of the dialysis63,64 (Fig. 23–7). This intimate anatomical relationship is probably responsible for the slow progression from retinal dialysis to retinal detachment.
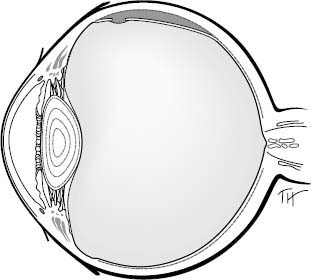
FIGURE 23–7 A retinal dialysis differs from a giant retinal tear as the vitreous spans the retinal defect and provides stability to the posterior retinal edge, making a detachment less likely. (From Tiedeman JS. Retinal tears and rhegmatogenous retinal detachments. In: Regillo CD, Brown GC, Flynn HW, ed. V’treoret’nal D’seases: The Essentials. New York: Thieme; 1999;476.)
A retinal dialysis may be difficult to visualize initially because of the minimal separation between the retina and ora serrata. The difficulty in early detection is borne out by published reports. In one series, 41% of retinal detachments associated with retinal dialyses were first diagnosed more than 1 year following the original injury.63
Scleral depression may aid the diagnosis, but is rarely possible in a child.
PITFALL
Caution is advised at the initial evaluation with respect to scleral depression: it may cause further damage to an already compromised eye.
Retinal detachments related to dialysis are usually slow to develop,65 giving the ophthalmologist a window of opportunity to detect and treat them, provided regular follow-up and meticulous examination of the patient are performed.
PITFALL
>A retinal dialysis may not be visible at the initial examination and may be overlooked at subsequent examinations.22,63,66
It is difficult to overstate the importance of proper examination of the entireo ora serrata. In one study:23
• 66% of dialyses were located in the inferotemporal quadrant;
• 10% in the superotemporal quadrant;
• 4% in the inferonasal quadrant;
• 6% of retinal dialyses occurred in more than one quadrant.
The predilection for the inferotemporal and, to a lesser extent, superonasal quadrants has been confirmed in several reports.16–18,22,65,67,68
PEARL… The most common retinal dialysis location is the inferotemporal quadrant.7,63,65,69 However, because the dialysis can occur in any quadrant, thorough evaluation of the entire ora serrata is necessary.
MANAGEMENT includes the following.
• In the absence of retinal detachment, most retinal dialyses should be treated prophylactically with transscleral cryoretinopexy or, preferably, laser retinopexy.
• Early recognition of retinal dialysis is the key to avoiding more extensive intervention.
• Not all retinal dialyses lead to retinal detachment. Occasionally, a dialysis will seal spontaneously due to a vigorous chorioretinal response to the insult.
PEARL… If the surgeon elects not to treat a retinal dialysis, regular follow-ups are mandatory, and the patient should be counseled (see Chapters 5 and 8) with respect to this management strategy.
Peripheral Retinal Breaks are a common source of posttraumatic retinal detachment.
CLINICAL FEATURES The location and configuration of flap horseshoe or “U” tears tend to mimic those associated with a spontaneous posterior vitreous detachment. The typical appearance of the horseshoe flap or an operculum confirms an etiology secondary to vitreous traction.
The symptoms are also similar with complaints of:
• floaters;
• photopsia; and/or
• blurred vision from primary or secondary vitreous hemorrhage.
PEARL… The risk of progression to retinal detachment in case of a horseshoe tear is much greater than with a retinal dialysis.
Tears from full-thickness retinal necrosis are usually slower to evolve and are more likely than tears from vitreous traction to be associated with periretinal hemorrhage. These tears also tend to be large, more irregular, and located at the site of direct ocular contusion.
• Peripheral retinal breaks without visible evidence of traction (retinal holes) tend to be small and round.
• Stretch tears supposedly occur in the setting of rapid horizontal expansion of the eye. They are usually located anterior to the equator and have a curvilinear configuration. They may progress to retinal detachment or seal spontaneously.
• Giant retinal tears, defined as retinal tears involving 90° or more of the circumference of the globe, are commonly associated with contusion70,71 (Fig. 23–8).
 Myopic males appear to be at a higher risk of developing giant retinal tears from contusive injury.71
Myopic males appear to be at a higher risk of developing giant retinal tears from contusive injury.71
 Occasionally, giant tears can be seen secondary to trauma-induced full-thickness retinal necrosis.
Occasionally, giant tears can be seen secondary to trauma-induced full-thickness retinal necrosis.
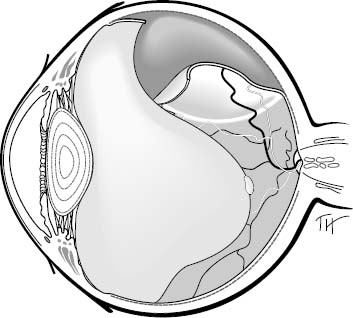
FIGURE 23–8 In a giant retinal tear the vitreous separates from the posterior edge of the retina, allowing the retinal edge to detach and roll over in some cases. (From Tiedeman JS. Retinal tears and rhegmatogenous retinal detachments. In: Regillo CD, Brown GC, Flynn HW, ed. Vitreoretinal Diseases: The Essentials. New York: Thieme; 1999;475.)
PEARL… The presence of periretinal hemorrhage following ocular trauma should alert the clinician to the possibility of underlying retinal tears.
PATHOPHYSIOLOGY A retinal tear secondary to contusion occurs when the transmission of an external force causes sudden and rapid distortion of the globe.
• The eye shortens anteroposteriorly and elongates equatorially.
• The relative inelasticity of the eyewall, coupled with the fact that the eye is a fluid-filled structure and therefore relatively resistant to compression, means that the globe cannot adequately stretch in response to this deformation.
• The volume of the eye remains virtually constant during/following contusion because the aqueous outflow facility cannot adjust rapidly enough to the sudden volume displacement.
• Compression of one part of the globe therefore effectively means that a corresponding volume of fluid must be displaced elsewhere within this closed system.
• This sudden violent change in shape without a corresponding change in volume generates tractional forces within the globe. This discrepancy can be extremely destructive to ocular tissues.
• All these factors conspire to make the posterior segment particularly susceptible to a contusive insult.
MANAGEMENT In most instances, traumatic retinal tears should be treated with laser retinopexy or, less prefereably, cryoretinopexy. Holes that have undergone spontaneous closure due to chorioretinal adhesion can be observed but should be followed closely to detect possible progression to retinal detachment.
CONTROVERSY
A giant retinal tear, even in the absence of retinal detachment, may require a prophylactic scleral buckle as a reasonable alternative to retinopexy because of the associated vitreous traction and risk of PVR development.
The risk of progression to retinal detachment is too great in contused eyes with retinal breaks outside the fovea; therefore, prophylactic treatment should at least be considered for all of these eyes.
Traumatic Rhegmatogenous Retinal Detachment is the most common cause of permanent visual loss.
CLINICAL FEATURES Trauma accounts for up to 12% of rhegmatogenous retinal detachments and remains the most common cause of detachments in children.72,73
Traumatic retinal detachment may occur secondary to:
• retinal dialysis;
• flap/horseshoe tears;
• giant retinal tears;
• full-thickness retinal necrosis; or
• stretch tears.
PEARL… With the exception of giant retinal tears as the cause, traumatic retinal detachments in general tend to progress slowly.4,65 This is particularly true if a formed vitreous is present.
Retinal detachments secondary to peripheral retinal tears tend to progress more quickly than those due to retinal dialysis, which can sometimes take years to develop or to become symptomatic. Consequently, if considerable time elapses between injury and presentation, differentiation of this type of retinal detachment from nontraumatic types may be difficult. A search for other signs of trauma, especially if unilateral, may be particularly rewarding in unraveling the precise etiology.
The symptoms of traumatic rhegmatogenous retinal detachment are similar to those associated with rhegmatogenous retinal detachment in nontraumatic settings; they range from:
• floaters and
• photopsia to
• progressive visual field loss and eventual
• loss of central vision from macular involvement.
In some cases, presentation may be delayed until the retinal detachment involves the macula and causes decreased visual acuity.
PEARL… Delayed presentation typ-ically occurs for retinal detachments following retinal dialysis, evolving over several months or even years.
In eyes with a slowly developing retinal detachment, the examination may reveal:
• progressive “high or tide water marks” beneath the detached retina;
• a retina that is thin/atrophic; and
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


